Fetal Intra-Abdominal Cysts - Accuracy of Prenatal Ultrasound Diagnosis
Intra-abdominal cysts are commonly seen on prenatal ultrasounds. They are derived from different organ systems. Differentials include renal, hepatic, mesenteric, ovarian cysts, choledochal cysts and many others. Postnatal course may vary from asymptomatic lesions to life threatening conditions. Thus the need for prenatal diagnosis which helps in predicting the clinical outcome and formulating the perinatal management. The objective of our study was to determine the accuracy of prenatal ultrasound in identifying fetal intra adbominal cysts and it’s correlation with postnatal radioimaging. We concluded that indeed prenatal ultrasound is effective tool to predict the occurrence and nature of intra abdominal cysts. Ultrasound is freely available as compared to Fetal MRI and is having high level of accuracy. With advances in ultrasound diagnosis, Fetal medicine centres are better equipped to manage these cases. Antental diagnosis of fetal intrabdominal cysts helps in preparation of the parents, involvement of neonatology and related disciplines; thereby optimizing the perinatal outcome.
Introduction
Intra-abdominal cysts are commonly seen on prenatal ultrasound. They can have origin from various organs. Thus the many differentials include renal, hepatic, mesenteric, ovarian, choledochal cysts and many others [1, 2]. Intra-abdominal cysts originating from urogenital and gastrointestinal malformations are the most common [3, 4]. Adrenal cysts, splenic cysts, hydrocolpos, urachal cysts and chylous ascites are seen less frequently [1, 2].
Likely diagnosis may be established depending on size, shape, location and fetal sex. This aids in predicting the clinical outcome and formulating the perinatal management. Postnatal course may vary from asymptomatic lesions to life threatening conditions. Thus, the need for prenatal detection.
In literature, it has been reported prenatal ultrasound can have upto 70% accuracy in diagnosis of fetal intra-abdominal cysts [1, 5].
The objective of our study was to determine the accuracy of prenatal ultrasound in identifying fetal intra- abdominal cysts and it’s correlation with postnatal radio imaging.
Material and Methods
The study involved the retrospective analysis of 36 patients who attended the fetal medicine clinic of a Tertiary Care Hospital in Oman from 2016 to 2022. The prenatal ultrasound in these cases showed fetal intraabdominal cysts. Characteristics like size, shape, consistency, location (depending on abdominal quadrant and proximity to other organs) were described for each of these cysts and likely diagnosis was made on prenatal scan. Where ever possible these findings were correlated with postnatal scan. All cases had detailed anomaly scan by Fetal Medicine Consultant on Philips IU22 machine.
Results
Out of 36 cases (Table 1) with prenatal diagnosis of fetal intraabdominal cysts, 34 delivered in our hospital, 2 delivered elsewhere and hence were lost for follow up. Mean maternal age was 31.5 years. A female preponderance was noted amongst the fetuses, constituting 21 out of the 36 cases and amounting to 58%. The most common gestational age at diagnosis was 31 weeks. Maximum cases were diagnosed between the gestational ages 27- 33 weeks. Most of them delivered beyond 37 weeks. Only 7 babies were born preterm. 12 out of the 34 babies were delivered abdominally giving a caesarean section rate of 35.2 %. However, it was noted that the diagnosis of fetal intraabdominal cyst did not contribute towards the indications of the caesarean sections. Smallest cyst to be picked up measured 0.6 x0.9 cm whereas largest was 3.5 x 2.6 cm in diameter.
| Case | Maternal age yrs, parity | Gesta tional age in wks at diagnosis | USG Localization | Cyst diamet er (cm) | Additional findings | Antenatal diagnosis | Delivery, fetal outcome | Postnatal diagnosis | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 24 Primi | 38 | Unilocular right side of bladder | 1.9 x 1.7x 1.3 | - | D/D Omental cyst, duplication cyst, mesenchymal cyst, mesenteric cyst Female fetus | - | Delivered in other hospital | |
| 2 | 31 G4P3 | 31 | Intra-abdominal cyst between Intraumbilical vein and gall bladder | 1.2 x 1.1 | - | D/D Omental / peritoneal / GIT | NSD at 39 weeks, girl, 2600 grams | Hepatic cyst 1.3 x 0.8 cm in left lobe of liver | Referred to Pediatrics surgery |
