Mucociliary Apparatus of the Fallopian Tubes, the Role of its Disorders in Inflammation and Infertility
The mucociliary apparatus (MCA) of the fallopian tubes (FT) is one of the key mechanisms that ensure the reproductive function of the female reproductive system. Its disorders play a huge role in the pathogenesis of diseases of the reproductive organs and infertility. Insufficient coverage and study of this problem initiated this work. For this purpose, a search and analysis of literary data was carried out using various scientific databases, including Index Medicus, PubMed, Embase, Cochrane Library and others for the period 1980 - 2024. The analysis made it possible to reflect the morphofunctional, structural and genetic features and other important aspects of the MCA FT in an original aspect. The influence of various factors on the MCA, the mechanisms of development of pathological processes and the causes of infertility are shown. The state of the MCA FT against the background of monogenic and multifactorial diseases is reflected. In conclusion, we note that the role of MCA FT disorders in the development of the pathological process and infertility is significant and eserves close attention, since they are often not diagnosed by standard methods and require the use of targeted morphofunctional research methods for their verification. The prospects for diagnostics and correction of MCA FT disorders are considered.
Abbreviations
MCA: Mucociliary Apparatus; FT: Fallopian Tubes; IVF: In Vitro Fertilization
Introduction
The transport function of the mucociliary apparatus of the fallopian tubes (MCA FT) is the most important mechanism for protecting them from endogenous and exogenous pathogenic effects, ensuring the normal state of the reproductive system and the course of the pregnancy process. Its violation under the influence of these effects plays a significant, and sometimes key, role in the pathogenesis of inflammatory diseases of the reproductive organs, which are the leading cause of infertility among a variety of etiological factors, including exposure to tobacco smoke, alcohol and other causes [1]. Nevertheless, this problem is not given enough attention, although it is obvious that its solution can increase the effectiveness of conservative treatment of inflammation and reduce the frequency of surgical interventions, optimize them, which is one of the important tasks of gynecology and reproductive medicine [2]. This determined the purpose of this review - to analyze the state of the problem from a modern perspective and expand our understanding of the function of the MCA FT and the role of its disorders in the development of diseases of the reproductive system and infertility, as well as to determine the prospects for correcting these disorders based on the latest scientific achievements.
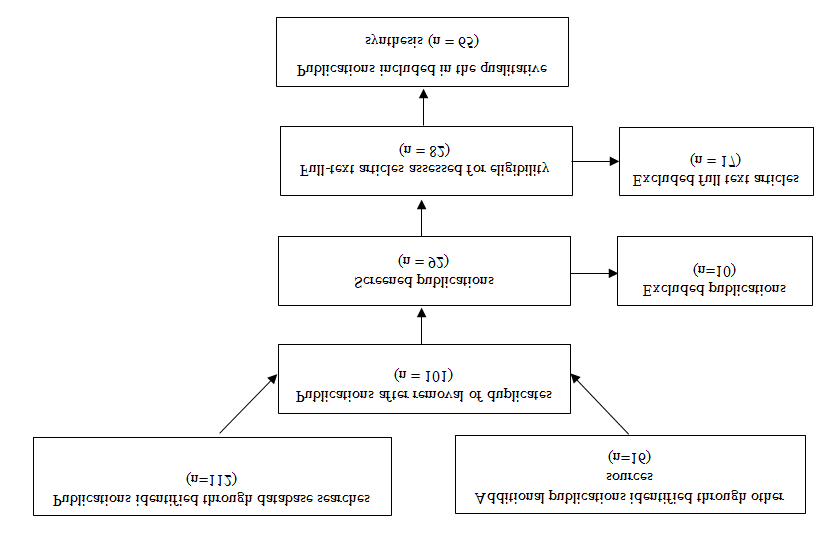
The methodological basis of the study was based on the analysis of the state of the problem by using various literary databases, including Index Medicus, Scopus, PubMed, Embase, Cochrane Library and others, for the period 1990- 2024. The key words and phrases were used: “mucociliary apparatus”, “mucociliary system”, “fallopian tubes”, “cilia and mucus of the fallopian tubes”, “disorders and infertility”. The researcher selected the information independently, and then analyzed only full-text original articles with research results, as well as systematic reviews (Figure 1). The selected literary data were systematized and then used to prepare a review article. Morphofunctional and structural-genetic aspects and features of the mucociliary apparatus of different parts of the reproductive organs.
