Endometrial Stromal Nodule with Intense Decidual Changes. Findings during Delivery of the Placenta
Background: Endometrial stromal nodules involving the placental membranes are exceptionally rare. Only two cases have been described in the literature. We report a new case of endometrial stromal nodule with intense decidual changes as an incidental finding during delivery of the placenta. Case: A 31-years-old female patient with no history of interest presented after a normal term delivery, a 3.5 x 2.6 x 1cm well circumscribed nodule independent of the placenta and not attached to it. The tumor was asymptomatic and was not identificated ultrasonographically. Microscopically, the neoplastic nodule was composed of spindle and epithelioid cells with extensive eosinophilic cytoplasm with a decidualized appearance without associated glands, except for minimal epithelial remnants in the periphery. Characteristic features of endometrial stromal tumor were identified, such as CD10, WT-1, and progesterone receptor positivity, and an expanding noninfiltrating linear pushing rim. There were also pregnancy-related changes, such as decidualization and myxoid change. The lesion was considered a endometrial stromal nodule with an unusual morphology and increased proliferation rate due to the hormonal stimuli of pregnancy. Conclusion: We report a rare case of an incidental endometrial stromal nodule during delivery of the placenta, representing only the third such case reported in the world literature. In all likelihood, this neoplasm originated from the decidua of the free membranes.
Introduction
Endometrial stromal tumors (ESTs) are uncommon uterine tumours responsible for less than 10% of uterine mesenchymal neoplasms and less than 2% of all uterine neoplasms [1]. The last classification of the World Health Organization (WHO) in 2020 sub-categorized ESTs into four groups: Endometrial Stromal Nodule (ESN), Low- Grade Endometrial Stromal Sarcoma (LG-ESS), High-Grade Endometrial Stromal Sarcoma (HG-ESS), and Undifferentiated Uterine Sarcoma (UUS) [2]. The endometrial stromal nodule (ESN) is a benign tumor characterizes by a well-delineated, expansive margin and composed of cells resembling endometrial stroma in the proliferative phase with minimal or absent myometrial invasion (<3 mm and <3 bulges) and no vascular invasion [3]. Very few cases of endometrial stromal nodules involving the placenta have been described. Given the rarity of these tumors and the scarcity of reports in the literature regarding the clinical management and final evolution of these cases. We report a new case of endometrial stromal nodule with intense decidual changes found during delivery of the placenta.
Case Report
A 31-year-old woman, primigravida, had an unremarkable previous clinical history. The ultrasounds controls without incidences. The pregnancy was uneventful, and at the 39th week, a healthy male baby weighing 3270 g was delivered spontaneously. During the expulsion of the placenta, a 3 cm well-defined whitish ovoid nodule was identified, apparently independent of the placental membranes. Clinically it was thought to correspond either to a expelling of the placental tissue. The placental expulsion that followed was unremarkable with no unusual bleeding. We received for histological study a nodular tumor that macroscopically measured 3.5 x 2.6 x 1 cm, was oval, somewhat flattened, well demarcated, unencapsulated, grayish-brown in color. The cut surface presented a fleshy, whitish appearance with an elastic consistency. It was completely included for histological study. Microscopically, the nodule was composed of spindle and epithelioid cells with extensive eosinophilic cytoplasm with a decidualized appearance without associated glands, except for minimal epithelial remnants in the periphery. The cells showed varied architecture with more compact epithelioid areas alternating with spindle-shaped, storiform areas and very loose edematous-myxoid foci (Figure 1).
