Use of Fetal Occiput – Spinal Angle at Early Active Phase of First Stage of Labour in Predicting the Labour Outcome – A Cross- Sectional Observational Study
Introduction: Fetal head deflexion plays an important role during the labour process and predicts the outcome of labour. Though traditionally it was assessed via digital examination, recent advancements in medicine have shown ultrasonographic parameters might be useful to measure of head flexion via fetal occiput-spine angle (OSA). Aim of this study was to evaluate its role. Method: We conducted a cross-sectional observational study on 292 uncomplicated singleton pregnant mothers without occiput posterior position. At early active phase of labour (OS= 4 – 6cm), angle between two tangential lines to the occipital bone and the vertebral body of the first cervical vertebra was measured as OSA. Labour progression and mode of delivery was monitored. Association between OSA and labour outcome along with the inter-observer difference was evaluated. Results: The mean OSA value was 133.88 ± 7.39°. The OSA measurement showed good inter-observer agreement (r = 0.99; p<0.001). The mean OSA was significantly less for the group of patients who had to undergo operative delivery (instrumental and cesarean) due to labour dystocia (n=37) as compared to women who had vaginal delivery (n=251), (128 ± 7.28° vs 134.83 ± 6.97°, P<0.001). The mean OSA was significantly greater for the group of patients who had a normal labour progression (n=32) as compared to women who had an abnormal progression (n=260), (134.67 ± 7.06° vs 127.47 ± 6.99°, P<0.001). Sonographic assessment of deflexion using OSA was found to be an independent predictor of labour outcome according to multivariate regression analysis. OSA value less than 127.8° was associated with abnormal labour progression and operative delivery with a good sensitivity of 86.5% & 85% respectively. However negative predictive value for operative delivery being 6.8%, suggests that multiple clinical parameters should be considered when the decision of caesarean section is made. Conclusion: Sonographic assessment of fetal head deflexion during early active phase can be used as reproducible, feasible screening parameter to predict labour progression and mode of delivery. Decision for operative delivery should be made using multiple clinical assessments.
Introduction
Most pregnancies have a successful outcome in having a spontaneous vaginal delivery. But some women experience abnormal labour during first and second stage needing obstetric interventions. It is found to be due to abnormalities in birth passage, passenger and/ or the power of uterine contractions [1, 2]. Even with adequate passage and powerful contractions, some fetuses are unable to have a normal vaginal birth. It is commonly due to malpresentation and malposition [3].
In vertex presentation fetus must undergo flexion, allowing chin to rest in chest, which make the wider occipito- frontal diameter to be suboccipito-bregmatic diameter of 9.5cm. Some fetuses in vertex presentation fail to achieve a fair degree of head flexion during first stage of labour which is essential for the correct alignment between fetal head and the widest diameter of the birth canal [4]. Currently, deflexed vertex presentations have become a frequent indication for operative vaginal and caesarean deliveries in labour across the world [5].
Three types of deflexed cephalic malpresentations has been described; sinciput, brow and face. Traditionally this is assessed via intrapartum vaginal examinations. However it’s been identified that digital assessment is inaccurate to diagnose fetal occiput position [6, 7, 8]. Therefore since recently, use of intrapartum ultrasonography has come into play as an indication for assessment of fetal malposition [9]. Usefulness of measuring various parameters such as angle of progression, progression distance, head-symphysis distance during second stage of labour has been evaluated and found to be effective in predicting of the labour outcome [10, 11, 12].
However as the assessments in second stage is difficult and sometimes uncomfortable to the mother who is in pain, need of a tool that can be assessed in early labour was emerged. Several studies found that assessment of fetal occiput-spinal angle (OSA) is a reliable ultrasonographic parameter as a measurement of degree of head deflexion [13]. It is measured trans-abdominally, as the angle between the fetal occiput and the fetal spine in the sagittal plane. It is a user friendly method which can be done at early labour with minimal discomfort to the mother [13].
Though few studies have been done to look for the association between the degree of fetal head flexion and labour outcome, the evidence is still controversial, especially on primi-gravida and Asian population. And also several studies have reported various but closely similar cut off values to OSA that adversely affect the labour outcome.