As the analysis of literary data showed, the function of the reproductive organs, as well as a number of other organs and systems, including the brain, organs of vision, kidneys, and the bronchopulmonary system, is largely determined by mobile cytoplasmic outgrowths of the epithelium, which include axonemal structures and are classified as special- purpose organelles [3].
In the female reproductive system they are represented by cilia, which are formations of ciliated cells that are part of the single-row columnar epithelium of the mucous membrane of the uterus, which is a paired formation and is represented (as in the conducting respiratory tract) by a single-layer columnar epithelium (Figure 2). Cilia constitute a high numerical density (≈ 1 million per 1 cm) and are in constant unidirectional movement towards the uterus. Between the cells of the ciliated epithelium there are secreting (goblet) cells that produce a viscous fluid (mucus) covering the surface of the epithelium and moving in accordance with the movement of its cilia towards the uterus at a speed of up to 70–100 μm/s [4] (Figure 2; A1, A2). The flow of fluid transports the egg and embryo (Figure 2; C5–C10). It has been established that the movement of the cilium, which provides transport.
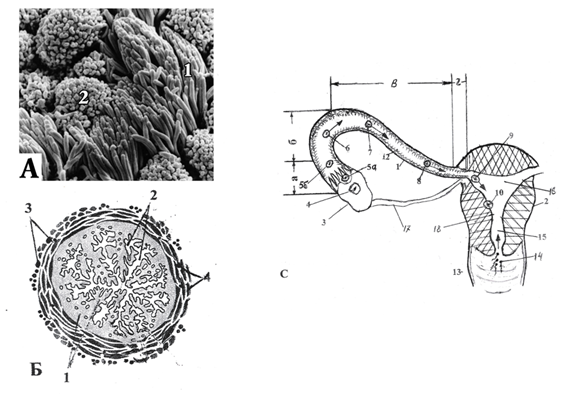
Note: A – fallopian tube mucosa is determined mainly by two types of cells: ciliated (1) and secretory (2); B – cross- sectional image of fallopian tube: 1 – mucous membrane of fallopian tube, 2 – lumen of fallopian tube, 3 – blood vessels, 4 – muscular layer of fallopian tube; C – a depicting functional and structural features of the fallopian tube: 1 – fallopian tube, 2 – uterus, 3 – ovary, 4 – corpus luteum, 5a – immature egg, 5b – mature egg fertilized by sperm, 6 – zygote formation, 7 – zygote resulting in blastomeres, 8 – zygote transformation into blastula, 9 – blastula moving into the uterine cavity, 10 – implantation of the blastula into uterine mucosa, 11 – fallopian tube fimbria, 12 – mucus-covered fallopian tube cilia (mucociliary apparatus), 13 – vagina, 14 – sperm, 15 – cervical canal, 16 – uterine cavity, 17 – ovarian ligament, 18 – uterine mucosa (endometrium), 19 – myometrium. Fallopian tube compartments: a – infudibulum, b – ampulla, c – isthmus, d – pars uterina.
Mucous membrane has its own beating cycle and its trajectory resembles the movement of a swimmer’s arm.
During the beating, making an effective blow towards the uterus, it describes an arc of 180° in the sagittal plane and, with the help of the “claws” at the ends of the cilia, pushes the fluid forward. Then the cilium bends and makes a backward stroke along the trajectory of an arc of 180° in the frontal plane, during which it, taking its original position, rests [5]. The beating of the cilia is highly coordinated, and their beating occurs rhythmically, one after another, with slightly shifted in time cycles of neighboring cilia. In this case, metachronal waves are formed, moving in the direction opposite to the effective blow [6]. The beating frequency of the cilia of the FT varies, according to different authors, from 5 to 12.5 Hz, which is apparently associated with the study being conducted in vivo and in vitro. Regardless of this, the beat frequency increases by 10% in the ampullar region compared to the fimbrial region [7]. The main molecular engine that ensures the functioning of the cilia is axonemal dynein, which is controlled by a number of genes, including DNH5, DNH4, etc [8]. Such a well-coordinated morphofunctional combination of the ciliary and mucous links of the FT is called the MCA or, according to the theory of biological systems, the mucociliary system, as is the case, for example, with the respiratory organs [9]. Due to the work of the MCA, the egg, captured by the fimbria of the FT, moves from the ovary to the uterine cavity, and this path is 10–12 cm (Figure 2; A1, C12). Thus, one of the main functions of the FT is carried out – the transport of the egg and embryo, ensuring normal fertility of a woman.