| 3 | 26 Primi | 27 | Intra-abdominal cyst below right kidney | 1.2 | - | Fetal intraabdominal cyst | NSD at 38+ weeks, boy, 3140 grams | Well defined Anechoic cystic area 5.6 x 3.4 x 2.1 cm inferior to pelvis and anterior to urinary bladder D/D lymphangioma / duplication cyst | Referred to Pediatrics surgery |
| 4 | 30 G2P1 | 27 | Intra-abdominal cyst anterior and below kidney | 2.6 x 3.0 | - | Fetal intraabdominal cyst | NSD at 38+ week, boy, 2100 grams | Cyst abutting left kidney along lower pole and medial aspect | No intervention required |
| 5 | 29 G7P4 | 30 | Cyst at the right side of the bladder | 3.0 x 2.5 | - | Ovarian cyst | NSD at 37+ week, girl, 2800 grams | Unilocular cyst in right lumbar region scalloping inferior surface of liver / gall bladder On CT scan right ovarian cyst | Referred to Pediatrics surgery |
| 6 | 33 G4P3 | 25 | Intraumblical cyst between umblical vein and gall bladder | 3.4 x 2.4 | Fetal intraabdominal cyst | CS at 36+ weeks, girl, 2000 grams | Intraabdominal cystic lesion with septation at right hypochondrium, close to liver and gall bladder fossa | Referred to Pediatrics surgery | |
| 7 | 35 G4p2 | 28, 34 | Bladder outlet obstruction with cystic spaces around both kidneys | Renal dysplasia, anhydramni os | Bilatral urinomas with bladder outlet obstruction | 3.1 kg, male, nvd, | Bilateral enlarged kidneys with hydronephrosis and hydrureter, empty bladder | Neonatal death immediately after birth | |
| 8 | 43 G8P6A1 | 31 | Intraabdominal cyst between intrahepatic and umblical vein | 1.2 x 1.2 | Liver cyst | CS at 38+ weeks, girl, 2700 grams | 1.4 x 1 cm simple hepatic cyst in left lobe | Referred to Pediatrics surgery | |
| 9 | 44 G6P4 | 31 | Left to midline above the level of bladder ovarian origin | 1.6 x 1.9 | Ovarian cyst | NSD at 38+ week, girl, 2900 grams | Normal study | ||
| 10 | 42 G7P5A1 | 28 | Cyst posterior to stomach bubble and below the diaphragm | 1 X 0.8 | Repeat scan no cyst seen. | CS at 37+ weeks, girl, 2200 grams | |||
| 11 | 38 G5P4 | 26 | Intraabdominal cyst between gall bladder and umblical vein | 0.9 | Liver cyst | CS at 37+ week, girl, 4300 grams | Simple hepatic cyst 0.5 x 0.5 cm and 1.1 x 1.1 cm | Referred to Pediatrics surgery | |
| 12 | 27 Primigrav ida | 29 | Small clear cyst to right of spine below right kidney | Fetal intraabdominal cyst | NSD at 38+ weeks, boy, 3100 grams | Solitary abdominal cyst D/D mesenteric cyst / duplication cyst | Referred to Pediatrics surgery | ||
| 13 | 33 G6P4 | 29 | Umblical cyst | 1.9 x 2.5 | Umblical varix | CS at 34+ week, boy, 2080 grams | Portal vein and hepatic vein normal. | ||
| 14 | 28 G2P1 | 29 | Diverticulum? Partial duplication of gall bladder | Gall bladder diverticulum | NSD at 38+ week, girl, 2200 grams | Normal study | |||
| 15 | 29 G3P2 | 35 | Cystic structure on side of spine. Fluid collection around right kidney, bladder distended | 6 x 6 | Urinoma/ bladder outlet obstruction | NSD at 35+ weeks ,boy, 3200 grams | Bilateral hydronephrosis grade 2 &4. Large perinephric collection could represent subcapsular urinoma. Urinary bladder distended. Significant dilatation of bladder neck and posterior urethra. Bladder outlet obstruction | Referred to Pediatrics surgery | |
| 16 | 39 Primigrav ida | 31 | Umblical vein verix | 1.4 | Umblical vein varix | CS at 37+ week, girl, 2500 grams | Portal vein and hepatic vein normal. | ||
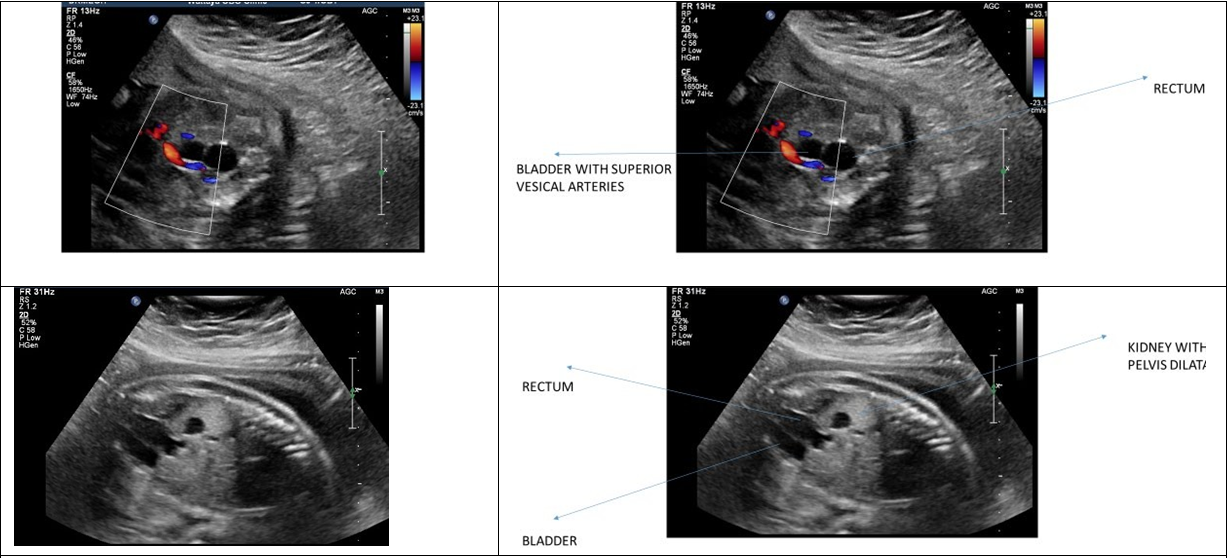
| 17 | 28 G2P1 | 27 And 31 | Elongated cystic area in lower abdomen behind bladder Rpt scan at 31 wks. rectal dilatation | Right kidney pelvic dilatation 1.6cm, Anal atresia | Dilated rectum Mega ureter | NSD at 37 weeks ,boy, 3770 grams | right mild to moderate hydrone phrouretosis with dilated right ureter upto distal aspect demonstrating abrupt narrowing in right iliac fossa.. possibly congenital mega ureter/ vesicoureteric reflex to be considered. Dilated rectum with anechoic lumen | Referred to Pediatrics surgery | |
| 18 | 24 Primi | 37 | Irregular cyst on the right side in anterior part of liver | 2.5 x 2 | Irregular intrahepatic cyst | NSD at 38+ weeks, boy , 2640 grams | Thin walled cystic lesion with internal sepatation 2.2 x 1.4 cm in right lobe of liver… hepatic cyst | Referred to Pediatrics surgery | |
| 19 | 24 G2P1 | 32 | Small cystic area in abdomen near the gall bladder | 1.5 | Origin from liver/ gall bladder | CS at 35+ weeks, twin boy, 1700 grams | Gall bladder twisted with septate( normal variant) |
Table 1: Differential Diagnoses of various prenatal intrabdominal cyst with Outcome at birth.
