Narrative Descriptive Reports on Public Health Impact of Conflict among War-Affected Zones at Amhara Region, 2022
Introduction: Armed conflicts result in the interruption of clinical services, public health services, and other health-related programs and damage to the health facilities and their infrastructures. Objective: This study aimed to assess the impact of conflict on public health within the war-affected zones of the Amhara region. Method: a descriptive cross-sectional study was conducted in the Amhara region. Document review and interview administered questionnaires were employed for collecting the data during the study period. Result: Based on this assessment; more than 51% of health facilities and their infrastructures were damaged and looted. About 10,333 patients on chronic disease follow-up had interrupted their treatment and follow-up for more than three to six months. And also, more than 29632 civilians died in the conflict-sourced war. Maternal and child health services have been interrupted for more than70, 000 pregnant & lactating mothers. 1035 unwanted pregnancies and 934 sexual gender-based violence (SGBV) have been occurred due to the conflict. Conclusion: About 51% of health facilities in the region were damaged; following this essential health services such as chronic follow non-communicable and chronic infectious disease, maternal health services, and child health services have been interrupted in the affected zones. This had led to the occurrence of maternal mortality of 233 &child mortality of 166 among those who lived in the affected area. Therefore, it needs Rapid strengthening of mobile health services, and the reestablishment of health facilities buildings and their infrastructures to reduce future morbidity and mortality.
Introduction
Conflict is actual or perceived need value belief and interest between two or more states. And in political science conflict mean war or revolution which may use force which is called armed conflict. Armed conflicts within States are political conflicts involving citizens fighting for internal change. Most armed conflicts are fought not only by regular armies but also by militias and armed civilians with a little discipline and ill-defined chains of command [1]. Armed conflicts present a multitude of risk factors that enhance disease emergence and transmission, especially in poor countries Conflicts and wars, a commonplace in today’s world have left populations in dire poverty, displaced people from their homes, and deprived them of having access to essential services and made people vulnerable to various diseases. Detection and control of diseases in conflict- affected regions is an arduous task because of multiple risk factors that promote disease transmission and hinder control in many poor-resource settings [1, 2]. Detection and control of diseases in conflict-affected regions is an arduous task because of multiple risk factors that promote disease transmission and hinder control in many poor-resource settings. Conflict is the ultimate social determinant of health, and conflict-affected countries are lagging. More and more people are being forcibly displaced inside their own countries, while still others attempt to cross into neighboring countries and beyond [1, 3].
The public health impact of a crisis ranges from both direct (injury or death from the crisis itself) to indirect (changes in living conditions, forced displacement, lack of legal protection or decreased access to health care). Based on the situation reports from the health sector, these humanitarian crises resulted in a significant impact on the health and well-being of affected populations. The social support and interactions have also been interpreted in these areas which can create panic and anxiety in the affected community [4]. Conflicts arising due to violent differences between two opposing groups or individuals present a multitude of risk factors that enhance disease emergence and transmission, especially in poor countries. Conflicts and wars are commonplace in today’s world have left populations in direct poverty, displaced people from their homes and deprived them of having access to essential services, and made people vulnerable to various diseases. It is one of the most common disasters and a global health issue. Long-lasting and protracted conflicts in particular have consequences not only for the war-wounded but also for the health of entire communities [1, 5]. In recent years Ethiopia has also one of the victims of conflict with TPLF and other armed forces. So, conflict is one of the most common disasters in Ethiopia including in the Amhara region and its respective zones. Even if the government of Ethiopia has taken different interventions the disaster of conflict is now away from a serious problem in the Amhara region from different directions. And it results in acritical public health impacts. Despite this, the regional disaster risk management early warning and preparedness and mitigation intervention are very weak and too limited Notification and supporting letters were written to the department of Amhara public health institute. Give clear information about the participants. Participants have the right to give their opinion, the right to withdraw, and refuse the interview at any time. In addition, written informed consent was also requested for their readiness to participate during the data collection period.
Method and Material
Study Area
This study was conducted in the Amhara region. Bahir dar is the capital city of the Amhara region found 450 km from the capital city of Addis Ababa. The region has a total of 15 zones including the city administration. Among this zone nine [6] of them were affected by the conflicts between the two regions. The region has a total population of 22000170 from this 11005000 are male the rest are female. The region has a total of 876 health centers, 87 hospitals, and 16000 health posts.
