The Management of Obese Women in Pregnancy & Neonatal Outcome in Malta
Background: Over the past few years, the rise of obesity in pregnancy has been associated with a rise in pregnancy complications. The aim of this audit was to analyze the current management of obese women in pregnancy at Mater Dei Hospital (MDH). The Royal College of Obstetricians and Gynaecologists (RCOG) green-top guideline: Care of Women with Obesity in Pregnancy which was published in 2018 was used as a standard for this audit. Method: Data was collected from inpatient medical notes of obese mothers who presented at MDH between July 2020 and October 2020. There was no patient contact during data collection and all data was kept anonymous. Results: 53 mothers were recorded as obese between July and October 2020. The average maternal age was 31 years and the average maternal weight was 94kgs at antenatal booking visit. 47% of obese mothers were classified as Class 1 obese. Only 38% of obese mothers had an oral glucose test performed, and 70% of these mothers had a positive test.54.7% delivered via a caesarean section. 12% of neonates required NPICU admission. Conclusion: Pregnancy in women with obesity is an important public health problem with short- and long-term implications for maternal and child health. This audit demonstrates that the management of obese women in pregnancy currently in use at MDH does not follow all the RCOG recommendations. We suggest the need for local guidelines together with the use of patient information leaflets to help improve the care of women with obesity in pregnancy.
Introduction
It is well known that obesity in Malta is a public health concern. In fact, 25.5% of the Maltese population is classified as obese when compared to 14.9% in the rest of Europe [1]. According to the latest data found by NOIS in 2015, 23.8% of mothers were classified as overweight while 13.7% of mothers were classified as obese [2]. The World Health Organization (WHO) defines obesity as a Body Mass Index (BMI) of 30Kg/m2 or more [3]. It is subdivided into 3 classes; Class 1 with a BMI range of 30 to 34.9Kg/m2, Class II with a BMI between 35 and 39.9Kg/m2 and Class III with a BMI exceeding 39.9Kg/m2 [4] Over the past few years, the rise of obesity in pregnancy has been associated with a rise in pregnancy complications such as gestational diabetes, pre-eclampsia, venous thromboembolism (VTE), wound infections and stillbirths. Obese pregnant women are 40% more likely to experience stillbirth when compared to non-obese pregnant women [5]. Also, fetuses of obese mothers have a higher risk of congenital anomalies, intra-uterine growth restriction and macrosomia [6]. Furthermore, babies born to obese mothers are 1.5 times more likely to be admitted to NPICU than babies born to mothers of a healthy weight [7]. As a result, there is a need for consistent clinical care including pre-pregnancy care, antenatal and postpartum care. Many studies have shown that guidelines can improve the health care system and reduce adverse effects [6]. Currently, there are no guidelines on the management of obese women in pregnancy in use at Mater Dei Hospital (MDH). The RCOG Green top Guideline 2018: ‘Care of Women with Obesity in Pregnancy’ was used as a standard for this audit.
Materials and Method
Data was collected from in patient medical notes found in Obstetrics wards 1, 2, 3 and delivery suite at MDH, Malta. The inclusion criteria included all mothers with a BMI of 30Kg/m2 or more that presented to MDH for delivery from July 2020 to October 2020. Most of the information required was gathered from blue cards and partograms. The BMI was calculated by using the following formula; weight (Kg)/ [height (m)]2. The maternal weight used was the one taken at the first booking visit at around 11 week’s gestation. Blue cards which failed to document this weight were automatically excluded from the audit. In order to audit post-partum complications and neonatal outcome, the medical notes of a mother within the inclusion criteria were followed up 48hrs post-partum or until the mother was fit for discharge. Data collection consisted of the following; Demographic data, BMI, gestational age at delivery, treatment during pregnancy, mode of delivery, post- partum complications and neonatal outcome were recorded.
Data was stored and analyzed using google sheets. The data was protected with a password which only the authors had access to. All data was kept anonymous and was destroyed at the end of the audit. Data from private hospitals was not included in this audit. Data was analyzed in percentages and presented in tables and bar charts as deemed appropriate.
