Screening and Management of Smoking in Pregnancy
Smoking in is harmful to both the mother and baby in pregnancy. Smoking cessation is strongly encouraged and needs to be approached in a sensitive manner employing patient centred care. Women should be provided with information about the risks of smoking and referred to smoking cessation services. Referral applies to smokers and ex-smokers who quit in the prior two weeks. Data was collected from smoker or ex-smoker post-natal mothers who delivered at Mater Dei Hospital and was analysed against NICE Public Health guideline (PH26) ‘Smoking: stopping in pregnancy and after childbirth’ published in 2010 and Green-top guideline no.31 ‘The Investigation and Management of the Small-for-Gestational-Age Fetus’ published in 2013. The audit included 50 post-natal smokers or ex-smokers with the majority being either smokers or ex-smokers who stopped as soon as they found out they were pregnant. There was not a single documented referral to smoking cessation services. Only 75% of smokers who smoke 11+ cigarettes daily had serial ultrasounds to monitor for SGA. Foetal outcomes were overall satisfactory with only 12% being admitted to NPICU, 10% of which belonged to mothers still smoking in pregnancy. It is essential that mothers understand the risks of smoking in pregnancy and these should be provided with the necessary information and assistance in smoking cessation. It is not enough to recommend smoking cessation but referrals and constant support should be offered.
Introduction
Smoking is one of the leading preventable causes of adverse outcomes in pregnancy and may impact the unborn child and infant with long-term health and socio- economic effects [1]. It increases the risk of miscarriage, foetal abnormalities, contributes to intra-uterine growth retardation, prematurity, and may lead to perinatal death.
Infants are also at greater risk of sudden infant death syndrome and have a detrimental impact on the educational achievements in childhood. Smoking cessation in pregnant women is strongly encouraged and needs to be approached in a sensitive manner employing patient centred care [2]. Women should be provided with information about the risks of smoking to themselves and the unborn child and referred to smoking cessation services. The scope of this audit is to compare local practice to NICE Public Health guideline (PH26) ‘Smoking: stopping in pregnancy and after childbirth’ published in 2021 [3] and Green-top guideline no.31 ‘The Investigation and Management of the Small-for-Gestational-
Age Fetus’ published in 2013 to assess whether optimal care is provided to antenatal mothers who smoke [4].
Materials and Methods
The data was collected from post-natal mothers who were smokers or ex-smokers. Data was collected at the Obstetrics Ward 1 and 3 at Mater Dei Hospital between 1st February and 31st March 2021 during the recovery period of post-natal mothers. The information gathered consisted of patient age, BMI, gestational age at delivery, smoking status, no. of cigarettes smoked daily, when they stopped if ex-smokers, documentation of serial ultrasounds from 26-28 weeks, fetal outcomes immediately after delivery and birth weight.
Results
This audit included 50 post-natal mothers who were smokers or ex-smokers. 48% (24) were smoking in pregnancy whilst 52% (26) were ex-smokers. Out of the ex- smokers a majority of 77% (20) had only stopped as soon as they found out they were pregnant, meaning <2 weeks prior pregnancy. The average maternal age was 30 years with ages ranging between 15 to 42 years old? NICE Public Health guideline (PH26) recommends referrals for all smokers and ex-smokers for smoking cessation services but there were no such referrals documented on any of the patients’ maternity notes. A small group of smokers, 33% (8), admitted to smoking 11+ cigarettes daily. Out of these, 75% (6), had serial ultrasounds from 26-28 weeks as recommended by Green-top guideline no.31, whilst the other 25% (2), were not followed up by serial ultrasounds. Out of all the patients, 76% (38) lived with another household member who smoked but the effect due to exposure from second hand smoking is difficult to quantify. 48% (24) patients had a raised body mass index and classified as overweight or obese, whilst 6% (3) were noted to be underweight. The obstetric history was also noted, with 24% (12) of patients having a history of a previous miscarriage but no IVF pregnancies.
44% (22) delivered vaginal whilst 56% (28) delivered by C-section. Information on whether the delivery was spontaneous induced or an emergency C-section was not documented as it was beyond the scope of this audit. 14% (7) of births were preterm at the time of delivery, 10% (5) of which belonged to mothers still smoking in pregnancy. Foetal outcomes were generally satisfactory with only 12% (6) being admitted to NPICU, 10% (5) of which belonged to mothers who were still smoking in pregnancy. Birth weights ranged between 1.69- 4.23Kg. A majority of 94% (47) weighed between 2-3.9Kg whilst only one fetus had a low birth weight of 1.69Kg and 2 fetuses weighed more than 4Kg. 62% (31) of patients wanted to try breastfeeding after delivery. It was difficult to objectively determine whether this attempt was successful and if smoking affected the quality and quantity of breast milk, hence this data was not collected. The majority of patients who had stopped smoking during pregnancy had resumed smoking after delivery. In fact, 62% stated that they resumed smoking by 8 weeks post-partum.