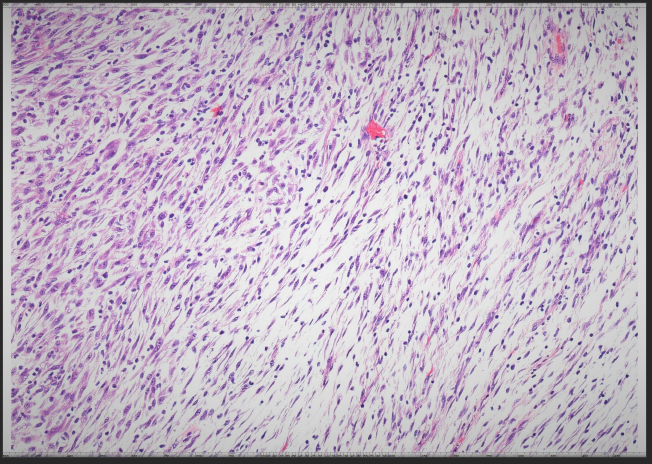
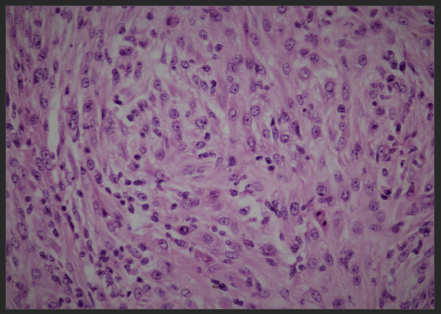
Foci of ischemic necrosis were identified. The nuclei were rounded or ovoid, of medium-large size with a small nucleolus and nuclear grooves, sometimes showing a vesicular appearance with a nucleolus. The proliferative activity was 5/7 mitoses per 10 HPF (Figure 2) in the most active areas (interpreted in the gestational context). There was a slight accompanying mixed inflammatory component and a rich vascular network (CD-34) of very small caliber and homogeneously distributed. In the periphery, remains of myometrium and decidua were identified with isolated intermediate trophoblast cells.
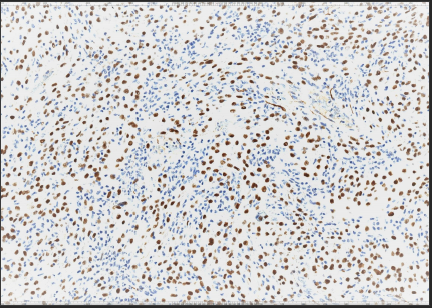
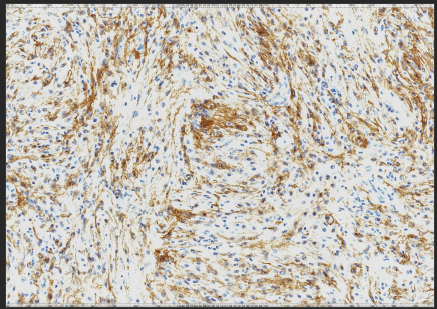
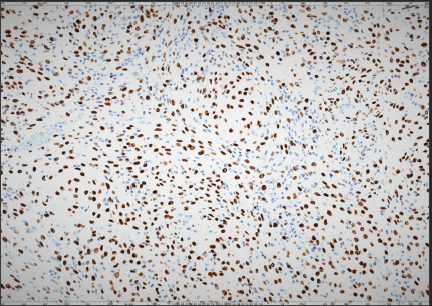
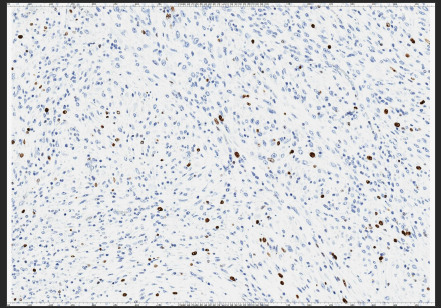
Immunohistochemistry revealed strong positivity for WT-1 (Figure 3), CD-10 (Figure 4), and progesterone (Figure 5). B-catenin was diffuse but weakly positive. The minimal epithelial remnants in the periphery were positive with CK8/18 and EMA. The proliferative activity (Ki-67) was moderate with around 20% (Figure 6), although it must be interpreted in the context of a pregnancy with a strong hormonal environment. Focal staining with estrogen and GATA-3. Cells were negative with muscle markers such as desmin, actin, calponin and caldesmon. Negativity with trophoblastic markers: PLAP, human placental lactogen, p63, p40 and human chorionic gonadotropin. ALK, inhibin, HMB-45 and Melan-A were also negative. This is a very unusual lesion with a decidualized appearance due to gestational changes. The lesion was in close contact with the decidua (remnants are observed in the periphery) with minimal surface myometrium. It is a decidualized cell lesion with endometrial stromal phenotype (WT-1, CD-10, and progesterone positive) without accompanying glands. A wide differential diagnosis was made, ruling out, among other lesions, muscle tumors (negative for desmin, actin, calponin and caldesmon), trophoblastic tumor, especially that of the placental bed (negative with PLAP, human placental lactogen, p63, p40 and chorionic gonadotropin), PECOMA (negative with HMB-45 and Melan-A) and inflammatory my fibroblastic tumor (negative with ALK, actin and desmin). For all these reasons, it was interpreted as ESN with intense gestational decidual changes. Clinical and ultra-sonographic follow-up of the patient, latest at 12 months after delivery, revealed no abnormalities in the uterine cavity.