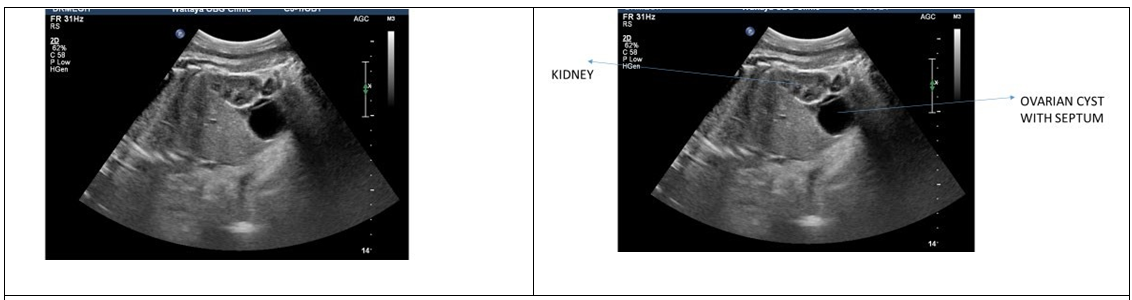
| 20 | 32 Primi | 31 | Cyst to the left of bladder. The septum echogenic area seen at 31 wks not seen at 36 wks | 4 x 4 | Ovarian cyst | NSD at 37+ week, girl, 3250 grams | 2.5 x 2.3 cm thin walled cyst no internal septate of solid nodule seen in abdominal cavity. No clear relation with abdominopelvic viscera, lying close to small bowel along right posterior lateral wall of urinary bladder. It is seen separate from small ovary and uterus. D/D solitary abdominal cyst/ duplication cyst/ mesenteric cyst | Referred to Pediatrics surgery | |
|---|---|---|---|---|---|---|---|---|---|
| 21 | 40 G5P3 | 27 | Intraabdominal cyst close to stomach bubble medially/ below the diaphragm. | 1.5 x 1 x 1 | Muscular Ventricular septal defect | D/D duplication cyst/ extra pulmonary CCAM/ mesenteric cyst / omental cyst / liver cyst | CS at 37+ week, girl, 3250 grams | Normal study | |
| 22 | 34 G2P1 | 30 34 wks | Intra abdominal cyst closed to stomach bubble. Between umblicalvein and gall bladder no communication between cyst and stomach bubble. | 2.5 x 2 3.7 x 2.6 x 4 | Mild Tricuspid regurgitation | Fetal intraabdominal cyst | Delivered in other hospital | ||
| 23 | 34 G6P3 | 30 | Cystic, solid, echogenic mass above left kidney and below diaphragm | 2 x 2 | D/D adrenal hemorrhage/ adrenal tumor, extra pulmonary sequestration / CCAM | CS at 30+ weeks, girl, 1330 grams | Multicystic hyperechoic left adrenal lesion ?. hematoma and neuroblastoma. ?? Extra lobar subdiaphragmatic pulmonary sequesteration | Referred to Pediatrics surgery For further onvestigations and managment | |
| 24 | 22 G3P2 | 33 | Clear intra abdominal cyst near to right of bladder | 3.5 x 2.6 x 2.4 | Ovarian cyst | NSD at 40+ week, girl, 3800 grams | D/D ovarian cyst/ duplication cyst/ mesenteric cyst t | ||
| 25 | 24 G2P1 | 30 | Clear cyst near to bladder | 2 x 1.7 | Ovarian cyst | NSD at 39+ week, girl, 3240 grams | Normal study | ||
| 26 | 24 G2P0 | 36 | Clear cyst with thin septa right side of abdomen | 3.5 x 3 x 3 cm | Ovarian cyst | NSD at 38+ week, girl, 3120 grams | Right adenexal simple, clear thin walled cyst mostly follicular cyst 1.1 1.2 x 1.5 cm | ||
| 27 | 39 G6P4 | 31 | Clear cyst behind the bladder. Pelvic region | 1.2 x 1.2 | 36 weeks no cyst seen | NSD at 38+ weeks, girl, 2700 grams | |||
| 28 | 35 G5P2 | 31 | Intra abdominal cyst irregular with septations At 35 weeks seen again. | 3 | Fetal intraabdominal cyst | NSD at 39+ weeks, girl, 3600 grams | Multiseptatic cyst seen in right hypochondrium. Bowel/ mesenteric / pancreatic cyst | Referred to Pediatrics surgery | |
