A Comparative Study of Neonatal Outcome in Early-Term Neonates versus Full-Term Neonates in a Tertiary Care Hospital in North India
Background: Neonatal morbidity due to physiologic immaturity has been extensively studied in preterm infants delivered in less than 37 weeks gestation. However, evidence indicates that the infants delivered between 37+0 and 38+6 weeks gestation are also at increased risk for morbidity compared with the infants delivered at 39+0 to 40+6 weeks. Methodology: The present hospital-based prospective observational study was conducted among 150 neonates [75 babies each of early term (37+0 to 38+6 weeks) and full term (39+0 to 40+6 weeks)], born to consenting mothers in a tertiary care referral and teaching hospital, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly. Apart from maternal demographic and obstetric factors, features of the newborn - APGAR score at 1 & 5 minutes, admission to NICU, and other morbidity indicators such as respiratory distress, hyperbilirubinemia, neonatal sepsis, and prolonged hospital stay (>7 days), etc were recorded and compared. SPSS v21.0 was used for statistical analysis. Results: The mean age of mothers was 25.27+3.93 years (age range 19-40 years). Early term deliveries were common among older age groups, and full term among younger ones. Full term neonates had a higher APGAR 1-minute score than early term (p = 0.049), but this difference was not significant at 5-minute score (p > 0.05). NICU admission, respiratory distress and jaundice were more common among early term as compared to full term neonates (*p < 0.05). Conclusion: Early term neonates have a significantly higher morbidity and distress as compared to full term neonates. Studies are recommended to develop strategies to reduce early delivery of high-risk pregnancies.
Introduction
Neonatal morbidity due to physiologic immaturity has been extensively studied in preterm infants delivered in less than 37 weeks gestation [1]. Evidence indicates that neonatal morbidity decreases with delivery at later gestational ages, nevertheless, the infants delivered between 37+0 and 38+6 weeks gestation are at increased risk for morbidity as compared with the infants delivered at 39+0 to 40+6 weeks [2, 3]. Specifically, rates of respiratory distress syndrome, transient tachypnea of the newborn, pneumonia, hypothermia, feeding difficulties, as well as long-term childhood morbidities including increased risk of problems with school performance and behavior, increased hospital admission up to 5 years of age, asthma, and wheezing are increased in infants born at 37 to 38 weeks compared with infants born after 38 weeks [4]. The American College of Obstetrics and Gynecology has thus recommended designating 37+0 to 38+6 completed weeks’ gestation as “early term” and 39+0 to 40+6 weeks’ gestation as “full term” [5]. Both the reason and gestational age at delivery are likely important factors contributing to morbidity, as neonatal morbidity has been found to vary depending on the underlying indication for delivery [6]. Although early term babies are a category known for its high mortality and diverse morbidities, the overall incidence of prematurity related complications decreases significantly with increasing gestational age.
In the Indian setting, there has been a paucity of data regarding whether increased morbidity in early term neonates is a consequence of physiologic immaturity at earlier gestation or because of the underlying precursor leading to early term delivery. Hence, this study was carried out with a goal to compare the differences in morbidity and mortality as neonatal outcome among early and full-term neonates in a tertiary care hospital in North India.
Methodology
This prospective hospital-based observational study was conducted among all neonates born to mothers presenting to the Department of Obstetrics and Gynaecology in a tertiary care referral and teaching hospital, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly (UP) India, over a period of one and half year (Nov 2019 to May 2021). A total of 150 neonates (75 babies with gestational age 37+0 weeks to 38+6 weeks, termed as “Early term”- Group A; and 75 babies with gestational age 39+0 weeks to 40+6 weeks, termed as “Full term”- Group B) born to mothers consenting to participate were included in the study. All patients were subsequently followed up till the neonate was discharged from the hospital [7]. However, preterm babies born <37 weeks gestational age, babies with associated congenital anomalies, fetal growth restriction, maternal medical illness like Diabetes Mellitus and H/o preeclampsia, patients with bleeding disorders and immunocompromised patients were excluded from the study. Sample selection was done using convenience sampling method (first come first serve basis) for the study. Ethical Approval was taken from the Institutional Ethical Committee prior to initiation of the study. A written informed consent was obtained from each mother/guardian before clinical examination as well as data collection. The involvement of the subject was voluntary and deliberate.