Study Design
The descriptive cross-sectional design was employed during the study period.
Sampling Procedure
Purposive sampling methods were employed.
Data Collection Method
The data has been collected by using documented review of secondary data from the regional health bureau and observation of some primary data at the affected sites. The tool was used for the data extraction checklist.
Ethical Clearance
Notification and supporting letters were written to the department of Amhara public health institute. Give clear information about the participants. Participants have the right to give their opinion, the right to withdraw, and refuse the interview at any time. In addition, written informed consent was also requested for their readiness to participate during the data collection period.
Result
The TPLF invasion of the Amhara region starts on July 10/2013 and scaleup up to many zones and districts of the Amhara region within a short period Following this conflict different public health emergency responses at different times at different phases have been cascaded. Regional disaster risk management situation: there is a leading sector of disaster risk management at the regional level in the form of a disaster risk management office. with a role in disaster prediction, data analysis, interpretation, and result dissemination, in addition, to organizing the responsible stakeholders before and after the occurrence of an emergency and emergency preparedness and readiness plan within the participation of members of the leading sectors such as health, agriculture, water and security. Early warning and preparedness: Though there were some clues about the Tigray invasion since October 24/ 2013 EFY; there is no documented and organized risk prediction, analysis, evidenced preparedness plan, or emergency preparedness plan concerning conflict and other disasters except drought and flood. Even if no risk mapping and prediction when the conflict starts; some evacuation, readiness to relief response, and collective site selection had been done some weeks before the risked area was invaded. In addition to human evacuation, there were some medical supplies, medical equipment, and other materials have been evacuated. The Ethiopian pharmaceutical supply agency (EPSA) evacuated a supply and medical equipment which cost 227million birr from eastern Amhara EPSA, and the Regional health bureau has been evacuated ambulances which cost 3 billion ETB. As evidenced by the regional health bureau report, especially from the north wall, south wollo, and North Shewa.
Emergency public health response: Even if it was weak and non-resilient there have been established technical working groups (TWG), Taskforce, and rapid response teams (RRT) as a region that can provide different relief tasks during an emergency of conflict. As a result, 37 collective sites were selected and responsible TWG and task force were assigned at all levels for providing different services such as food distribution (984,000ton) shelter establishment (234,0000), finical empowerment (168,234,345ETB), and sanitary equipment such as soap, detergent, blench (2,134.654psc), modes (454,000pcks), different cooking materials which cost (1256712ETB), lancets (689,000), and maters and (534238 pcs) have been distributed. As a region, a total of 132,865,123(ETB) have been allocated for purchasing drugs, medical equipment, and other supplies. About 452 additional health professionals have been employed for the mobile clinic to do different tasks such as nutritional screening, vaccination, health education, gender-based violence (GBV) screening and linking to treatment, and follow-up for chronic follow-up (Table 1).