| 29 | 44 G4P3 | 31 | Cyst left to midline above bladder At 33 weeks left of bladder with daughter cyst( 1.3 x 1.2 cm) | 1.6 x 1.9 2.3 x 2.1 | Ovarian cyst | NSD at 38+ weeks, girl, 3900 grams | Normal study | ||
| 30 | 37 G4P3 | 24 31 | Intra abdominal cyst medial to stomach bubble | 0.6 0.9 | Hepatic cyst | NSD at 39+ weeks, girl, 2600 grams | Septatic hepatic cyst around 1.3 x 0.6 cm in left lobe of liver | Referred to Pediatrics surgery | |
| 31 | 31 G2P1 | 27 34 | Cyst anterior and below left kidney Another small cyst either separate or communicating with this. | 2.6 x 3 | D/D duplication cyst/ mesenteric cyst / omental cyst | NSD at 38+ weeks, boy, 2100 grams | 1.6 x 1.6 cm cyst abutting left lower pole of left kidney | Referred to Pediatrics surgery | |
| 32 | 37 G4p2 | 22 28 34 | Iac ant very close to left kidney.one big cyst with two daughter cysts | 3x4 cm | Renal cysts/ non functioning moiety of kidney | NSD at 38+ weeks,mal e , 4200 grams | 3 thin wall unilocular cysts from lower pole of left kidney 2.2x2.6,0.9x0.7,0.5x 0.3. | Referred to Pediatrics surgery | |
| 33 | 25 G3P2 | 25 | Intraabdominal cyst on right of bladder. No bowel dilatation | 3 x 2 | Fetal intraabdominal cyst | NSD at 39+ week, boy, 3600 grams | Normal study | ||
| 34 | 27 Primi | 32 | Intra abdominal cyst | 1.5 x 1.7 | Hepatic cyst | CS at 34+ weeks, girl, 2000 grams | Simple hepatic cyst 1.9 x 1.4 cm | Referred to Pediatrics surgery | |
| 35 | 27 Primigrav ida | 29 | Clear cyst on right of spine below right kidney At 36 weeks right kidney inferior pole | 1 1 | Fetal intraabdominal cyst | NSD at 38+ weeks, boy, 3100 grams | Large anechoic cyst 5.6 x 3.4 x 2.1 cm in abdomen on right side extending to pelvis anterior to bladder. Lymphangioma / duplication cyst | Referred to Pediatrics surgery | |
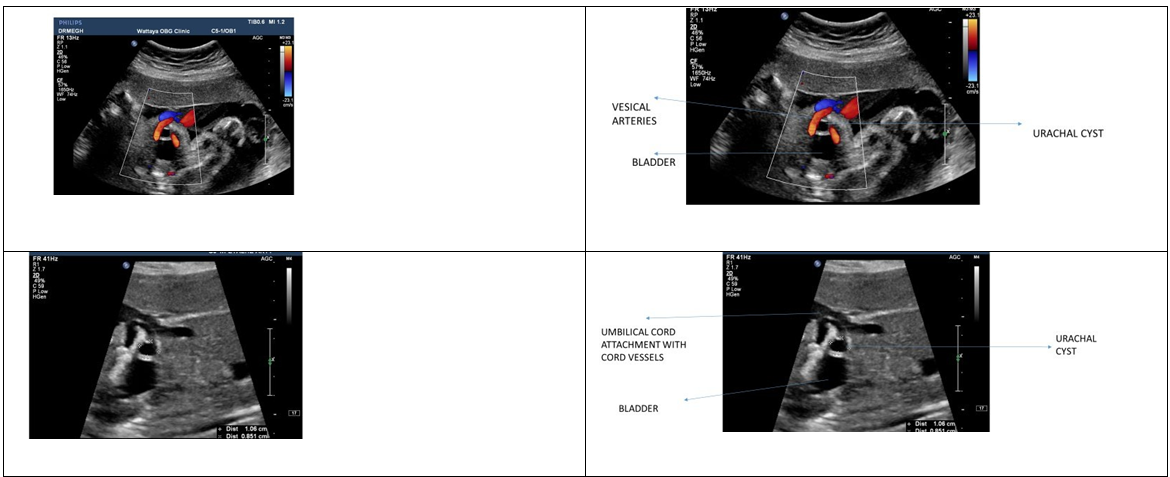
| 36 | 40 G2p1 | 27 | Small cystic area above bladder between two supvesical arteries | 7mm | Urachal cyst | Lscs male 38 weeks ,2800 gms | Urachal cyst |
Table 2: Differential Diagnoses of various prenatal intrabdominal cyst with Outcome at birth.
Spontaneous resolution of the intra-abdominal cyst was seen in 2 cases prenatally <5.8%>. Postnatal scan was unremarkable in 6 cases. In the remaining 26 cases, there was good correlation between pre and postnatal ultrasound findings giving ultrasound accuracy of 81.25 % (26/32 cases).
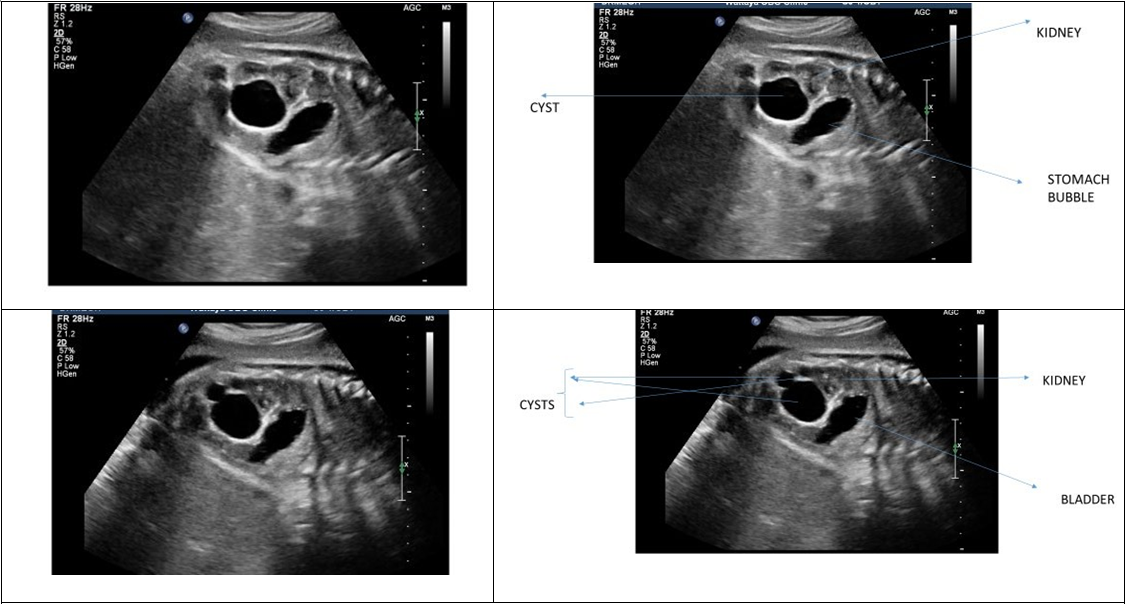
In our series we had 6 liver cysts (Figures 5 A,B), 2 urinomas (Figures 3 A,B), 1 renal cyst (Figure 6), 1 urachal cyst (Figure 8), 1 dilated rectum< secondary to anal atresia >(Figure 2) and 1case with suprarenal mass (Figure 1).
