An Analytical Study on the Medical Reports of Rape Survivors in Nepal
Case reports of rape is increasing in society. Rape adversely affects physical, mental, and social wellbeing. Clinicians are at the forefront for the medical management as well providing medico-legal documentation as per the guidelines protocol imposed by the State. This is a retrospective rape case law study of cases retrieved from the Nepalese Supreme Court website. The medical reports provided were studied on the rape cases claimed and analyzed. 149 rape cases were analyzed for medical report. Only one third of the rape cases had positive findings of rape. However, only physical evidence of violence was noted, mainly on the state of hymen, signs of struggle and the presence or absence of spermatozoa in female genitalia. Age determinations were requested to mitigate the punishment in perpetrator. The significance of mental, behavioral, and social wellbeing in rape victims were completely overlooked in the medical report documentation.
Introduction
The word rape is derived from Latin term “rapio” which means “to snatch” [1]. Absence of consent is the essential element in the crime of rape [2]. The victim’s body is forcibly seized by the perpetrator to fulfill the gratification of sex. Rape is a heinous crime criminalized by the law in Nepal [3]. The number of reported cases of sexual violence has increased by 256 percent in the past decade [4]. The Nepal Police report of October 2020 shows that there are 7 reported cases of sexual violence every day. The report adds on that 61.3% of women with sexual violence never shared the incident to anyone, thus suffer in silence. The consequence of rape is known to have immediate, short-term, and long-term physical, mental, and psychosomatic maladies [5]. Clinicians are the forefront for the medical management [6] as well as medico-legal documentation on the victim which carry a huge impact in the court of justice not only to come into final verdict, but also for justice for victim of crime, rehabilitation, and security against further abuse. This is a retrospective case law study on rape cases, retrieved from the Supreme Court website from the fiscal years 2012/13 to 2017/18 under the jurisdiction of High Court in Province Five in Nepal. The medical reports provided were studied on rape cases claimed and analyzed. 149 rape cases were analyzed for medical report. This research analyses the medical reports on the rape victim and the accused.
Methodology
This study is a retrospective descriptive focused analysis on the medical report on rape cases retrieved from the Supreme Court website under the jurisdiction of High Court in Province Five in Nepal registered from fiscal year 2012/13 to fiscal year 2017/18. The data were collected and processed with Microsoft Excel format for evaluation.
At the time of research, 149 cases under the jurisdiction of High Court in Province Five in fiscal year 2012/13 to 2017/18 were able to be retrieved from the Supreme Court website for analysis (Table 1 & Figure 1).
Age group of the Rape Survivors
Results & Discussion
| Age of Survivors | <10 years | 11-13 years | 14-16 years | 17-18 years | >18 years | Total |
|---|---|---|---|---|---|---|
| Number of Survivors | 46 | 27 | 30 | 6 | 40 | 149 |
| Percentage | 31% | 18% | 20% | 4% | 27% | 100% |
Table 1: Age Group of Rape Survivors.
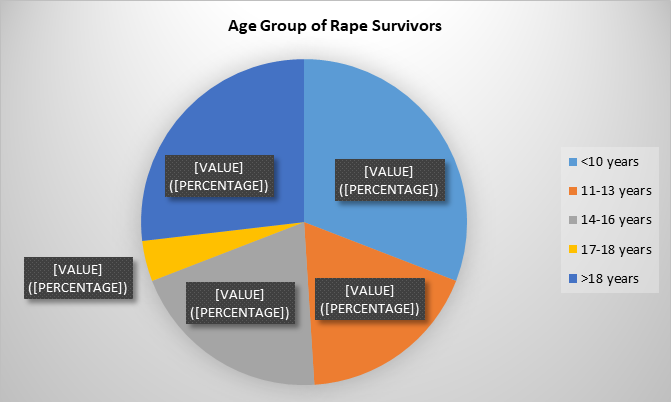
The most vulnerable group was minor (less than 18 years of age) composing almost three quarters of survivors in this study. The younger the girls, the more violence they were found to suffer. More than one third of the rape survivors in this research were less than 10 years of age. The high incidence of children less than 10 years of age could be due society having less tolerance to violence that takes place in small children. The seriousness of the outcome, such as vaginal bleeding, tear, discharge etc., causes anger and draws emotion of retribution compelling parents to demand justice. Children less than 10 years of age are unlikely to distinguish sexual activities to any other activity; moreover, when involving someone trusted and known [7, 8, 9]. The perpetrators take the advantage of vulnerabilities and innocence of children. Another large group of victims were children aged between 11 and 16 years of age, where almost 40% survived the sexual violence. These groups of children are easy to coerce and threat and get involved in sex without much struggle. Girls aged 16 and 18 were relatively spared, mainly because they could voice out their refusal, retaliate or the perpetrator may have feared exposure and consequences of court appearances.