Results
Between July 2020 and October 2020, a total of 53 mothers were recorded as obese at MDH. This excludes potential obese mothers who did not have documentation of weight. Maternal age ranged from 20 to 42 years with an average age of 31 years. The average weight taken at the antenatal booking visit was 94Kg (range 75Kg – 134.5Kg). Table 1 shows the BMI distribution of obese mothers that presented to MDH during the 3 months of data collection. 77% of obese mothers were re-weighed during the 3rd trimester.
| BMI (Kg/m2) | Nutritional Status | Percentage of Mothers |
|---|---|---|
| 30.0–34.9 | Class I | 47% |
| 35.0–39.9 | Class II | 34% |
| Above 40 | Class III | 19% |
Table 1: Patient BMI distribution.
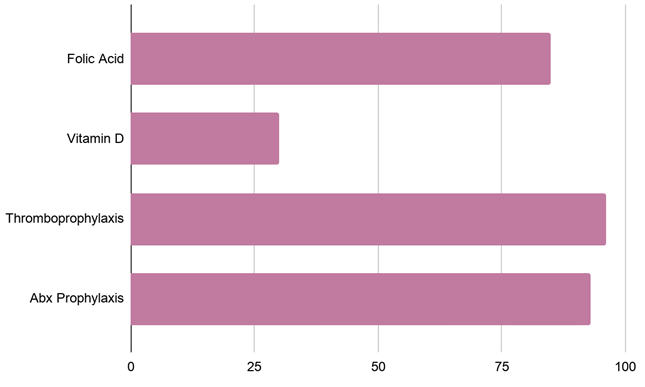
From a total of 53 mothers, a history of 21 miscarriages and 6 stillbirths were noted. 51% were nulliparous, 26% primiparous and 23% multiparous. Figure 1 shows the treatment given to these mothers. 85% of mothers had documentation of folic acid supplementation during the first trimester of pregnancy. 30% had documentation of vitamin D supplementation. 96% of mothers were given Enoxaparin 40mg daily after LSCS as thromboprophylaxis.
Only 38% of obese mothers had an oral glucose tolerance test (OGTT) and 7 out of these 10 mothers had a positive test. 21% of obese women were referred for dietician advice. As recommended by the RCOG, no mother was taking weight loss medications during pregnancy. 11 mothers were primigravida and had a BMI of 35Kg/m2 or more, but only 3 of these mothers were taking Aspirin. 75% of mothers in Class II and Class III had serial assessment of foetal size using ultrasound. Only 11% of mothers in Class III had an obstetric anaesthetic referral and no mother was referred for tissue viability. 67% of mothers had venous access established early but there was no documentation of a second cannula being established during labour. An equal amount of induction of labours (IOL) and lower segment caesarean section (LSCS) were performed. Table 2 shows the distribution of planned mode of delivery versus actual mode of delivery that occurred in obese mothers during July 2020 and October 2020. During these 3 months of data collection, 89% of mothers did not experience postpartum complications. The other 11% reported 3 wound infections, 2 persistently high blood pressures and 1 increased per- vaginal bleeding.
| Planned Mode of Delivery | Actual Mode of Delivery |
|---|---|
| 22 Induction of Labour | 1 Instrumental Delivery |
| 17 Normal Vaginal Delivery | |
| 4 Emergency LSCS | |
| 22 Elective LSCS | 16 Elective LSCS |
| 6 Emergency LSCS | |
| 9 Not Discussed/ Documented | 6 Normal Vaginal Delivery |
| 3 Emergency LSCS |
Table 2: Planned mode of delivery versus actual mode of delivery From a total of 53 mothers, 49 singleton pregnancies, 3 twin pre
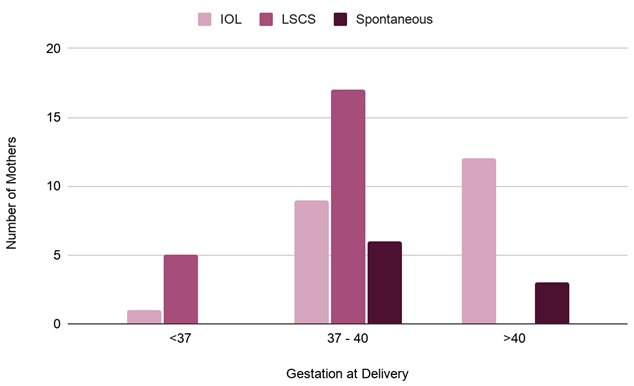
Table 2: Planned mode of delivery versus actual mode of delivery From a total of 53 mothers, 49 singleton pregnancies, 3 twin pregnancies and 1 triplet pregnancy were documented. Figure 2 shows that 61% of neonates were born between 37 and 40 weeks gestation, the majority of these were delivered by elective LSCS. 28% of neonates were delivered after 40 weeks mainly by induction of labour and 11% of babies were born before 37 weeks with the preferred mode of delivery being elective LSCS.