Discussion
Smoking leads to disease and disability and has the potential to harm every organ of the body causing cancer, heart disease, stroke, lung diseases, diabetes, and chronic obstructive pulmonary disease amongst many others. Therefore, it comes as no surprise that smoking is harmful in pregnancy [5]. Smoking cessation in pregnancy involves communicating in a sensitive, patient-centred manner, especially because some pregnant women find it difficult to say that they smoke. Such an approach is important to reduce the likelihood that some of them may miss out on the opportunity to get help [2]. Recommendations to stop smoking will benefit women who are planning a pregnancy, those already pregnant as well as the unborn child, any children she may have especially infants under the age of 12 months, her partner and other household members [3]. Smoking in pregnancy may be considered a taboo topic since the pressure not to smoke during pregnancy is intense that mothers who smoke often find it difficult to admit. This, in turn, makes it difficult to ensure they are offered appropriate support [2].
The earlier the intervention to encourage smoking cessation the better. Mothers should be screened for smoking at the first maternity booking visit and at each subsequent appointment. The first step is to use any appointment as an opportunity to ask women if they smoke and advise them to stop, not just cut-down. Intervention is not solely the responsibility of the obstetrician or the midwife but includes all healthcare workers involved in patient care such as GPs, nurses, paediatricians and other members of the maternity team [2]. Patients should be provided with information about the risks to the unborn child of smoking when pregnant and the hazards of exposure to second-hand smoke for both mother and baby [3].
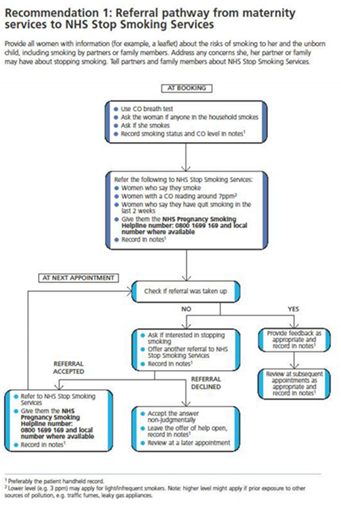
In the United Kingdom all mothers are screened for smoking and those who are smokers or ex-smokers within the past 2 weeks are checked for Carbon Monoxide level at the booking visit. The CO breath test is a physical measure of smoking as well as exposure to smoke. They then refer smokers, ex-smokers (< 2 weeks) and mothers with a Carbon Monoxide reading of 7ppm for smoking cessation services. This test is not carried out in Malta, and it is up to the patients whether they wish to disclose their smoking status. The pathway used by the national health system in the United
Kingdom is simplified in Figure 1 [2].
Those who wish to stop should be offered a referral for smoking cessation services which should be clearly documented in the antenatal records. Referral should apply to smokers and ex-smokers who have stopped within the last two weeks. Out of the 52% ex-smokers, 77% had only stopped as soon as they found out they were pregnant, meaning <2 weeks prior pregnancy. Local helplines should be provided in case they want to talk to someone over the phone until their next appointment and offer them regular follow up [2]. some may decide to opt out of referral to cessation services. In this case it is important to accept the decline in an impartial and respectful manner, leave the offer of help open and consider providing structured self-help materials or support via the telephone helpline or even offering home visits. Those who opt out should be sent information on smoking and pregnancy, including details on how to get help to quit at a later date [2]. It is also important to ask if her partner or anyone else in her household smokes, since this is common for many smokers. In fact 76% of the patients lived with another household member who smoked. When there are household smokers it’s essential to provide clear advice about the danger that second-hand smoke poses to the pregnant woman and to the baby, before and after birth and recommend not smoking around the pregnant mother or baby especially in the house or car. This could be used as an opportunity to quit smoking and provide them with a helpline or referral to contact cessation services [2].