The mental health consequences of sexual violence can be just as serious and long lasting. Victims of child sexual abuse, for example, are more likely to experience depression, substance abuse, post-traumatic stress disorder (PTSD) and suicide in later life than their non-abused counterparts. Worldwide child sexual abuse is a major cause of PTSD, accounting for an estimated 33% of cases in females and 21% of cases in males [10]. Most of the survivors were female, however, there were 4 cases of male children who suffered unnatural sexual violence which was brought to trial for justice. There are likely to be several dormant cases of male rape victims that are never unveiled. This could possibly be due to stereotypes set on men and boys to act brave and to not to voice out their sufferings (Table 2 & Figure 2).
Relation of Rape Survivor to the Perpetrator
| Relationship | Blood related | Relative | Neighbors | Entrusted | Strangers | Total |
|---|---|---|---|---|---|---|
| Number of Rape Survivors | 3 | 6 | 113 | 11 | 16 | 149 |
| Percent | 2% | 4% | 76% | 7% | 11% | 100% |
Table 2: Relation of Rape Survivor to the Perpetrator.
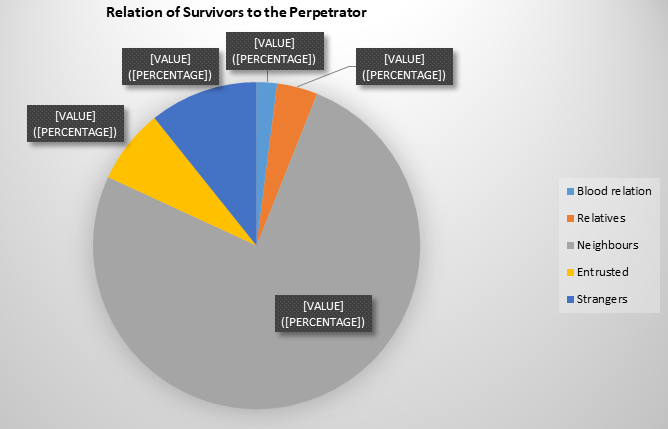
The risk factors in the study are the perpetrators who are known to the survivors and thus trusted [11, 12, 13]. 90% of rapes were victimized by someone they trusted as their well-wisher: close family members, relatives, and entrusted people by family. 76% of survivors were raped by neighbors. 74% children were raped, those who can be easily influenced with love or threat, similarly noted as in other studies [7, 8, 9]. 90% of perpetrators were someone the survivor know and trusted. Only 10% of rapes were done by strangers. These
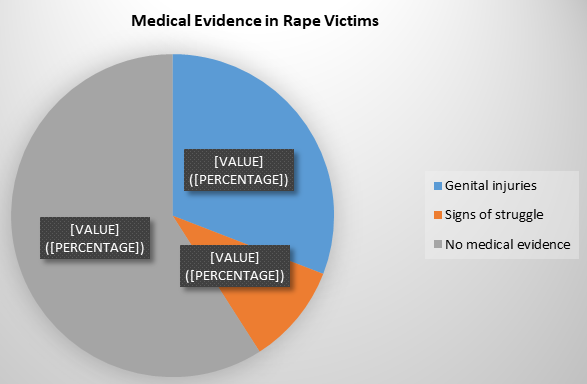
Medical Report of the Survivors of Rape Crime
could be the reasons that there was very little sign of struggle (10%) in rape survivors in this study. The perpetrators appear to be opportunistic to the vulnerability of trust and lonely situation at the time of crime. In addition, in Nepali culture, every single male neighbor or acquaintances are called as brother, uncle, father, grandfather according to age, and people trust easily. This could probably be the reason that only 10% of the rape survivors had signs of struggle in the study (Table 3 & Figure 3).
| Medical report findings | Signs of struggle in rape victim | Genital injuries following rape | Absence of medical evidence of injuries | Total |
|---|---|---|---|---|
| Number of rape survivors | 15 | 46 | 88 | 149 |
| Percent | 10% | 31% | 59% | 100% |
Table 3: Medical Report on Rape Survivors.
The State protocol obliges a clinician to fill up a clinical format for documentation in rape cases [3]. Sexual violence has both physical and psychological effects on health and well- being; these can be short- and/or long-term [6]. The health consequences of, and the responses to, sexual violence vary markedly between individuals and according to the nature of the abuse (e.g., frequency, severity, perpetrator) [14]. A good report demands timely examination of rape survivor, preferably immediately or at least within 72 hours of rape, so as not to erase the evidence. A dedicated, compassionate, and specially trained clinician for the management of rape victim is preferred. The detail history taking, physical examination along with mental status evaluation ensuring confidentiality is paramount [6]. Depending on the case scenario emergency treatment for injuries, gynecological trauma, emergency contraception, treatment and prophylaxis for sexually transmitted infection, prophylaxis for HIV as appropriate, information on safe abortion, and forensic examination along with maintaining the chain of command in transferring the sample for laboratory testing [6]. The survivors are vulnerable to sexual and reproductive health consequences such as unwanted pregnancy, unsafe abortion, pregnancy complication, infanticide, and a higher risk of sexually transmitted infections, including from HIV, traumatic fistula, subfertility, and sexual dysfunction. The survivors may suffer from mental health problems such as anxiety, depression, panic disorder, sleep disorder, suicidal tendencies. In addition, the survivors may have high risk behavioral problems [14].