Hence, this study was designed to assess whether the measurement of fetal OSA, as determined by sonographic evaluation, can predict of the mode of delivery and abnormal labour among a group of primi and multiparous pregnant women. We also assessed the reliability of the measurement by developing a cut-off value and assessing the inter- observer variability, thereby, to determine its usefulness in clinical application to improve quality of obstetric care.
Method
This was a cross-sectional observational study conducted among pregnant women admitted to the labour ward of a maternity unit at a tertiary care Teaching Hospital in Sri Lanka between August and December 2023. Study was approved by the Ethics Review Committee of the Post- graduate Institute of Medicine, University of Colombo, Sri Lanka.
Inclusion Criteria
• Live singleton pregnancies in cephalic presentation and left/ Right / Direct Occipito-anterior or transverse position.
• Term pregnancies in 37 to 41 weeks of gestation as determined by the expected date of delivery using the Last Menstrual Period (LMP) date or dating ultrasound scan.
• Maternal age between 18yrs to 40 yrs.
• Mothers in early active phase of first stage of labour (4- 6cm cervical dilatation) with spontaneous or induced uterine contractions of 2 to 3 in every 10 minutes.
• Fetal head station above level 0 assessed by vaginal examination.
• With intact membranes or with membrane rupture for less than 24hrs.
Exclusion Criteria
• Diagnosed small or large for gestational age by antenatal ultrasound scan.
• Known fetal anomalies.
• Compromised fetuses with abnormal heart rate/ cardiotocography (CTG) at the beginning of labour.
• Occipito-posterior position of fetus.
• Complicated vaginal deliveries with placenta previa and previously scared uterus.
• Pregnancies complicated with pre-eclampsia, heart disease, liver disease and renal disease.
• Mothers with preterm labour or with membrane rupture for more than 24hrs.
Pregnant women who fulfilled the above inclusion and exclusion criteria were recruited to the study following obtaining informed written consent with convenient sampling. At early labour (active phase of 1st stage ), when cervical OS is 4 – 6cm dilated, they underwent a trans- abdominal ultrasound scan using a portable Samsung Medison H60 ultrasound machine equipped with a 4-7MHz trans-abdominal two-dimensional convex transducer. Images with fetal head and cervical spine were acquired to measure the fetal occiput-spinal angle, which is the angle formed by the conjunction of two tangential lines; one line across the fetal occipital bone and the other, across the body of the first cervical vertebrae. It was measured by two independent experienced sonographers, 2 times in separate images.
Labour process was observed using partogram. The health care team involved in labour management was blinded to the measurement of occiput-spinal angle. Mothers who underwent caesarean delivery due to fetal distress were excluded from further assessment.
Abnormal labour was defined as; prolonged 1st stage of labour with <2cm dilatation for 4hrs duration in primigravida and <2cm dilatation for 4hrs or slowing of progression in multigravida or, arrest of cervical dilatation or, arrested fetal head decent for more than 2hrs. Prolonged 2nd stage of labour was defined as >2hrs in primigravida & >1hr in multigravida with good contractions and adequate pushing.
Data analysis was done using SPSS statistical software. Pearson’s correlation coefficient was used to assess inter- observer difference. The mean of OSA measured by 2 operators were taken for subsequent analysis. Comparison of continuous variables between modes of delivery and labour outcomes was done using student- t test, while categorical variables were compared using chi square test. P value of <0.05 was considered as statistically significant. Area under the Receiver Operator Characteristics (ROC) curve was used to assess the value of OSA in predicting abnormal labour and mode of delivery.
Results
Overall 292 participants were included in the study out of which, 251 had vaginal delivery (VD) and 41 had operative delivery (caesarean and instrumental). Among them 4 had caesarean Delivery (CD) due to fetal distress and were excluded from further analysis and 20 had CD due to labour dystocia. We compared the demographic characteristics; gestational age, BMI, maternal age, parity among women who had VD vs operative delivery and also normal vs abnormal labour. All groups didn’t have difference and were comparable.
The abnormal labour group showed significant difference against normal labour group in terms of; increased duration of labour (405.31 74.74 vs 263.83 93.19 min), induction of labour, ruptured membranes, augmented labour and 1 min APGAR score (9.53 0.56 vs 9.82 0.69).