Studies have shown that interventions effective in helping women who are pregnant to quit smoking include cognitive behaviour therapy, motivational interviewing, structured self-help and support from cessation. The method used to quit smoking, including whether or not the mother received help and support should be clearly documented on the patients notes and a follow up provided one year after the quitting date [2]. The management in antenatal clinics in Mater Dei Hospital relies on the history taken during the first antenatal booking visit. If patients are smokers or ex-smokers this should be clearly documented on their antenatal records and the patient should be provided with self-help tools, such as the website and contact numbers for smoking cessation services or else directly referred by the caring physician who can contact cessation services in the patient’s name [6]. Another tool that can be used for smoking cessation is pharmacological support including Nicotine replacement therapy (NRT). There is mixed evidence on the effectiveness of NRT and other pharmacological support in helping women to stop smoking during pregnancy. Trials have found no evidence that it is effective (or that it affects the child’s birthweight). In addition, there are insufficient data to form a judgement about whether or not NRT has any impact on the likelihood that a child will need special care or will be stillborn. NRT is prescribed for use only once the smoker has quit and for duration of two weeks to start with. Pregnant women who are using nicotine patches are advised to remove them before going to bed and it is important to note that neither Varenicline nor Bupropion should be offered to pregnant or breastfeeding women [2]. It is essential that staff involved in patient care throughout pregnancy are trained to encourage mothers to be open about their smoking, know about the health risks of smoking and the benefits of quitting and understand why it can be difficult to stop, know about the treatments that can help people to quit and how to refer them to local services for treatment and always recommend quitting rather than cutting down [2].
Unfortunately, in our audit, none of the mothers were referred for smoking cessation services. The lack of referrals can be attributed to many factors such as failed previous attempts, limited time during the antenatal visit, lack knowledge about the services offered or fear that it might harm the doctor-patient relationship. It is well known that smoking may lead to delivery of a small for gestational age (SGA) infant. The risk for SGA is most relevant in mothers who smoke 11+ cigarettes daily. In fact Green-top guidelines shown in Figure 2. Recommend that these mothers are monitored by serial ultrasounds from 26-28 weeks approximately every two weeks. The results from the audit show that 33% of known smokers admitted to smoking 11+ cigarettes daily and out of these 75% had serial ultrasounds from 26-28 weeks whilst the other 25% were not followed up by serial ultrasounds as recommended [4].
![Figure 2: Recommend that these mothers are monitored by serial ultrasounds from 26-28 weeks approximately every two weeks. The results from the audit show that 33% of known smokers admitted to smoking 11+ cigarettes daily and out of these 75% had serial ultrasounds from 26-28 weeks whilst the other 25% were not followed up by serial ultrasounds as recommended [4].](/fulltextimages/9712/fig_2.png)
Foetal outcomes were generally satisfactory with only 12% being admitted to NPICU, 10% of which belonged to mothers who were still smoking in pregnancy. 14% of births were born preterm meaning they were delivered earlier than 37 weeks, 10% of which belonged to mothers still smoking in pregnancy.
It was noted that even though several mothers who previously smoked had decided to stop smoking during pregnancy, 62% of these resumed smoking within the first 8 weeks after delivery. This stresses the need for ongoing support and functioning systems in place for mothers who are attempting to quit smoking. Smoking does not only harm the mother and the unborn child, but babies and children of mothers who smoke are also at greater risk of sudden infant death syndrome, asthma, pneumonia and behavioural problems such as ADHD (attention deficit hyperactivity disorder). Stopping smoking reduces the risk of such complications [2]. Discrepancy between standard guidelines and current practice will serve as an eye opener as well as a reminder to adhere to recommended guidelines and hence improve quality of care.
Conclusion
It is essential that mothers understand the risks of smoking in pregnancy. As clinicians it is our responsibility to provide patients with the necessary information and provide assistance in smoking cessation. It is not enough to simply recommend smoking cessation, but referrals constant support should be offered to all patients who fit the criteria.3
References
-
Gorman DM (2019) Use of publication procedures to improve research integrity by addiction journals. Addiction 114(8): 1478-1486.
-
(2008) Smoking and pregnancy patient information leaflet. Royal College of Obstetricians & Gynaecologists.
-
NICE (2022) Tobacco: preventing uptake, promoting quitting and treating dependence. National Institute for Health and Care Excellence, pp: 1-107.
-
(2013) Small-for-Gestational-Age Fetus, Investigation and Management (Green-top Guideline No. 31). Royal College of Obstetricians & Gynecologists.
-
Annika CG, Pete D, Seth MN, David H, Geoffrey TF (2019) Impact of adding and removing warning label messages from cigarette packages on adult smokers’ awareness about the health harms of smoking: findings from the ITC Canada Survey. Tobacco Control 28(1): e56.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’