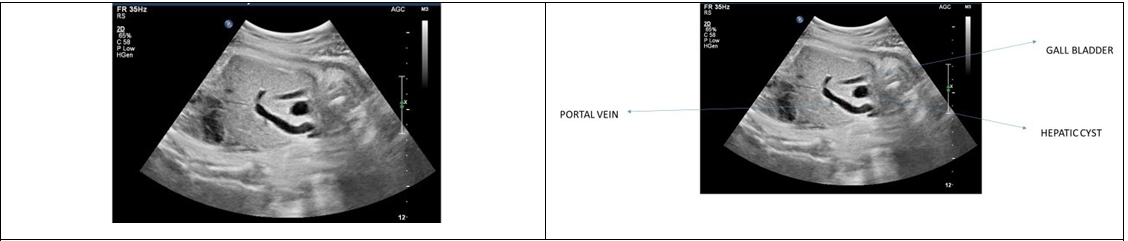
Figure 5A: Hepatic cyst.
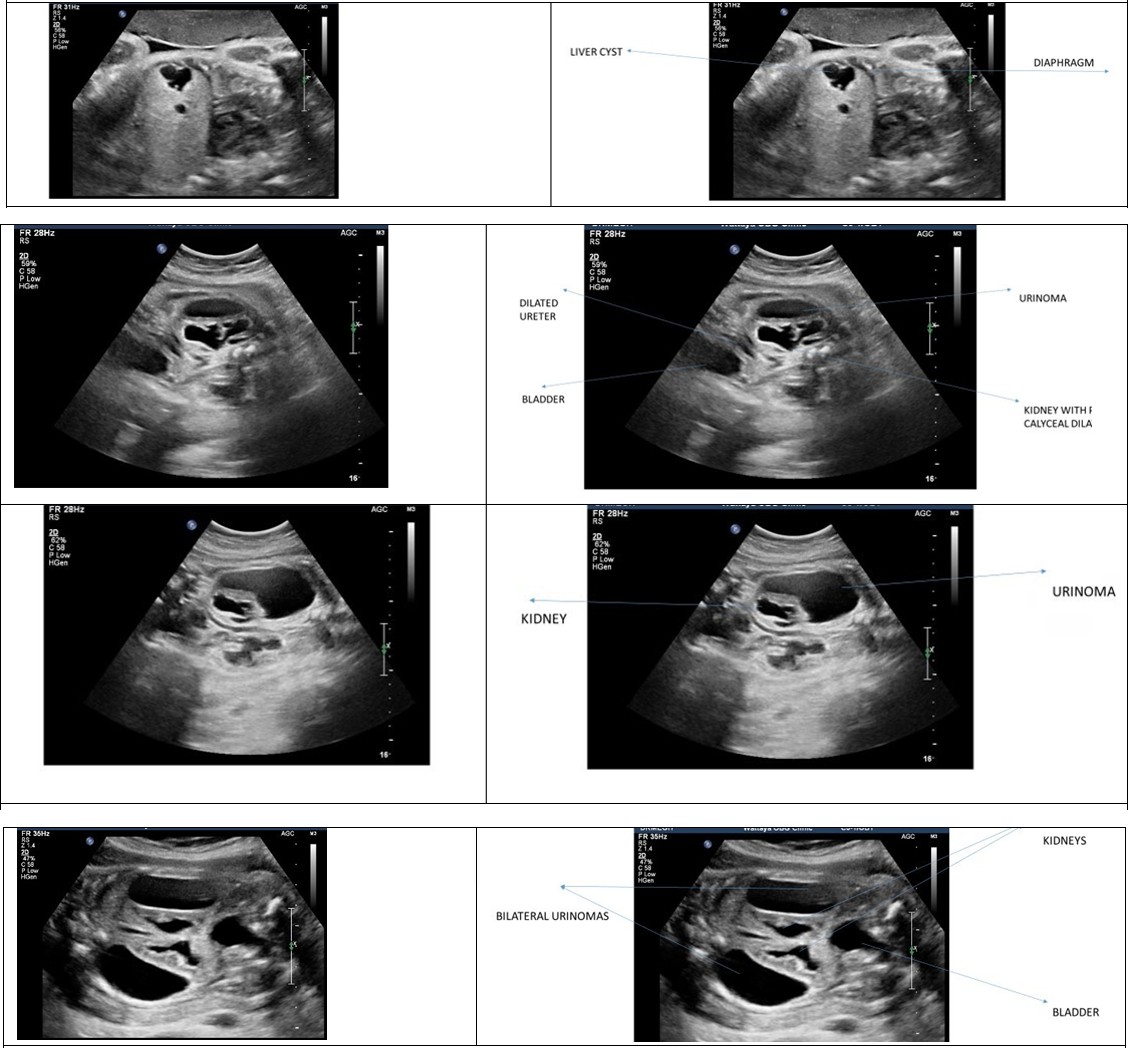
Figure 5B: Irregular hepatic cyst.
Figure 3A: Unilateral Urinoma.
Figure 3B: Bilateral Urinomas.