The average birth weight was 3.2Kg. The highest birth weight was 4.8Kg in a neonate born at 40 + 2 weeks to a mother weighing 134.5Kg who did not have an OGTT during the pregnancy. 96% of babies had a reassuring APGAR score, i.e. a score between 10 and 7 in the first 5 minutes after birth. 12% of neonates required NPICU admission for the following reasons: a twin baby weighing 1.8Kg, premature triplets born at 32+2 weeks, microcephalic osteodysplastic primordial dwarfism born at 34+4 weeks, a preterm baby born at 29+6 weeks and a baby with low APGAR score of 4, 5, 7 born at 38 weeks weighing 3Kg. Other abnormalities reported were tuft of hair and dimples on lower back, hypospadias and overriding toes. No neonatal deaths were reported.
Discussion
Pregnancy in women with obesity is an important public health problem with short- and long-term implications for maternal and child health [8]. Obesity complicates almost all aspects of pregnancy and given the growing prevalence, obstetricians need to understand the risks associated with obesity in pregnancy and the unique aspects of management for women with obesity. Approximately 50% of women who become pregnant are either overweight or obese [9]. In 2015, NOIS published that 23.8% of mothers were overweight and 13.7% of mothers were obese [2]. Maternal obesity is known to be an important risk factor for gestational diabetes with large cohort studies reporting a 3-fold increased risk when compared to women with normal BMI [10, 11]. In our audit only 38% of obese mothers had an OGTT performed and 14 out of these 20 mothers had a positive OGTT.NICE guideline Hypertension in pregnancy: diagnosis and management published in 2019 states that the moderate risk factors for preeclampsia are BMI equal to or more than 35Kg/m2 at first visit, first pregnancy, age 40 years or older, pregnancy interval of more than 10 years, family history of pre-eclampsia and multi-foetal pregnancy [12]. The guideline recommends that pregnant women with more than 1 moderate risk factor needs to take 75-150mg of aspirin from 12 weeks until the birth of the baby. More recent evidence suggests that women with high risk of pre-eclampsia may benefit from taking 150mg of aspirin daily and this benefit is enhanced if taken at night, rather than during the day [13, 14] In our audit 11 mothers were primigravida and had a BMI of 35Kg/m2 or more, but only 3 of these mothers were given 75mg Aspirin.
Obesity is also a risk factor for VTE in pregnancy and the risk is higher with increasing obesity. Obesity is associated with a higher risk of pulmonary emboli (PE) (adjusted OR 14.9, 95% CI 3.0–74.8) than of deep vein thrombosis (adjusted OR 4.4, 95% CI 1.6–11.9) [15, 16]. As pulmonary embolism remains a leading cause of maternal deaths in developed countries and knowing that 60% of women who died from PE in the UK between 2003 and 2008 were obese, accurate risk assessment and use of thromboprophylaxis is of utmost importance. 96% of mothers in our audit were given Enoxaparin post LSCS, but all patients received a 40mg dose during their hospital admission. The detection of congenital anomalies by ultrasonography is reduced by 20% in obese women when compared to women of healthy weight [5]. The increased echogenicity of adipose tissue and increased absorption of the ultrasonic sound beam by the abdominal fat results in reduced image clarity and poor image quality [17, 18] Women should be counselled that all forms of screening for structural anomalies are more limited in obese pregnant women [7]. In our audit, we had no neonatal deaths and the anomalies noted at birth were overriding toes, hypospadias and a case of spina bifida occulta.
Pregnant women with a higher BMI have an increased risk of caesarean birth. A systematic review and meta- analysis by Poobalan, et al. concluded that the risk of LSCS is increased by 50% in overweight women and more than doubled in obese women [19]. However, the decision regarding mode of birth should be individualized and a multidisciplinary approach is recommended. A discussion between the consultant obstetrician, anaesthetist, midwife and woman during the antenatal period is encouraged. Lee et al concluded in 2016 that elective IOL at term in obese mothers may reduce the chance of LSCS without increasing the risk of adverse outcomes [20]. In our audit, 54.7% (29 mothers) delivered via a caesarean section with 55.2% of these mothers having an elective section.