When compared to VD, the operative delivery group showed significant statistical difference with regard to; spontaneous onset of labour (11.6% vs 88.4%), ruptured membranes, labour duration, augmented labour and 1 min APGAR score (9.44 0.67 vs 9.84 0.67).
The percentage of different positions of occiput positions were as: anterior (2.8%), right-transverse (14.4%), right anterior (7.2%), left transverse (31.5%), and left anterior (43.8%). The OSA measurements for those groups didn’t show significant statistical difference.
The comparison between women who had vaginal delivery and operative delivery due to labour dystocia is shown in Table 1, together with the comparison between women who had normal labour process and abnormal labour process.
The mean value of the OSA for the study population was 133.88 7.39°. The mean OSA in the group of women with vaginal delivery (134.83 6.97°), was significantly greater than the group of women who had operative delivery (128 7.28°); P<0.001, as shown in Table 1.
| Characteristics | All (n=292) | Labour Normal (n=260) | Labour Abnormal (n=32) | P* | VD (n=251) | Caesarean+ Instruments+ Forcep (n=37) | P* | |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 28.05±4.79 | 28.13±4.75 | 27.41±5.18 | 0.42 | 28.17±4.80 | 27.37±4.75 | 0.32 | |
| BMI(kg/m2) | 23.32±1.68 | 24.33±1.71 | 23.27±1.48 | 0.86 | 23.36±1.75 | 23.06±1.15 | 0.15 | |
| Gestational age at delivery(weeks) | 39.12±0.65 | 39.11±0.66 | 39.20±0.63 | 0.46 | 39.10±0.65 | 39.24±0.69 | 0.21 | |
| Level of education | <OL | 5 | 4/5 (80.0%) | 5-Jan (20.0%) | 0.3 | 5-Aprl (80.0%) | 5-Jan (20.0%) | 0.48 |
| OL | 25 | 24/25 (96.0%) | 25-Jan (4.00%) | 24/25 (96.0%) | 25-Jan (4.00%) | |||
| AL | 193 | 174/193 (90.2%) | 19/193 (9.8%) | 165/193 (85.5%) | 28/193 (14.5%) | |||
| Degree | 69 | 58/69 (84.1%) | 11/69 (15.9%) | 58/69 (84.1%) | 11/69 (15.9%) | |||
| Induced labour | Yes | 43 | 33/43 (76.7%) | 10/43 (23.3%) | 0.005 | 31/41 (72.1%) | 12/41 (27.9%) | 0.01 |
| No | 249 | 227/249 (91.2%) | 22/249 (8.8%) | 220/247 (88.4%) | 29/247 (11.6%) | |||
| Intact Membranes | Yes | 229 | 212/229 (92.6%) | 17/229 (7.4%) | 205/227 (89.5%) | 24/227 (10.5%) | 0 | |
| No | 63 | 48/63 (76.2%) | 15/63 (23.8%) | <0.001 | 46/61 (73.0%) | 17/61 (27.0%) | ||
| Duration | 273.33± 101.41 | 263.83± 93.19 | 405.31± 74.74 | <0.001 | 264.56± 94.61 | 369.76± 95.56 | ||
| Augmented | Yes | 121 | 91/121 (75.2%) | 30/121 (24.80%) | <0.001 | 91/119 (68.3%) | 30/119 (31.70%) | 0 |
| No | 171 | 169/171 (98.8%) | 2/171 (1.20%) | 163/169 (95.3%) | 8/169 (4.7%) | |||