| Types of disease | Number of patients |
|---|---|
| Diarrheal disease | 34234 |
| Upper respiratory tract infection | 28986 |
| dyspepsia | 678 |
| helminthiasis | 27668 |
| scabies | 22,456 |
| injuries | 18845 |
| pneumonia | 14786 |
| Fungal infection | 16798 |
| Mental health | 3456 |
| Diabetes mellitus | 268 |
| hypertension | 167 |
| HIV/AIDS | 432 |
| TB | 89 |
Table 1: Clinical services delivery for different disease categories in the last six months at different internal displacement si
Damage to Health Facilities and their Infrastructure due to Tigray Conflict in the Amhara Region
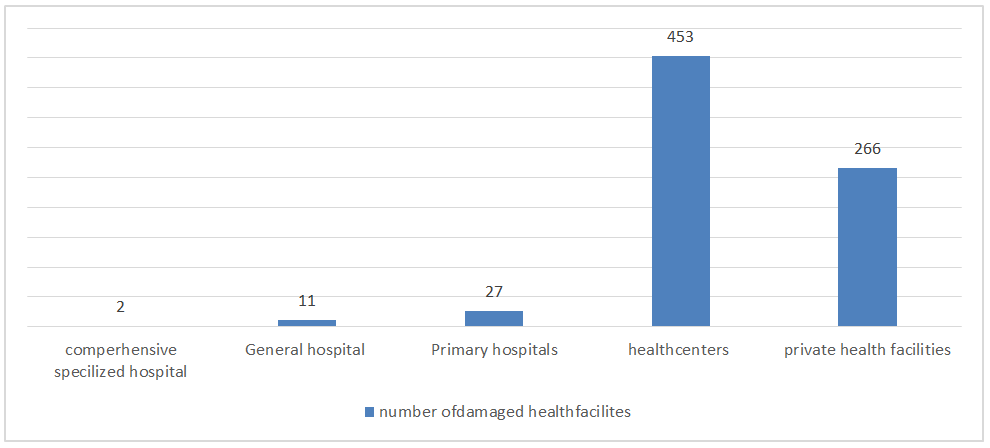
TPLF-led invasion and terrorist attacks destroyed health system infrastructures partially or completely, pillaging medical supplies and equipment, and interruptions of health services, leaving the community reliant on emergency medical assistance. Because in less than six months of the war, health facilities including 2 comprehensive specialized hospitals (Dessie and Woldia Comprehensive specialized hospitals, 11 general hospitals, 27 primary hospitals, and 453 health centers were affected during the war period (Figure 1).
List of the Damaged Building Health Centers, Hospitals, and Substructures of the Building during the Conflict Period
Medical equipment damaged and lost/stolen by the TPLF conflict and the estimated cost. The table below indicates the medical equipment damaged in each health facility and the estimated cost. From the two affected comprehensive specialized hospitals, the medical equipment was damaged and its estimated cost was (41273677.12ETB), from 11 general hospitals the estimated cost was (134,190,966.69) and from27 primary hospitals medical equipment was lost and its estimated cost were (169,559,774.82) (Table 2).
| S.no | Different Categories of Health Facilities | Number of Health Facilities whose Medical Equipment was Looted and Damaged | Total Cost (ETB) |
|---|---|---|---|
| 1 | CSH | 2 | 41,273,677.12 |
| 2 | General hospitals | 11 | 134,190,966.69 |
| 3 | Primary hospital | 27 | 169,559,774.82 |
| 4 | Health center | 453 | 1,167,848,396.34 |
| Total | 453 | 1,512,872,814.97ETB |
Table 2: List of the damaged building of health centers, hospitals, and substructures of the building during the conflict period,
The Chronic Disease Follows up Patients during the Conflict Period
Chronic follow-up patients whose treatment and follow up interrupted by TPLF conflict for six months in the affected zones of the Amhara region, 2022. A total of 8915 patients with chronic follow-up for chronic infectious diseases such as TB, HIV, and leprosy have been interrupted their monthly treatment and clinical follow-up (Table 3).
| Zones | TB cases | MDR TB | Leprosy | HIV/AIDS | Remarks |
|---|---|---|---|---|---|
| North Gondar | 163 | 11 | 25 | 112 | |
| North Wollo | 382 | 16 | 42 | 1100 | |
| Wag Himera | 118 | 9 | 19 | 540 | |
| Dessie city | 86 | 26 | 11 | 1067 | |
| North Shewa | 291 | 29 | 95 | 861 | |
| Oromo special zone | 178 | 3 | 27 | 1311 | |
| South Gondar | 31 | 1 | 3 | 324 | |
| South Wollo | 542 | 8 | 190 | 1260 | |
| West Gondar | 49 | 9 | 76 | 123 |
Table 3: Showed that Chronic disease follow up patients during the conflict period.