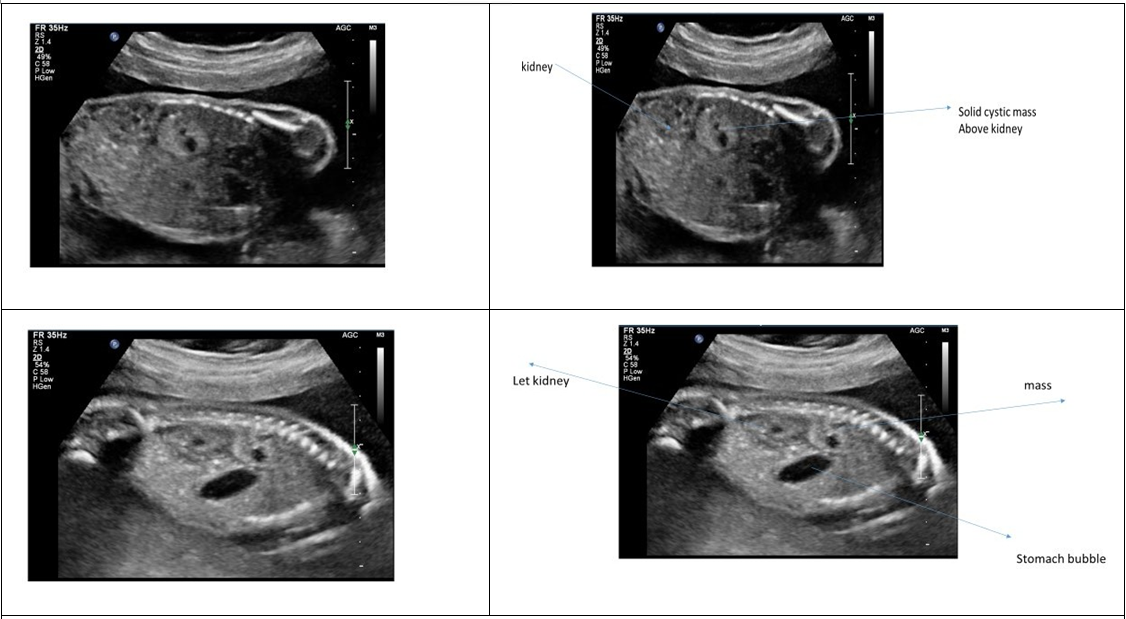
The case with suprarenal mass carried the same diagnosis postnatally. Prenatal differentials for the mass included adrenal hemorrhage/ neuroblastoma/extrapulmonary CCAM. Postnatal ultrasound also gave similar differentials for the same mass and the neonate was referred to pediatric surgeons for further investigations and management.
MRI done sometime later confirmed the presence of left involuted adrenal hemorrhage, luckily entailing conservative management only.
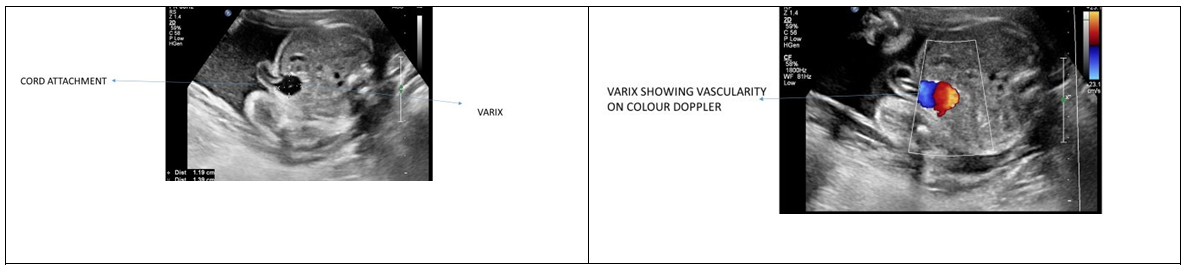
There were 2 cases of umbilical varix (Figure 7) but in both there was no dilatation of portal vein or hepatic vein.
We had 7 cases with prenatal diagnosis of ovarian cysts (Figure 4). 3 were confirmed postnatally as ovarian cysts and 1 case was assigned to be solitary abdominal cyst.
Postnatal ultrasound did not reveal any specific finding in the remaining 3 cases.
Amongst 14 cases of fetal abdominal cysts of nonspecific origin, 2 were lost for follow up and 2 resolved antenatally. Postnatally 6 were assigned to be solitary abdominal cysts occupying the same location as the prenatal scan, 2 were labelled as lymphangiomas/ duplications cysts. In the remaining 2 cases, no cysts were seen in postnatal ultrasound.
One case with prenatal gallbladder diverticulum was seen as normal variant in postnatal scan. Most of the cases in our series were managed conservatively in the neonatal life, apart from three cases. The case with anal atresia needed surgery soon following birth. Postnatal ultrasound in the case with unilateral urinoma showed bilateral hydronephrosis with large perinephric subcapsular urinoma on right side. Urinary bladder, bladder neck and posterior urethra were noted to be significantly dilated. The neonate was referred to paediatric surgeon for Bladder outlet obstruction and later underwent procedure for the same.
The other neonate with bilateral huge urinomas died immediately in postnatal period due to severe pulmonary hypoplasia and renal dysplasia. Our study shows 81.25 % accuracy between antenatal and postnatal ultrasound findings (Table 1). Most common in our study were liver cysts followed by ovarian cysts. The cysts that resolved spontaneously were the abdominal cysts of nonspecific origin.
Discussion
Incidence of fetal abdominal cyst is quoted around 1/1000 [6], mostly reported in female fetuses [6, 7]. Usually diagnosed in second trimester or third trimester [7, 8], nonetheless can be detected incidentally in the first trimester [6] as well.
Detection of fetal abdominal cyst is relatively easy but determining it’s origin is difficult [7]. Fetal intraabdominal cyst may be nonspecific having different ultrasound characteristics, varied locations that makes exact diagnosis, origin and prognosis unclear [7].
When defining the cyst, we can gain clues to the organ of origin by it’s location in the abdomen, the characteristic nature < solid, cystic, vascular, simple/complex, septate>, fetal gender and accompanying ultrasound findings such as presence of peristalsis in the cyst, presence of thick muscular wall, etc. These provide vital information for the diagnosis and management of the cyst [6, 7].
They can regress or grow progressively until being operated in the postnatal period. The prenatal and postnatal diagnosis may be discordant in some cases. All this may further add to the dilemmas thereby complicating counselling and management plan [7].
The many differential diagnoses include cysts originating from gastrointestinal tract (mesenteric, omentum, intestinal duplication, hepatic, biliary cysts and meconium pseudo- cysts) and genitourinary tract (ovarian, renal, urachal and adrenal cyst) [9]. Additionally, extra-abdominal pulmonary, spinal or retroperitoneal lesions can also resemble fetal intraabdominal cyst [7, 10].