| Station | 0 | 278 | 246/278 (88.5%) | 32/260 (11.5%) | 0.18 | 238/274 (85.6%) | 40/256 (14.4%) | 0.45 |
| 1 | 14 | 14/14 (100.0%) | 0/14 (0.00%) | 13/14 (92.9%) | 14-Jan (7.10%) | |||
| Perineal tears | Yes | 4 | 3/4 (75.0%) | 4-Jan (25.00%) | 0.365 | 4-Mar (75.00%) | 4-Jan (25.00%) | 0.53 |
| No | 288 | 257/288 (89.2%) | 31/288 (10.8%) | 248/284 (86.1%) | 40/284 (13.9%) | |||
| Maternal complications | 285 | 253/285 (88.7%) | 32/285 (11.3%) | 244/281 (85.6%) | 41/281 (14.4%) | |||
| Post-partum haemorrhage | 3 | 3/3 (100.0%) | 0/3 (0.00%) | 3-Mar (100.0%) | 0/3 (0.00%) | |||
| Retained placenta | 4 | 4/4 (100.0%) | 0/4 (0.00%) | 0.643 | 4-Apr (100.0%) | 0/4 (0.00%) | 0.56 | |
| APGAR score (at 1min) | 9.79±0.68 | 9.82±0.69 | 9.53±0.56 | 0.025 | 9.84±0.67 | 9.44±0.67 | 0 | |
| Parity | 1 | 152 | 125/152 (82.2%) | 27/152 (17.8%) | 118/148 (77.6%) | 34/148 (22.4%) | ||
| 2 | 95 | 91/95 (95.8%) | Apr-1995 (4.20%) | 89/95 (93.7%) | Jun-1995 (6.30%) | |||
| 3 | 34 | 33/34 (97.1%) | Jan-1934 (2.90%) | 33/34 (97.1%) | Jan-1934 (2.90%) | |||
| 4 | 9 | 9/9 (100.0%) | 0/9 (0.00%) | 9-Sep (100.00%) | 0/9 (0.00%) | |||
| 5 | 2 | 2/2 (100.0%) | 0/2 (0.00%) | 2-Feb (100.00%) | 0/2 (0.00%) | |||
| Occiput spine angle (OSA) | 133.88± 7.39 | 134.67± 7.06 | 127.47±6.99 | <0.001 | 134.83±6.97 | 128.00±7.28 | 0 | |
| Birth weight(grams) | 2986±326 | 2988±331 | 2972±287 | 0.791 | 2993±331 | 2949±301 | 0.42 | |
| NICU admission | Yes | 4 | 4/4 (100.0%) | 0/4 (0.00%) | 0.48 | 4-Apr (100.00%) | 0/4 (0.00%) | 0.42 |
| No | 288 | 256/288 (88.9%) | 32/288 (11.1%) | 247/284 (85.8%) | 41/284 (14.2%) | |||
| Occiput Position | LOA | 128 | 114/128 (89.1%) | 14/128 (10.9%) | 109/126 (85.2%) | 19/126 (14.8%) | ||
| LOT | 92 | 84/92 (91.3%) | Aug-1992 (8.70%) | 82/90 (89.1%) | 10/90 (11.1%) | |||
| OA | 8 | 8/8 (100.0%) | 0/8 (0.00%) | 8-Jul (87.50%) | 8-Jan (12.50%) | |||
| ROA | 21 | 21/21 (100.0%) | 0/21 (0.00%) | 20/21 (95.2%) | 21-Jan (4.80%) | |||
| ROT | 43 | 33/43 (76.7%) | 10/43 (23.3%) | 33/43 (76.7%) | 10/43 (23.3%) |
Table 1: Maternal, obstetric, and newborn characteristics stratified by type of labour progression and type of delivery, after ex
The mean OSA in the group of women with normal labour process (134.67 7.06°), was significantly greater than the group of women who had abnormal labour process (127.47 6.99°); P<0.001) (Table 1).
With regard to mode of delivery, the area under the ROC
curve for the prediction of vaginal delivery was 0.761 (Figure 1). When focused on labour process, the area under the curve for the prediction of normal labour process was 0.771 as shown in (Figure 2).