Maternal and Child Health Services In War- Affected Zones of the Amhara Region during the Conflict Period
During the time of the war in the affected Amhara region there are 74980 home delivery, 91 unsafe abortions, 45980 lost post-natal care, 33 maternal mortality,66 neonatal death, and 137698 interrupted family planning method, and 1035 unwanted pregnancy happened during the conflict period (Table 4).
| Zones | Home delivery | Unsafe abortion occurred | Post- natal care lost | Maternal mortality | Neonatal death | Family planning user interrupted | Unwanted pregnancy |
|---|---|---|---|---|---|---|---|
| North Gondar | 1363 | 0 | 363 | 2 | 1 | 8112 | 38 |
| North Wollo | 28822 | 16 | 8822 | 9 | 6 | 45100 | 343 |
| Wag Himera | 2118 | 9 | 2118 | 5 | 4 | 2540 | 168 |
| Dessie city | 2986 | 12 | 2986 | 3 | 3 | 34067 | 123 |
| North Shewa | 2291 | 22 | 291 | 2 | 22 | 9861 | 0 |
| Oromo special zone | 6178 | 3 | 178 | 0 | 0 | 1311 | 87 |
| South Gondar | 5331 | 1 | 5331 | 3 | 3 | 3324 | 86 |
| South Wollo | 23542 | 29 | 23542 | 8 | 27 | 31260 | 178 |
| West Gondar | 2349 | 9 | 2349 | 1 | 0 | 2123 | 12 |
| Total | 74980 | 91 | 45980 | 33 | 66 | 137698 | 1035 |
Table 4: showed that Maternal and child health services in war-affected zones of the Amhara region during the conflict period.
Discussion
This study was conducted to describe the public health impact of the TPLF war in the Amhara region. And the study included all affected zones of the region. Because the war in the Amhara region of Ethiopia by Tigrayan has started on Oct. 2021. It has brought enormous damage to the health system. And this assessment aimed to describe the occurrence of public health impact following the Tigray people liberation front (TPLF) conflict in the Amhara region of the nine affected zones. Due to this conflict within a short period; 45% of hospitals among hospitals in the region and 51.7% of health centers among total health centers of the region were damaged. Overall, 51% of government health facilities were damaged and looted. This resulted from morethan16 million people suffering due to a lack of any type of health services for more than three months and this has resulted in the occurrence of too many communicable and non- communicable diseases incidence. In general, the war altered both rates of change and absolute health outcomes for the worse which is supported in the study conducted in Sri Lanka [3]. If there were strong early warnings and alerts by the regional DRM and national DRM there was a probability of reducing the damage to the health system [1]. However, the limited capacity of the DRM created an opportunity for the TPLF to deliberate destruction, vandalization, and looting of the entire health system in the affected zones of the region. This is in line with a study conducted in sub-Saharan Africa [6].
This war had great public health and economic loss. In the affected health facilities, different types of medical equipment were destroyed, looted, and stolen.it results from a loss of medical equipment which has an estimated cost of
1,512,872,814.97 ETB based on the previously purchased estimate. This results from a need for an estimated budget of 19,634,779,165 ETB to recover and rehabilitate. This economic cost lowers the region as well as the country’s GDP not only this it has substantial effects on both the revenue and expenditure sides of a country’s public finances. This is in line with other studies conducted in sub-Saharan Africa on the economic impact of conflict [7]. Following the conflict women and children who lived in affected zones have lost essential health services. Some of the essential health services included; home delivery (74980), women were lost post- natal care (74,981), women lacking family planning services (137698), women faced unsafe abortion (91), unwanted pregnancy (735), pregnant women were lack ANC1st follows up (96789), about 17,764 pregnant or lactating women have been screened for malnutrition and 3,966 (22.3, gender-based violence (234), severe acute malnourished under five years children 27.7% (13,479) and moderate acute malnutrition 59.4% (16,963). This will result from an intergenerational effect on physiological growth and development; especially in children with malnutrition conditions throughout their lifetime. because household food insecurity is an important factor contributing to poor nutritional status among children during conflict and is associated with the risk of stunting and underweight in children and this has direct negative consequences in terms of disease and disability, brain development, educational attainment and income potential for individuals and communities [8, 9]. Antenatal care for pregnant women is the most valuable maternal health service which helps to reduce maternal mortality by 42% [3]. In general neglecting essential maternal health services during the optimal period will increase the maternal mortality and morbidity alarmingly which is in line with a study conducted at Sub-Saharan Africa [6].