Discussion
Neoplasms within the placental membranes are exceptionally rare. A few cases of leiomyomas have been described. Rare individual reports of endometrial stromal nodule and low grade endometrial stromal sarcoma have also been describe [4, 5] (Table 1). Endometrial Stromal Nodules, which are considered a clinically benign tumors. They occur much more commonly in the corpus than in the cervix. They are frequently polypoid with protrusion into the uterine cavity but may be intra-myometrial (ranging up to 10 cm). They typically are well circumscribed and show a uniform tan to yellow, soft cut surface. Cyst formation as well as ischemic-type necrosis and hemorrhage may be seen. They are characterized microscopically by a well- circumscribed, pushing border; however, small irregularities present as lobulated or finger-like projections (<3 in number and <3 mm) into adjacent myometrium may occur [3, 6]. The neoplastic cells of ESNs resemble proliferative phase endometrial stroma, being composed of cells with uniform round to ovoid nuclei that have scant to moderate amounts of amphiphilic to eosinophilic cytoplasm. These cells appear to whorl around the prominent vascular component, which resembles the spiral arterioles of non-neoplastic endometrium. The vessels are typically evenly spaced and uniform in caliber throughout the neoplasm; however, occasionally large, thick-walled vessels may be present, although this is usually only a focal finding identified in only a minority of cases. ESNs can show variant morphology, most commonly smooth muscle differentiation, but unusual forms of differentiation including skeletal muscle may occur. Immunohistochemistry for vimentin, CD 10, and actions as well as WT1, ER, and PR are typically positive (rarely tumors may be CD 10 negative). Desmin and h-caldesmon are positive in areas of smooth muscle differentiation although occasionally areas of conventional stromal differentiation may be desmin positive, and if so, typically it shows a perinuclear cytoplasmic pattern of staining. Over 70% of tumors are positive for androgen receptors [7], and some investigators have shown nuclear β-catenin positivity [8]. Variable degree of keratin expression may be seen [9]. Areas of sex cord differentiation may be positive for inhibin, calretinin, CD99, melan A, and WT1 [10]. Histologically, ESN and LG-ESS are distinguished by the presence of stromal invasion. LG-ESS shows invasive patterns, whereas ESN does not. ESN has an expansive but noninfiltrative border that often compresses the surrounding myometrium and endometrium [11]. In the majority of cases, the distinction between an ESN and low-grade endometrial stromal sarcoma (LGESS) cannot be made with certainty in a curettage/biopsy specimen as the margin of the tumor usually cannot be assessed well or completely. In these cases, the diagnosis of ‘endometrial stromal neoplasia’ should be rendered with a note stating that the distinction between a nodule and a sarcoma cannot be made. Recent studies have shown that ESN and LG-ESS share common genetic alterations. As in LG-ESS, JAZF1- SUZ12 fusion is the most common rearrangement in ESN, estimated to be present in 65% of ESN cases [12].
| Author | Year | Age | Size (cm) | Gross Findings | Microscopic | IHC |
|---|---|---|---|---|---|---|
| Karpf, et al. [4] | 2007 | 28 | 5 | well circumscribed nodule | Non-infiltrative pushing border. Decidualization and myxoid change | Vimentin, CD10, PR positive. Ki67about 40% |
| Heller, et al. [5] | 2018 | 31 | 3.7x2,2x1.4 | well circumscribed nodule | Non-infiltrative pushing border | Vimentin, CD10, PR positive. CD31 focal |
| Present case | 2023 | 31 | 3.5x2.6x1 | well circumscribed nodule | Non-infiltrative pushing border. Decidualization and myxoid change | Vimentin, CD10, PR, WT-1 and B-catenin positive. Ki67 about 20% |
Table 1: Previous reports of endometrial stromal nodules in the placenta. IHC: Immunohistochemistry, CM: centimeter.