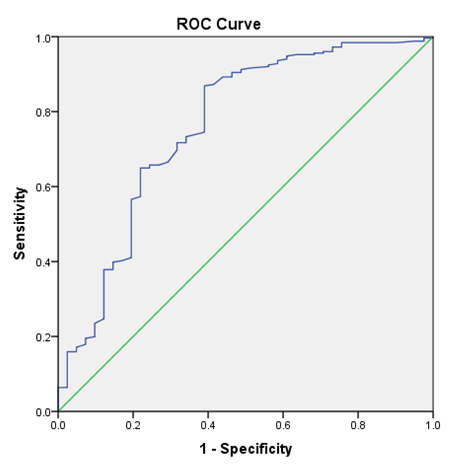
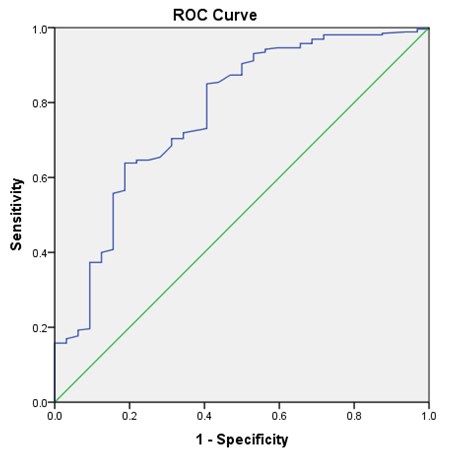
When both figures were analyzed, cut-off value of 127.8° was derived and was tested for its ability to differentiate between normal vs abnormal labour process and also for the mode of delivery. This value had a sensitivity of 86.5%, a specificity of 61% in predicting vaginal delivery with a positive predictive value of 56.9% and a negative predictive value of 6.8%. And it also showed a sensitivity of 85%, a specificity of 59.4% in predicting normal labour progression with a positive predictive value of 94.4% and a negative predictive value of 32.8%.
Multivariable logistic regression analysis confirmed that narrow OSA was associated with a greater risk of operative delivery (OR=0.909, 95% CI – 0.851 – 0.971, p<0.004) (Table 2) and for having an abnormal labour (OR=0.9, 95% CI – 0.830 – 0.976, p<0.011) (Table 3). Variables that didn’t show significance during univariate logistic regression were not analyzed during multivariate analysis.
| Maternal and Obestetric characteristics | Odds ratio | P value | 95% confidence interval |
|---|---|---|---|
| Parity | 0.077 | ||
| 1 | 0.237 | 0.008 | 0.082-0.689 |
| 2 | 0.202 | 0.138 | 0.024-1.669 |
| 3 | 0 | 0.999 | 0 |
| 4 | 0 | 0.999 | 0 |
| OSA | 0.909 | 0.004 | 0.851-0.971 |
| Duration | 1.005 | 0.072 | 0.000-1.011 |
| Effacement | 0.932 | 0.143 | 0.847-1.024 |
| Dilatation | 0.779 | 0.586 | 0.317-1.915 |
| Intact Membranes | 0.81 | 0.726 | 0.250-2.626 |
| Induced labour | 1.356 | 0.538 | 0.514-3.581 |
| Augmented labour | 1.827 | 0.319 | 0.558-5.984 |
| APGAR at 1 min | 0.691 | 0.104 | 0.443-1.078 |
| Parity | 0.21 | ||
| 1 | 0.258 | 0.044 | 0.191-2.087 |
| 2 | 0.137 | 0.111 | 0 |
| 3 | 0 | 0.999 | 0 |
| 4 | 0 | 1 | 1.126-23.041 |
| OSA | 0.9 | 0.011 | 0.830-0.976 |
| Duration | 1.012 | 0.003 | 1.004-1.020 |
| Effacement | 1.002 | 0.968 | 0.892-1.126 |
| Dilatation | 1.211 | 0.755 | 0.364-4.031 |
| Membranes intact | 0.394 | 0.252 | 0.080-1.940 |
| Induced labour | 1.172 | 0.806 | 0.330-4.159 |
| Augmented | 4.365 | 0.11 | 0.715-26.646 |
Table 2: Multivariable logistic regression in the prediction of instrumental & caesarean delivery due to labour dystocia.
The OSA measurement showed a positive linear relationship between the OSA measurements by two observers. Also there was no significant difference between the values observed by two observers according to independent sample T test. The mean difference was 0.1238° (CI=-1.3256, 1.0780).
Discussion
Traditionally, degree of fetal head deflexion has been assessed by vaginal examination and has been used as parameter to predict the progression and the outcome of labour. Since recent advancements, trans-abdominal and trans-perineal ultrasonography have been identified as useful to predict labour outcome, but most are assessed at second stage [10, 11, 12, 13].
Better understanding of the association and persistence of the head deflexion will be useful for healthcare professionals to target and guide the management in a patient centered approach and address abnormal labour progression and difficult deliveries early, to minimize maternal and fetal morbidity and mortality. It will result in favorable labour and pregnancy outcome. Multiple recent studies have found that assessment of OSA is a reliable, user friendly ultrasonographic parameter to assess degree of head deflexion [13].