Maternal demographic and obstetric factors and features of the newborn like sex, gestational age (GA), birth weight (BW), maternal age and mode of delivery were recorded. The primary outcome measured among neonates was: a) APGAR score at 1 minute and 5 minutes, and b) birth weight. The secondary outcome measures of the study included respiratory distress, NICU admission, hyperbilirubinemia requiring phototherapy, neonatal sepsis, hypoglycaemia, feeding difficulties, dehydration, and prolonged hospital stay (>7 days). The two study groups were compared on the basis of parameters like APGAR score, NICU admission, respiratory distress, jaundice, sepsis, hypoglycaemia, feeding difficulties and dehydration and duration of hospital stay. Statistical analysis was performed using SPSS (Statistical Package for the Social Sciences) for Windows (version 24.0). Categorical variables were described as frequency (percentage), mean ± standard deviation was used for continuous parameters. For non-parametric variables, the data are presented as median (min-max). For all analyses, a two-tailed p-value of <0.05 was considered statistically significant.
Observations
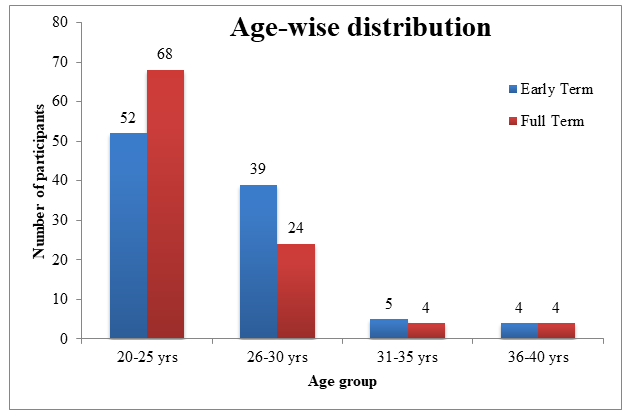
The results showed that the mean age of mothers was 25.27+3.93 years (range 20-40 years). Majority of mothers (60%) were young (19-25 years), followed by 31% among mothers aged 26-30 years, and the rest of the age groups had 9% subjects. A significant difference was observed in age distribution among early and full term infants. Early term deliveries were more common among older age groups, and full-term pregnancies were more common among younger age groups (p=0.041*) (Table 1 & Figure 1)
- Age distribution
- “Group A”
- “Group B” p-value
- N
- %
- N
- %
- 20-25 yrs.
- 39
- 52
- 51
- 68
- 0.041*
- 26-30 yrs.
- 29
- 39
- 18
- 24
- 0.003*
- 31-35 yrs.
- 4
- 5
- 3
- 4
- 0.552
- 36-40 yrs.
- 3
- 4
- 3
- 4
- 1
Table 1: Age wise distribution of mothers of study population.
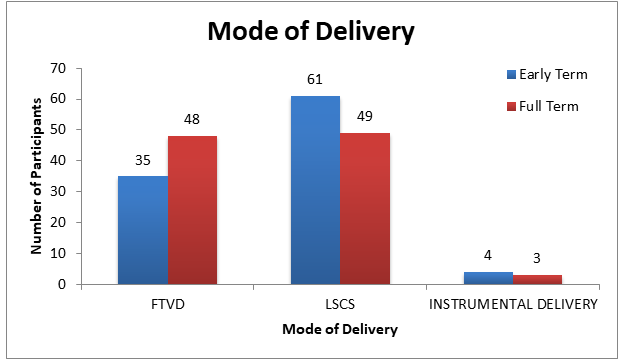
- Regarding the mode of delivery, majority of mothers underwent a LSCS delivery (61%), followed by vaginal delivery (35%) in early-term group. However, 49% of the mothers in full-term group underwent a LSCS delivery,
- Clinical parameters
- “Group A”
- “Group B” p-value
- N
- %
- N
- %
- FTVD
- 26
- 35
- 36
- 48
- 0.031*
- LSCS
- 46
- 61
- 37
- 49
- 0.017*
- Mode of delivery
- Instrumental
- 3
- 4
- 2
- 3
- 0.633
- Total
- 75
- 100
- 75
- 100
Table 2: Mode of delivery of mothers of study population.
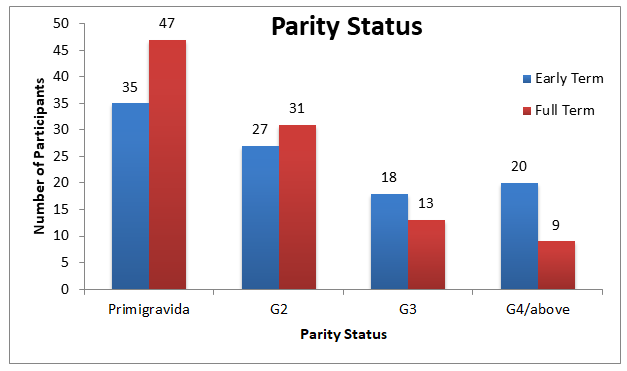
The difference in parity it was significant for multigravidas with 4th pregnancy & above between mothers having early term versus full term neonate was statistically significant in the present study. (p=0.045*) (Table 3 & Figure 3).