Sexual intercourse or rape to minor girls bears the danger of injury to external as well as the internal reproductive organs. There is also the possibility of conception, pregnancy, abortion, or childbirth, and sometimes subfertility. In all the situations, there are utmost dangers to the girl child of her life due to biological and physiological immaturity.
Maternal mortality in teenage pregnancy is one of the most important preventable aspects in Obstetrics [15]. Evidence suggests that male and female survivors of sexual violence may experience similar mental health, behavioral and social consequences [16, 17, 18, 19]. In this study there is 30% positive evidence of genital injuries in rape survivors. Only 10% were noted to have physical evidence of struggle. None of the sample send from the rape case was positive for spermatozoa. The medical examination report of accused men were mostly negative; only one had a bite mark, and 2 had few abrasions noted on the body. The medical reports have no mentioning of the behavioral, social or the mental status of the victim.
Conclusion
Medical examination on a rape survivor by a trained, dedicated, compassionate clinician is paramount not only for the immediate case management, medico-legal documentation, but also for the long-term possible holistic care for the optimum health of the survivor. Victims of sexual assault require comprehensive, gender-sensitive health services to cope with the physical and mental health consequences of their experience and to aid their recovery from an extremely distressing and traumatic event The World Health Organization’s definition of health is the “physical, mental and social wellbeing, and not merely absence of disease or infirmity”. Rape survivors suffer significant physical, mental, behavioral, and social maladies, gesturing towards the need for multidisciplinary medical teamwork up and plan of management. In Nepal at the time of this medical case law study, the medico-legal documentation needed to be filled in by doctors was inadequate. There is a need for amendment of medico-legal care for victims of rape in alignment with international standards. The government needs to prioritize these aspects in the care of rape victim survivors: in the setting of physical infrastructure facility structure, equipment, trained service-providers who work with ethical issues, and internationally standardized medico- legal documentation. In addition, a system of long-term holistic medical care, regular monitoring, and follow-up to identify shortcomings of these services and upgrade must be established.
References
-
Yubaraj S (2010) Jurisprudence: the philosophy of law, oriental perspective, with special reference to Nepal. Kathmandu School of Law, pp: 579.
-
World Health Organization (2002) World report on violence and health.
-
The National Penal (Code) Act (2017) An Act Made To Amend And Consolidate Laws In Force Relating To Criminal Offences.
-
Demographic and Health Survey (2016) Nepal Demographic and Health Survey. Ministry of Health, USA, pp: 1-636.
-
Tjaden P, Thoennes N (2000) Full report of the prevalence, incidence, and consequences of violence against women: findings from the National Violence against Women Survey. National Institute of Justice, Washington, DC.
-
(2003) Guidelines for Medico Legal Care for Victims of Sexual Violence, World Health Organization, Geneva.
-
Bennett LR, Manderson L, Astbury J (2000) Mapping a global pandemic: review of current literature on rape, sexual assault and sexual harassment of women. Centre for Women’s Health in Society, World Health Organization.
-
Jenkins C (1998) Sexual behavior in Papua New Guinea. Report of the Third Annual Meeting of the International Network on Violence against Women, International Network on Violence against Women, Washington, DC.
-
Bourgois P (1996) In search of masculinity: violence, respect and sexuality among Puerto Rican crack dealers in East Harlem. British Journal of Criminology 36(3): 412-427.
-
Heise L, Ellsberg M, Gottemoeller M (1999) Ending violence against women. Baltimore, MD, Johns Hopkins University School of Public Health, Center for Communications Programs.
-
Unicef Nepal/ UNDP/ WHO Nepal Report (Relationship/ age).
-
Bourgois P (2014) In search of respect. 2nd (Edn.), Selling Crack in El Barrio, Cambridge University Press.
-
Ariffin RE (1997) Shame, secrecy and silence: study of rape in Penang. Penang, Women’s Crisis Centre.
-
Petty GM, Dawson B (1989) Sexual aggression in normal men: incidence, beliefs and personality characteristics. Personality and Individual Differences 10(3): 355-362.
-
World Health Organization & Pan American Health Organization (2012) Understanding and Addressing violence against women: intimate partner violence. WHO, Geneva, pp: 12.
-
Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe JS, et al. (2014) 24th Edition William Obstetrics.
-
Andrews G, Corry J, Slade T, Issakidis C, Swanstion (2004) Child sexual abuse. In: Ezzati M, et al, (Eds.), Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. World Health Organization, Geneva.
-
Dube SR, Anda RF, Whitfield CL, Brown DW, Felitti VJ, et al. (2005) Long-term consequences of childhood sexual abuse by gender of victim. Am J Prev Med 28(5): 430- 438.
-
Patel V, Andrew G (2001) Gender, sexual abuse and risk behaviours in adolescents: a cross-sectional survey in schools in Goa. Natl Med J India 14(5): 263-267.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’