In this study, we evaluated the ability of using OSA measured at the early active phase of labour when the cervical OS is between 4 – 6cm, in prediction of labour process and mode of delivery. Analyzing the area under the curve of ROC, revealed a cut-off OSA value of 127.8° to predict operative delivery and to predict abnormal progression of labour. This cut-off value is in close relation to the values detected by other studies; Somu et al who have used only nulliparous women to the analysis have reported 121° as the cut-off value to predict labour arrest and caesarean section [14, 15]. Meanwhile Ghi, et al. have reported 125° and Maged, et al. [16] reported cut-off to be 126° [13]. Fattah, et al. also have reported a value of 126° [15].
In accordance to the previous study results of OSA being a tool with good reliability, we also have found that inter- observer agreement is fairly good with the difference being 0.12°.
Regarding labour progress, we found abnormal progress in 35.1% when the OSA was less than 127.8° while it was 5.5% when the angle was 127.8° or more which means that with decreasing angle, there is an increase in the probability of abnormal labour. Regarding mode of delivery, we found operative delivery in 46.4% when the OSA was less than 127.8° while it was 6.8% when the angle was 127.8° or more which means that with decreasing angle there is an increase in the probability of instrumental or caesarean delivery.
Maged, et al. [16] reported the sensitivity and specificity of the cut-off of 126° to predict vaginal delivery to be as 78.4% and 93.79%, respectively, while that of ours for a cut- off of 127.8° was 86.5% and 61%, implying that our cut-off had greater sensitivity, while theirs had better specificity.16 Therefore, accounting for the risk of operative delivery, if the OSA is around 126° to 127° could be considered as a reasonable guide for clinicians. But our study showed that the negative predictive value for operative delivery is very low, which suggests that clinical assessment with multiple parameters should be considered when the decision of operative delivery is made rather than just depending only on the OSA value.
As we didn’t include fetal occiput posterior positions, we didn’t analyze the association between OSA and occiput positions.
In our study, overall incidence of maternal complications, tears and fetal complications were 2.4%, 1.4% and 1.4% respectively. With regard to OSA cut off groups, there was no difference between each other on maternal & fetal complications nor perineal tears.
Several other studies have also shown similar results with regard to OSA measurement and predicting the labour outcome [16, 17, 18].
This is the only study with more than 200 participants reported in the literature so far. Including both nulliparous and multiparous mothers, and having analyzed the association of OSA with regard to mode of delivery and as well as to the labour progression are the strengths of our study.
However being a single-centered study is one of the limitations. Further research conducted across multiple centers with even more greater number of participants will give more details. Further, we have excluded cases of fetuses in the occiput–posterior position. Therefore, a degree of selection bias might apply to this study. However, as the measurement of the OSA is technically difficult in occiput posterior position, even if we included it, it might cause error in results. And also even if we manage to obtain a correct value, practical implication would be difficult in clinical practice.
Conclusion
Our study attempted to establish the association between the OSA and progression of labor, mode of delivery, maternal and fetal complications. We have found that, considering the labour progression and the mode of delivery, the best cut- off for OSA was 127.8°. Value being below this angle, there is a significant increase risk of abnormal labour progression and instrumental & caesarean delivery though we didn’t observe significant rise in the incidence of maternal and fetal complication.
Narrow OSA suggests deflexion of the fetal head and at higher the degree of deflexion, we observed higher need of operative interventions due to labour dystocia. It appears from our data that it is a good clinical tool with a good inter- observer agreement. It supports the idea of obstetrics that deflexed fetal head can be assessed ultrasonographically and taken into practice to predict risk of labour dystocia and need of obstetric intervention. However decision of operative delivery should be made using multiple clinical parameters.
Acknowledgements
- All the doctors, nursing and health care assistant staffs who were involved in the study and the patient care.
- Patients and their family members.
Disclosure of Interest
None
Contribution to Authorship
Dr J.T.N. Senevirathne was the investigator and was involved in data collection and OSA measurements with Dr. S.M. Shafraz, Dr. D.Y. Watthuhewa and Dr. S.V.P.N. Thushara. Dr P.H.P. de Silva, Dr R. Silva, Dr. C, Mathota were Obstetrician & Gynaecologists who managed the patients. Mr. N.A.K.S.R. Kumara was the statistician involved in statistical analysis.