- Parity
- “Group A”
- “Group B” p-value
- N
- %
- N
- %
- Primigravida
- 26
- 35
- 35
- 47
- 0.821
- G2
- 20
- 27
- 23
- 31
- 0.992
- G3
- 14
- 18
- 10
- 13
- 0.529
- G4/above
- 15
- 20
- 7
- 9
- 0.045*
- Total
- 75
- 100
- 75
- 100
Table 3: Parity status of mothers of study population.
There was a similar observation in APGAR scores, full term babies had a significantly higher APGAR score at one-minute than early term neonates (p= 0.049*), but this difference was not significant at five-minute APGAR score (p > 0.05) (Table 4).
| Birth weight (kg) | Group A | Group B | P-value | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| < 2.5 kg | 10 | 13 | 3 | 4 | 0.739 |
| 2.5-3 kg | 43 | 57 | 48 | 64 | 0.122 |
| 3-3.5 kg | 18 | 25 | 17 | 23 | 0.851 |
| APGAR score at 1 min | |||||
| >7 | 64 | 85 | 71 | 95 | 0.041* |
| <7 | 11 | 15 | 4 | 5 | 0.002* |
| APGAR score at 5 mins | |||||
| >7 | 73 | 97 | 75 | 100 | 0.848 |
| <7 | 2 | 3 | 0 | 0 | 0.955 |
Table 4: Comparison of primary outcome variables among study participants.
Birth weight too, was not significantly associated with early-term and full term (p > 0.05). NICU admission was more significantly common among early term as compared to full term group (p=0.024*) (Table 5).
Regarding secondary outcome measures, respiratory distress (p=0.02*) and incidence of jaundice was more common among early term as compared to full term group (p < 0.046*) (Table 5). However, occurrence of sepsis,
- hypoglycemia (RBS <45 mg/dl), any feeding difficulties, and dehydration was similar across both study groups (p > 0.05).
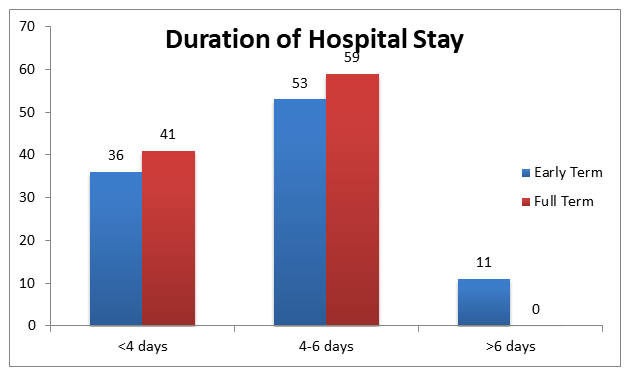
- In Group A most of the neonates had a hospital stay of
- 4-6 days (53%), followed by less than 4 days (36%) and >6 days (11%). However, In Group B, majority of the neonates had a hospital stay of 4-6 days (59%), followed by less than
- 4 days (41%). This difference was statistically not significant
- (p > 0.05) (Table 6 & Figure 4)
- Duration of hospital stay
- “Group A”
- “Group B” p-value
- N
- %
- N
- %
- <4 days
- 27
- 36
- 31
- 41
- 0.087
- 4-6 days
- 40
- 53
- 44
- 59
- 0.133
- >6 days
- 8
- 11
- 0
- 0
- 0.000*
- Total
- 75
- 100
- 75
- 100
Table 5: Comparison of duration of hospital stay None in group ‘B’ had hospital stay more than 6 days as compared to group ‘A’
| Variables | Group A | Group B | P-value | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Respiratory Distress | 11 | 15 | 2 | 3 | 0.002* |
| NICU Admission | 11 | 15 | 3 | 4 | 0.024* |
| Jaundice | 15 | 20 | 5 | 7 | 0.046* |
| Sepsis | 2 | 3 | 1 | 1 | 0.828 |
| Hypoglycemia | 3 | 4 | 1 | 1 | 0.671 |
| Feeding Difficulties | 12 | 16 | 7 | 9 | 0.074 |
| Dehydration | 0 | 0 | 1 | 1 | 0.672 |
Table 6: Comparison of duration of hospital stay None in group ‘B’ had hospital stay more than 6 days as compared to group ‘A’ in
Discussion
Most research on neonatal outcomes is centered on babies born as early preterm (<34 weeks), as they are considered as high-risk group for mortality and serious morbidity. But increasing awareness of the clinical risk and morbidities of early term babies prompted further investigation and research studies among this particular group. In the present study, early term deliveries were more common in older age categories (26-30 years) and full term deliveries in younger ages (20-25 years). This finding was in contrast to another study by Sengupta S, et al. [8], wherein the age difference between mothers of early term and full- term neonates was almost matching.