Conclusion
The long-term effects of obesity are not limited to maternal health, but also programs pathophysiology in their offspring. Empathic and patient-centered care, along with knowledge, can optimize outcomes for women and children. This audit demonstrates that the management of obese women in pregnancy currently in use at MDH does not follow the RCOG Guidelines. In view of the well-recognized risks, maternity care providers should have specific local guidelines, an example of such guidelines adapted from the RCOG guideline can be found in Annex 1. We also recommend the use of educational leaflets on the risks of obesity in pregnancy (Annex 2). These leaflets should be given to women of reproductive age as part of their pre-pregnancy care.
References
-
NSO (2020) Anti-obesity day. National Statistics Office Malta.
-
Galea N, Gatt M (2018) Highlights of the European perinatal health report on core indicators in 2015-Malta perspective. Malta: Directorate for Health Information and Research.
-
WHO (2021) Obesity and overweight. World Health Organisation.
-
WHO (2010) Body Mass Index-BMI. World Health Organisation.
-
Palaszewski DM, Phelan ST (2017) Obesity and Pregnancy Treatment & Management. Medscape.
-
Simon A, Pratt M, Hutton B, Skidmore B, Fakhraei R, et al. (2020) Guidelines for the management of pregnant women with obesity: A systematic review. Obes Rev 21(3): e12972.
-
Denison FC, Aedla NR, Keag O, Hor K, Reynolds RM, et al. (2019) Care of Women with Obesity in Pregnancy (Green-top Guideline No.72). BJOG 126(3): e62-e106.
-
Dolin CD, Kominiarek MA (2018) Pregnancy in Women with Obesity. Obstet Gynecol Clin North Am 45(2): 217- 232.
-
NICE (2010) Weight management before, during and after pregnancy. National Institute for Health and Care Excellence.
-
Sebire NJ, Jolly M, Harris JP, Wadsworth J, Joffe M, et al. (2001) Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. Int J Obes Relat Metab Disord 25(8): 1175-1182.
-
Weiss JL, Malone FD, Emig D, Ball RH, Nyberg DA, et al. (2004) Obesity, obstetric complications and cesarean delivery rate–a population-based screening study. Am J Obstet Gynecol 190(4): 1091-1097.
-
NICE (2019) Hypertension in pregnancy: diagnosis and management. National Institute for Health and Care Excellence, pp: 1-57.
-
Roberge S, Nicolaides K, Demers S, Hyett J, Chaillet N, et al. (2017) The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: systematic review and meta-analysis. Am J Obstet Gynecol 216(2): 110-120.
-
Ayala DE, Ucieda R, Hermida RC (2013) Chronotherapy with low-dose aspirin for prevention of complications in pregnancy. Chronobiol Int 30(1-2): 260-279.
-
Kane EV, Calderwood C, Dobbie R, Morris C, Roman E, et al. (2013) A population-based study of venous thrombosis in pregnancy in Scotland 1980-2005. Eur J Obstet Gynecol Reprod Biol 169(2): 223-239.
-
Knight M, UKOSS (2008) Antenatal pulmonary embolism: risk factors, management and outcomes. BJOG 115(4): 453-461.
-
Phatak M, Ramsay J (2010) Impact of maternal obesity on procedure of mid-trimester anomaly scan. J Obstet Gynaecol 30(5): 447-450.
-
Chung JH, Pelayo R, Hatfield TJ, Speir VJ, Wu J, et al. (2012) Limitations of the fetal anatomic survey via ultrasound in the obese obstetrical population. J Matern Fetal Neonatal Med 25(10): 1945-1949.
-
Poobalan AS, Aucott LS, Gurung T, Smith WCS, Bhattacharya S (2009) Obesity as an independent risk factor for elective and emergency caesarean delivery in nulliparous women–systematic review and meta- analysis of cohort studies. Obes Rev 10(1): 28-35.
-
Lee VR, Darney BG, Snowden JM, Main EK, Gilbert W, et al. (2016) Term elective induction of labour and perinatal outcomes in obese women: retrospective cohort study. BJOG 123(2): 271-278.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’