The diagnosis of endometrial stromal nodule was based on both its benign clinical behavior (no evidence of recurrence after a period of 12 months) and its pathologic features, which revealed a well circumscribed nodule with an expansive, non-infiltrative growth pattern, features characteristic of endometrial stromal tumors, such as CD10, progesterone receptor positivity, and plexiform vascularity. The diagnosis of leiomyoma was discarded owing to negativity for smooth muscle markers. Endometrial stromal tumors show a high histopathologic variability and indeed in this case the morphology was not entirely characteristic of ESN since there were focal degenerative myxoid and decidualized areas. These were interpreted as pregnancy- related changes. The variable but strong reactivity for CD10 may also be related to gestational stromal differentiation in which the usual endometrial stromal CD10 staining is known to be patchy or diminished. Uterine mesenchymal tumors continue to be a challenge to diagnose due to their non-specific clinical presentation, often non-distinctive gross appearance, varied (and many times overlapping) morphologic appearance, and unsuspected pitfalls in immunohistochemical expression. In the present case, the nodular tumor was entirely situated within the endometrial decidualized tissue; the expulsion of the placenta during delivery ensured the complete expulsion of the tumor attached to it, therefore proving curative, as confirmed by subsequent negative controls of the uterine cavity and the absence of any abnormal postpartum or puerperal bleeding. However, advised close follow-up with ultrasound control.
The pathologist must be aware that this lesion might involve the placenta in order to correctly identify it.
Author Contribution
The project was conceived by JPGT. The manuscript was written by RSO, with revision and intellectual input from AAR, and JPGT. Pathology slides and images were produced and annotated by RSO. Consent from the patient was obtained by AAR. All authors have read and approved the manuscript.
Ethics Approval and Consent to Participate
The patient has consented to the submission of the case report for submission to the journal.
Acknowledgment
We would like to thank all those who helped in the creation of this manuscript including the patient subject and the peer reviewers for their feedback and suggestions.
Funding
This study received no external funding.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Ali RH, Rouzbahman M (2015) Endometrial stromal tumours revisited: an update based on the 2014 WHO classification. J Clin Pathol 68(5): 325-332.
-
(2020) Female Genital Tumours: WHO Classification of Tumours. 5th (Edn.), IARC Publications, Lyon, France 4.
-
Dionigi A, Oliva E, Clement PB, Young RH (2002) Endometrial stromal nodules and endometrial stromal tumors with limited infiltration: a clinicopathologic study of 50 cases. Am J Surg Pathol 26(5): 567-581.
-
Karpf EF, Poetsch B, Langner C, Nogales FF, Regauer S (2007) Endometrial stromal nodule embedded into term placenta. APMIS 115(11): 1302-1305.
-
Heller DS, Hatem F (2018) Endometrial Stromal Neoplasm in the Placenta: Report of a Case and Review of the Literature. Int J Gynecol Pathol 37(1): 32-34.
-
Kurman RJ, Carcangiu ML, Herrington CS, Young RH (2014) WHO classification of tumours of female reproductive organs. 4th(Edn.), IARC, Lyon, 6.
-
Zadeh SL, Duska LR, Mills AM (2018) Androgen Receptor Expression in Endometrial Carcinoma. Int J Gynecol Pathol 37(2): 167-173.
-
Jung CK, Jung JH, Lee A, Lee YS, Choi YJ, et al. (2008) Diagnostic use of nuclear β-catenin expression for the assessment of endometrial stromal tumors. Mod Pathol 21(6): 756-763.
-
Rahimi S, Akaev I, Marani C, Chopra M, Yeoh CC (2019) Immunohistochemical expression of different subtypes of cytokeratins by endometrial stromal sarcoma. Appl Immunohistochem Mol Morphol 27(6): 466-470.
-
Irving JA, Carinelli S, Prat J (2006) Uterine tumors resembling ovarian sex cord tumors are polyphenotypic neoplasms with true sex cord differentiation. Mod Pathol 19(1): 17-24.
-
Conklin CMJ, Longacre TA (2014) Endometrial stromal tumors: the new WHO classification. Adv Anat Pathol 21(6): 383-393.
-
Ferreira J, Félix A, Lennerz JK, Oliva E (2018) Recent advances in the histological and molecular classification of endometrial stromal neoplasms. Virchows Arch 473(6): 665-678.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’