Funding
None
References
-
World Health Organization (2020) WHO labour care guide: user’s manual.
-
National Institute for Health and Excellence (2014) Intrapartum care for healthy women and babies.
-
Towner D, Castro MA, Eby-Wilkens E, Gilbert WM (1999) Effect of Mode of Delivery in Nulliparous Women on Neonatal Intracranial Injury. N Engl J Med 341(23): 1709-1714.
-
Kilpatrick S, Garrison E (2012) Normal labor and delivery. In: Eric G, Jauniaux RM, Driscoll DA (Eds.), Obstetrics Normal and Problem Pregnancies 6th(Edn.), Elsevier Saunders, Philadelphia, USA, Pp: 662.
-
Laughon SK, Branch DW, Beaver J, Zhang J (2012) Changes in labor patterns over 50 years. Am J Obstet Gynecol 206(5): 1-9.
-
Chou MR, Kreiser D, Taslimi MM, Druzin ML, El-Sayed YY, et al. (2004) Vaginal versus ultrasound examination of fetal occiput position during the second stage of labor. Am J Obstet Gynecol 191(2): 521-524.
-
Malvasi A, Tinelli A, Barbera A, Eggebø TM, Mynbaev OA, et al. (2014) Occiput posterior position diagnosis: vaginal examination or intrapartum sonography? A clinical review. J Matern Fetal Neonatal Med 27(5): 520- 526.
-
Akmal S, Kametas N, Tsoi E, Hargreaves C, Nicolaides KH, et al. (2003) Comparison of transvaginal digital examination with intrapartum sonography to determine fetal head position before instrumental delivery. Ultrasound Obstet Gynecol 21(5): 437-440.
-
Gustapane S, Malvasi A, Tinelli A (2018) The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol 218(5): 540-541.
-
Molina FS, Nicolaides KH (2010) Ultrasound in labor and delivery. Fetal Diagn Ther 27(2): 61-67.
-
Eggebø TM, Hassan WA, Salvesen KA, Lindtjørn E, Lees CC, et al. (2014) Sonographic prediction of vaginal delivery in prolonged labour: a two-center study. Ultrasound Obstet Gynecol 43(2): 195-201.
-
Ghi T, Maroni E, Youssef A, Morselli-Labate AM, Paccapelo A, et al. (2014) Sonographic pattern of fetal head descent: relationship with duration of active second stage of labour and occiput position at delivery. Ultrasound Obstet Gynecol 44(1): 82-89.
-
Ghi T, Bellussi F, Azzarone C, Krsmanovic J, Franchi L, et al. (2016) The “occiput–spine angle”: a new sonographic index of fetal head deflexion during the first stage of labor. Am J Obstet Gynecol 215(1): 84-85.
-
Somu K, Sujatha BS, Hebbar S, Shyamala G, Pai MV, et al. (2019) Sonographic assessment of fetal head deflexion using occiput spine angle measured during first stage of labour and its role in predicting the mode of delivery among nulliparous women. Int J Reprod Contracept Obstet Gynecol 8(8): 3025-3030.
-
Elfattah AAM, Gebril MM, Taha WS (2020) Measurement of the Fetal Occiput-Spine Angle as a Predictor of Labor Outcomes during the First Stage of Labor. Al-Azhar International Medical Journal 1(9): 210-223.
-
Maged AM, Soliman EM, Abdellatif AA, Nabil M, Said OI, et al. (2018) Measurement of the fetal occiput-spine angle during the first stage of labour as predictor of the progress and outcome of labour. J Matern Fetal Neonatal Med 32(14): 2332-2337.
-
Bellussi F, Livi A, Cataneo I, Salsi G, Lenzi J, et al. (2020) Sonographic diagnosis of fetal head deflexion and the risk of cesarean delivery. Am J Obstet Gynecol MFM 2(4): 100217.
-
Kamel R, Youssef A (2018) How reliable is fetal occiput and spine position assessment prior to induction of labour. Ultrasound Obstet Gynecol 53(4): 535-540.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’