Concerning chronic infectious disease treatment and follow-up; in the war-affected zones of the region, a total of TB (1840), MDR TB (91), leprosy (409), and HIV/AIDS (6698) cases have had treatment and monthly follow up interruption respectively. The treatment and follow-up interruption of infectious diseases especially HIV/AIDS implies an increased risk of death, opportunistic infections, virologic failure, resistance development, and poor immunological recovery among patients those who started and interrupted the follow- up and treatment supported by the study conducted [10, 11]. Based on the major NCD of diabetes mellitus hypertension and mental health problem more than 5041, 5292 and 659 cases were interrupted their follow-up and treatment for three to six months respectively. Discontinue the use of anti- hypertensive have three times higher risk of cardiovascular mortality. In addition to this worsening of the current disease condition; increased uncontrolled hypertension, increases morbidity and mortality secondary to NCD in conflict-affected areas. This implication was supported by other studies conducted in Brazil and Ethiopia [12].
Limitations of this Study
This study design uses secondary data so it has its own limitation of completeness and personal bias.
Conclusion
The displacement of healthcare manpower and damaged infrastructure will have a long-lasting consequence in rehabilitating the healthcare system of the region once. More than 50% of the region’s health facilities were damaged and looted. And it needs more than 9 billion of the estimated cost to do recovering the basic health services on behalf of reconstructing and maintaining the demolished health facilities. Furthermore, the widespread use of rape and sexual harassment as a systemic weapon of the war. And too many chronic infectious disease patients interrupted their treatment and follow-up for more than six months. Therefore, it needs reestablishment of building and furnishing of all types of damaged health facilities. And designing comprehensive chronic follow-up patient tracing and relinking mechanisms and especially providing ongoing clinical evaluation. in addition to this providing comprehensive capacity building for the regional disaster risk management in case of risk assessment and early warning which is supported by advanced technology.
Declaration
Ethics Approval and Consent to Participate
Notification and supporting letters were written to the Wollo University, College of Health Science and Medicine. Give clear information about the participants. Participants have the right to give their opinion OF n, the right to withdraw, and refuse the interview at any time. In addition, written informed consent was also requested for their readiness to participate during the data collection period.
Authors Contributions
All authors made significant contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit it to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgment
We would like to thank the Amhara health bureau and Amhara zone, each Woreda health facility affected by the war for giving us clear and precise information about this research. We are also grateful to all those participating in the data collection process.
References
-
Nayak DN, Solanki JB, Patel DC, Moliya DC (2019) Effect of human war and conflict on public healthcare. IJSET 8(6): 1114-1119.
-
Devakumar D (2014) Conflict and health. Med Confl Surviv 30(3): 213-214.
-
Johnson SA (2017) The Cost of War on Public Health: An exploratory method for understanding the impact of conflict on public health in Sri Lanka. PLoS One 12(1): e0166674.
-
Devkota B, Teijlingen VER (2010) Understanding effects of armed conflict on health outcomes: The case of Nepal. Confl Health 4(1): 1-8.
-
Debarre A (2018) Hard to Reach: Providing Healthcare in Armed Conflict. IPI pp: 1-40.
-
Oladayo NA (2019) The impact of conflict on health outcomes: systematic evidence from sub-Saharan Africa. Mgbakoigba J African Stud 8(1): 88-100.
-
Fang X, Kothari S, Mcloughlin C, Yenice M (2020) The economic consequences of conflicts in Sub-saharan Africa. IMF pp: 1-29.
-
Carroll GJ, Lama SD, Brockman JLM, Escamilla RP (2017) Evaluation of nutrition interventions in children in conflict zones: A narrative review. Adv Nutr 8(5): 770-
-
European Parliament (2014) The social and economic consequences of malnutrition in ACP countries. Backgr Doc.
-
Kranzer K, Ford N (2011) Unstructured treatment interruption of antiretroviral therapy in clinical practice : a systematic review 16(10): 1297-1313.
-
Leite MLC, Firmo JOA, Filho AIL, Costa MFL (2014) Discontinuation of anti-hypertensive drugs increases 11-year cardiovascular mortality risk in the community- dwelling elderly (the Bambuí Cohort Study of Ageing). BMC Public Health 14: 725.
-
Cramer BG, Summers A, Cardozo BL, Husain F, Couture A, et al. (2020) Noncommunicable disease burden among conflict-affected adults in Ukraine: A cross-sectional study of prevalence, risk factors, and effect of conflict on severity of disease and access to care. PLoS One 15(4): e0231899.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’