Each of these Differentials have their Own Significance
Congenital hepatic cysts are rare [7]. In postnatal life, The incidence of congenital hepatic cyst is 2.5% and much less in prenatal life. Conversely, they were the commonest in our series. Once a hepatic cyst is diagnosed antenatally, perinatal surveillance should be undertaken to monitor the size of cyst and determine if surgery is necessary [11]. Symptoms depend on the size rather than the location of the cyst [12]. Ultrasound is most commonly used modality to monitor hepatic cyst [11, 12]. Management is usually conservative with necessity of surgery only in cases with progressive enlargement, hemorrhage, torsion and infection [13].
Cysts originating from gastrointestinal tract and hepatobiliary system are the most difficult to diagnose [6]. Amongst the fetal intraabdominal cyst, the most frequent to be diagnosed are the ovarian [7]. In numerous studies and case reports, many of the fetuses underwent surgery postnatally for ovarian torsion, hemorrhage, however did well postnatally. Spontaneous resolution has also been noted in postnatal life [6].
Congenital renal cysts can also be identified on prenatal ultrasound. In the absence of associated anatomical or chromosomal abnormalities, the majority of cysts will resolve antenatally without any sequelae [14]. Postnatally their diagnosis may be revised as hydronephrosis, multicystic dysplastic kidney, adrenal gland mass or unilateral atrophic kidney [15]. Hence the importance of prenatal diagnosis and follow up of fetal renal cysts.
Umbilical varix is seen on ultrasound as round / fusiform structure close to the bladder. Color Doppler helps in differentiating vascular anomalies from cord lesions. Diagnosis and surveillance is necessary as they may be associated with adverse outcomes including aneuploidies, structural defects, and still births.
Urachus is fibrous remnant of the allantois, forming a channel between the dome of bladder and umbilicus in the midline. Failure to obliterate portion of urachus leads to cyst formation seen as anechoic structure In between umbilicus and bladder in midline. Most disappear after delivery. They might be associated with anomalies of gut [2].
Prenatal cystic solid adrenal mass could be simple cyst, hemangioma or neuroblastoma. Simple cysts frequently resolve spontaneously. Congenital cystic neuroblastoma usual presentation is as mixed solid and cystic mass possibly due to hemorrhage or necrosis of the tumor and can mimic adrenal hemorrhage. Adrenal neuroblastoma is most common neonatal malignancy and antenatal diagnosis improves prognosis [2]. In our series the adrenal mass was eventually confirmed to be benign left adrenal hemorrhage and involuted spontaneously.
Imperforate anus is relatively common with incidence of 1/1500 to 1/5000 newborns [16, 17]. It may be isolated or can exist with other anomalies [18]. Prenatal diagnosis of imperforate anus is difficult. It is usually not diagnosed until after birth, Though can be picked up as early as 12 weeks of gestation [18]. On prenatal ultrasound, imperforate anus may appear as an intra-abdominal cyst [17], identical to our case. In our case, anal atresia with associated dilated rectum was seen as an elongated cystic structure seen behind the bladder. In this condition, at birth, immediate evaluation is necessary and important as decompressive surgery is necessary. Hence highlighting the role of antenatal diagnosis, prenatal counselling and management.
Antenatally diagnosed nonspecific fetal intra-abdominal cysts can have complicated management due to the varied nature of confirmed postnatal diagnoses like gut duplication, meconium pseudocyst, ovarian cyst, choledochal cyst, splenic cyst, Meckel’s diverticulum, liver cyst, hydronephrosis, patent urachus and many such others [19]. Hence mandating postnatal surveillance.
Sometimes there can be prenatal spontaneous resolution of these intrabdominal cysts. In literature, the rate of prenatal spontaneous resolution of fetal intra- abdominal cysts has been reported between 19% and 34.7% [19, 20]. Some reported upto 6% [5]. In our study we had 5.8 % rate of spontaneous resolution. Ultrasonographic features, predictive for spontaneous prenatal resolution of the cyst, are: small size, unilocular clear content and intra- parenchymal presence [5].
Commonly intrasplenic and intrahepatic cysts are known to resolve spontaneously. Spontaneous resolution is also reported for ovarian and mesenteric cysts. However adrenal lesions and gastrointestinal malformations are less likely to resolve spontaneously [5].
The finding of an intra-abdominal cyst may modify obstetric management and the site of delivery but rarely does it affect the time or mode of delivery. It helps in prenatal counselling and preparedness of prospective parents and multidisciplinary team [2, 19].
If isolated finding, they are usually associated with good postnatal outcome [21]. When fetal abdominal cyst are identified at the lower abdomen with additional anomalies, families should be informed of the probable association of lower gastrointestinal tract obstruction [7].
Neonatal with intra-abdominal cysts usually have a favorable outcome, with various authors quoting a mortality rate lower than 17%, despite the high prevalence of surgical procedures [5, 11, 19, 22]. In our series we had only 1 case with neonatal death (in fetus with renal dysplasia and pulmonary hypolplasia) giving perinatal mortality rate of 2.95%.
Prenatal ultrasound is universally and easily accessible (in contrast with prenatal MRI – which is not available readily) and yields sufficient amount of information as is necessary in giving the prognosis and aiding the management of such cases. Ultrasound is the preferred modality for diagnosis. MRI is less frequently used. However, can prove complementary when diagnosis is uncertain [23].
The etiology of fetal intra-abdominal cysts can be prenatally diagnosed in about 70% cases. Accuracy of ultrasound in identifying fetal intrabdominal cysts has been variedly quoted around 51.1% [24], 58.6% [6], 72.4% [1] and 74.6% [23].Our study reveals an accuracy rate as high as 81.25% in the identification of these cysts and their etiology.