Parikh LJ, et al. [9] in their retrospective study of records of nearly 2 lakh mothers showed an increased risk for early term birth with increasing orders of parity. Another study by Noli, et al. [10] supports the above-mentioned finding. A large-scale study is therefore warranted to determine the influence of parity in gestational age at birth. Regarding the mode of delivery, almost every study in the literature supports the fact that LSCS mode of delivery was more common among early term neonate as compared to full term [8, 10]. The present study too, showed a similar pattern, the difference was statistically significant (p=0.017*).Study conducted by Sengupta S, et al. [8] showed a non-significant difference between LSCS and Vaginal deliveries between both study groups, which is in contrast to the present study [8]. Significantly more early term infants were delivered by cesarean section compared with full term infants, which is a contributor to longer duration of hospital stay and higher levels of morbidity. (p=0.031)* Studies by Bailit JL, et al. and Clark SL, et al. [11, 12] have focused on mode of delivery as a cause of morbidity in full term neonates. It is well established that cesarean section delivery, especially in the absence of labor, is a strong predictor of neonatal morbidity. Evidence states that low APGAR score, defined as less than 7, is associated with an increased risk of neonatal death among full term infants (≥37 weeks). Low APGAR scores are associated with increased neonatal morbidity and mortality in early term neonates. Asphyxia related complications, neonatal hypoglycemia and respiratory distress were strongly associated with APGAR scores of 7 and 8. It has been reported that among full term infants with 5-minute APGAR scores in the normal range (7 to 10), the risk of neonatal death was higher among those with a score of 7 or 8 than among those with a score of 9 or 10 [13]. The frequency of low APGAR scores increases with decreasing gestational age and may reflect biologic immaturity in early term infants. Also, NICU admission rates were significantly higher among early term as compared to full term. NICU admission was present in 15% of early term neonates as compared to 4% among full term neonates. Study conducted by Tiwari SK, et al. [14] have indicated that early term birth have higher levels of morbidity and distress leading to frequent NICU admissions, which is concurrent with our study.
Regarding secondary outcome variables, various studies have similarly reported higher rates of morbidities among early term neonates compared to full term. Another study by Wilcox AJ, et al. reported [15] a three times higher risk for overall morbidity due to any cause, 3.8 times higher risk for respiratory morbidity, and 3 times higher risk of hypoglycemia & any infection. A study from Singapore Seikku L, et al. [16] reported 7 times higher risk for RDS,
17 times higher risk of hypoglycemia and 7.8 times risk of hypothermia. Although neonatal morbidity was lower during the full-term period, benefits of delivery during the full-term period must be weighed against the risk of still birth. Longitudinal data is necessary to determine the optimal balance of neonatal morbidity vs risk of still birth and perinatal mortality at 38 or 39 weeks gestation. Information on neonatal outcomes based on the conditions leading to delivery is useful for patient counseling when discussing the risks and benefits of early term delivery. Our results showed that early term birth had significantly higher incidence of respiratory distress. Respiratory distress was present in 15% of early term neonates as compared to 3% in full term neonates. This is in concordance with the study done by Ghartey, et al. [17]. The immature lung structure present before full term may be associated functionally with delayed intrapulmonary fluid absorption surfactant insufficiency, and insufficient gas exchange leading to TTNB and RDS. Also, it was observed that none of the morbidity variables had a statistically significant association with the duration of hospital stay in the present study. This is in concordance with another study by Bates, et al. [18], which showed similar increased adverse neonatal outcomes in early term births.
The major strength of our study was the ability to analyze the morbidity and distress conditions leading to final neonatal outcome that enabled us to determine the reasons for increase in neonatal morbidity. Neonatal morbidity was lowest at or beyond 39 weeks gestational age and was significantly lower compared with 37 weeks gestation.
Limitations of the Study
The main limitation of the study is the small sample size and short-term follow-up period of neonates till discharge from the hospital. Long term follow-up in the form of language delay, attention deficits, intelligence or behavioral problems, developmental disability and academic achievement issues among these neonates later-on should also be considered.
Conclusion
Information on neonatal outcomes based on the conditions leading to delivery is useful for patient counseling while discussing the risks and benefits of early term delivery. For uncomplicated singleton pregnancies, our data support the recent American College of Obstetrics and Gynecology Committee Opinion of waiting until 39 weeks’ gestation for delivery, as there was clearly increased neonatal morbidity during the early term period. Early term babies delivered prior to 39 weeks of gestation had increased neonatal morbidities when compared with full term babies. The result of this study emphasizes the importance of discouraging non-indicated delivery before 39 weeks of gestation. It is conclusive that early term neonates have a significantly higher morbidity and respiratory distress as compared to full term neonates. Further studies are recommended to develop strategies to reduce early delivery of high-risk pregnancies to decrease incidence of early term births and reduce perinatal morbidities.
References
-
Laughon SK, Reddy UM, Sun L, Zhang J (2010) Precursors for late preterm birth in singleton gestations. Obstet Gynecol 116(5): 1047-1055.
-
Spong CY, Mercer BM, Alton MD, Kilpatrick S, Blackwell S, et al. (2011) Timing of Indicated Late-Preterm and Early-Term Birth. Obstet Gynecol 118(2 pt 1): 323-333.
-
Reddy UM, Bettegowda VR, Dias T, KushnirTY, Ko CW, et al. (2011) Term pregnancy: a period of heterogeneous risk for infant mortality. Ostet Gynecol 117(6): 1279- 1287.
-
Hourani M, Ziede F, Rajab M (2011) Timing of planned caesarean section and the morbidities of the newborn. N Am J Med Sci 3(10): 465-468.
-
(2013) ACOG committee opinion no. 561: Nonmedically indicated early-term deliveries. Obstet Gynecol 121(4): 911-915.
-
Tita ATN, Landon MB, Spong CY, Lai Y, Leveno KJ, et al. (2009) Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med 360(2): 111- 120.
-
Kambiakdik T, Leelalanslat AD, Sohi I, Varkey VP (2018) Maternal risk factors and early neonatal outcome among late preterm and term neonates in a Neonatal Intensive Care Unit in Punjab, India. Int J Contemp Pediatr 5(2): 612-616.
-
Sengupta S, Carrion V, Shelton J, Wynn RJ, Ryan RM, et al. (2013) Adverse Neonatal Outcomes Associated With Early-Term Birth. JAMA Pediatr 167(11): 1053-1059.
-
Parikh LI, Reddy UM, Männistö T, Mendola P, SjaardaL, et al. (2014) Neonatal outcomes in early term birth. Am J Obstet Gynecol 211(3): 265e1-265e11.
-
Noli SA, Baini I, Parazzini F, Mauri PA, Vignali M, et al. (2019) Preterm Birth, Low Gestational Age, Low Birth Weight, Parity, and Other Determinants of Breech Presentation: Results from a Large Retrospective Population-Based Study. Biomed Res Int 16: 9581439.
-
Bailit JL, Gregory KD, Reddy UM, Quintero VHG, Hibbard JU, et al. (2010) Maternal and neonatal outcomes by labor onset type and gestational age. Am J Obstet Gynecol 202(3): 245e1-245e12.
-
Clark SL, Miller DD, Belfort MA, Dildy GA, Frye DK, et al. (2009) Neonatal and maternal outcomes associated with elective term delivery. Am J Obstet Gynecol 200(2): 156e1-156e4.
-
Wilcox AJ (1993) Birth weight and perinatal mortality: the effect of maternal smoking. Am J Epidemiol 137(10): 1098-1104.
-
Tiwari SK, Kumar N, Kumar S, Prabha R (2017) A study of late preterm babies for early neonatal outcome. Ind Jr Neo Med Res 5: 1-5.
-
Wilcox AJ (2001) A review: on the importance—and the unimportance—of birthweight. Int J Epidemiol 30(6): 1233-1241.
-
Seikku L, Gissler M, Andersson S, Rahkonen P, Stefanovic V, et al. (2016) Asphyxia, Neurologic Morbidity, and Perinatal Mortality in Early-Term and Postterm Birth. Pediatrics 137(6): e20153334.
-
Ghartey K, Coletta J, Lizarraga L, Murphy E, Ananth CV, et al. (2012) Neonatal respiratory morbidity in the early term delivery. Am J Obstet Gynecol 207(4): 292.e1-292. e4.
-
Bates E, Rouse DJ, Tita ATN, Carlo WA, Chapman V, et al. (2010) Neonatal outcomes after demonstrated fetal lung maturity before 39 weeks of gestation. Obstet Gynecol 116(5): 1295.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’