Postnatal diagnosis is improving due to antenatal detection. Accurate prenatal diagnosis allows parent counseling and pre-delivery planning. Management of these lesions requires a specific planning to achieve diagnosis, treatment and follow-up. Anticipated antenatal diagnosis allows formulation of referral strategy to appropriate center with neonatal intensive care unit having availability of pediatric surgery services. This approach is helpful for early perinatal evaluation, facilitates admission to the neonatal intensive care unit, and immediate surgical treatment when indicated [5].
Conclusion
We concluded that indeed prenatal ultrasound is effective tool to predict the occurrence and nature of intra- abdominal cysts. Ultrasound is freely available as compared to Fetal MRI and is having good level of accuracy, as high as 81.25%. Antenatal diagnosis of fetal intrabdominal cysts helps in counseling, preparation of the parents, involving neonatology and related disciplines. This expedites the postnatal diagnosis and management thereby optimizing the perinatal outcome. With advances in ultrasonography, fetal medicine centres are better equipped to manage these cases and provide the best suited care to the prospective parents and fetuses.
References
-
Açıkgöz AS, Tuten A, Bulut B, Öncül M, Eskalen S, et al. (2015) Fetal Abdominal Cysts: Prenatal Diagnosis and Management. Gynecology & Obstetrics 5(9): 1-4.
-
McEwing R, Hayward C, Furness M (2003) Foetal cystic abdominal masses. Australas Radiol 47(2): 101-110.
-
Maudar C, Naware SS, Singh A, Puri B (2000) Foetal intra abdominal cyst: antenatal diagnosis and follow-up. Med J Armed Forces India 56(3): 237-239.
-
Tu CY (2017) Ultrasound and differential diagnosis of fetal abdominal cysts. Experimental and Therapeutic Medicine 13(1): 302-306.
-
Catania VD, Briganti V, Giacomo VD, Miele V, Signore F, et al. (2016) Fetal intra-abdominal cysts: accuracy and predictive value of prenatal ultrasound. J Matern Fetal Neonatal Med 29(10): 1691-1699.
-
Kahraman NC, Celik OY, Obut M, Arat O, Celikkan C, et al. (2022) Cysts of the fetal abdomen: Antenatal and postnatal comparison. J Med Ultrasound 30(3): 203-210.
-
Kumru P, Arısoy R, Erdoğdu E, Demirci O, Tozkır E, et al. (2014) The prenatal diagnosis and outcome of fetal intra-abdominal cysts. Perinatal Journal 22(3): SE11.
-
Bryant AE, Laufer MR (2004) Fetal ovarian cysts: Incidence, diagnosis and management. J Reprod Med 49(5): 329-337.
-
Hyett J (2008) Intra-abdominal masses: prenatal differential diagnosis andmanagement. Prenat Diagn 28(7): 645-655.
-
Laje P, Martinez-Ferro M, Grisoni E, Dudgeon D (2006) Intraabdominal pulmonary sequestration. A case series and review of the literature. J Pediatr Surg 41(7): 1309- 1312.
-
Sepulveda W, Dickens K, Casasbuenas A, Gutierrez J, Dezerega V (2008) Fetal abdominalcysts in the first trimester: prenatal detection and clinical signifi-cance. Ultrasound Obstet Gynecol 32(7): 860-864.
-
Celebi S, Kutluk G, Bestas CB, Kuzdan Ö, Sander S, et al. (2014) Current diagnosis and management of simple hepatic cysts detected prenatally and postnatally. Pediatr Surg Int 30(6): 599-604.
-
Recinos A, Zahouani T, Guillen J, Rajegowda B (2017) Congenital Hepatic Cyst. Clin Med Insights Pediatr 10: 11.
-
Blazer S, Zimmer EZ, Blumenfeld Z, Zelikovic I, Bronshtein M (1999) Natural history of fetal simple renal cysts detected in early pregnancy. J Urol 162(3 Pt 1): 812-814.
-
Sanna E, Derwig I, Loukogeorgakis S, Prior T, Paramasivam G, et al. (2017) EP12.30: Significance and outcome of simple renal cysts detected antenatally. Ultrasound Obstet Gynecol 50(S1): 309-310.
-
Cho S, Moore SP, Fangman T (2001) One hundred three consecutive patients with anorectal malformations and their associated anomalies. Arch Pediatr Adolesc Med 155(5): 587-591.
-
Brantberg A, Blaas HG, Haugen SE, Isaksen CV, Eik- Nes SH (2006) Imperforate anus: A relatively common anomaly rarely diagnosed prenatally. Ultrasound Obstet Gynecol 28(7): 904-910.
-
Sahiti M, Rethiman MK, Andrew C (2019) Fetal Abdominal Cyst. IOSR Journal of Dental and Medical Sciences 18(1): 1-4.
-
Sherwood W, Boyd P, Lakhoo K (2008) Postnatal outcome of antenatallydiagnosed intra-abdominal cysts. Pediatr Surg Int 24: 763-765.
-
Lecompte JF, Hery G, Potier A, Gorincour G, Giudicelli B, et al. (2014) Putative criteria for predictingspontaneous regression of prenatally diagnosed thoracoabdominalcystic lesions. Eur J Pediatr Surg 24: 426-429.
-
Taipale P, Rovamo L, Hiilesmaa V (2005) First-trimester diagnosis of imperforate anus. Ultrasound Obstet Gynecol 25(2): 187-188.
-
Ozyuncu O, Canpolat FE, Ciftci AO, Yurdakok M, Onderoglu LS, et al. (2010) Perinatal outcomes of fetal abdominal cysts and comparison of prenatal and postnatal diagnoses. Fetal Diagn Ther 28(3): 153-159.
-
Gai S, Wang L, Zheng W, Xu B, Luo Q, et al. (2022) Outcomes of sonographically-suspected fetal intra- abdominal cysts: Surgical intervention, conservative management and spontaneous regression. Front Pediatr 10: 1015678.
-
Hugele F, Dumont C, Boulot P, Couture A, Prodhomme O (2015) Does prenatal MRI enhance fetal diagnosis of intra-abdominal cysts? Prenat Diagn 35: 669-674.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’