The process of egg transport due to the MCA, according to some researchers, is more fundamental for the ampullar region of the FT, where fertilization and early stages of embryogenesis occur (Figure 2; C6) [10].
The transport of the ovulating and fertilized egg into the uterine cavity, where it implants and creates conditions for the development of the embryo (Figure 2; C5–C10), is optimized due to the interaction and adhesive contacts between the ciliary receptors and the cumulus cells of the egg [11, 12]. The secretion of the FT epithelium is located along the apical surface of the secretory and ciliated cells of the endosalpinx epithelium and contains nutrients for the sperm and oocyte, providing a suitable environment for fertilization and sperm capacitation [13, 14]. Its main components are glucose and glycoproteins, as well as bicarbonates - lactic acid, calcium, sodium, and chloride. The content of glucose, pyruvate and lactate, measured by microfluorescence analysis, was 1.11, 0.14 and 4.4 mmol / l, respectively. The study of the composition of human tubal secretion shows that it is rich in amino acids. Measurement of the concentration of 17 amino acids in tubal fluid, carried out using high-performance liquid chromatography, showed the predominance of arginine, alanine and glutamate, which is lower than the concentrations in blood plasma. Violations of the rheological properties of the secretion hinder the work of cilia and the efficiency of the MCA, which creates conditions for the development of an infectious process, reduces the possibility of moving the egg. If fertilization does not occur, the oocyte remains viable for a maximum of about 24 hours. Various causes that reduce the motility of the cilia or make it uncoordinated and, therefore, ineffective, reduce the movement of the egg, and pregnancy does not occur, or a tubal (ectopic) pregnancy develops. The division of cells into ciliated and secretory, unlike the respiratory tract, is not categorical, since the same cells, depending on the hormonal balance of the body, can exhibit signs of both secretory activity and ciliogenesis, although there are obvious morphological differences in the apical surfaces of these cell types. Ciliated cells, as in the respiratory tract, are at different stages of ciliogenesis, which largely depends on the saturation of the body with estrogens and directly depends on their concentration in the blood [15]. For example, a slowdown in the ciliogenesis process is observed in the luteal phase of the cycle, as well as with endometrial atrophy. The mucous membrane of the FT in their transitional sections adjacent to the uterus (Figure 2; B1, Cc, Cd) passes into the mucous membrane of the latter. At the same time, as it approaches the uterus in the isthmic part of the FT, the number of cilia decreases, and the efficiency of transport becomes somewhat lower [16]. At the same time, the number of secretory cells increases towards the uterine end of the FT.
The physical properties of the mucus covering the ciliary epithelium, as in other organs, in particular in the respiratory tract, play an important role in the work of the mucociliary apparatus of the FT. It has been shown that epithelial cells respond to increased viscosity of the culture medium, modulating their development and functionality to improve the formation and coordination of cilia. In particular, the ciliary beat frequency decreases by 30% when cells are cultured at 100 mPa.s. In this case, increased viscosity activates the TRPV4 channel in epithelial cells to increase intracellular Ca 2+, subsequently decreasing the level of mitochondrial membrane potential for ATP production to maintain cell viability and function. This represents a potential mechanism to facilitate egg and embryo transport, suggesting possible therapeutic options for the treatment of infertility [17].
Considering the importance of assessing the transport function of the MCA FT a method for measuring the ciliary beat frequency in real time during laparoscopy or laparotomy was developed based on the already developed simple laser spectroscopy method. In this case, the point of application is the ampullar part of the FT. This allows assessing the motor activity of the MCA FT and performing a correlation between morphological indicators, including the ultrastructure of the cilia and their percentage index, determined in biopsies and functional indicators [7].
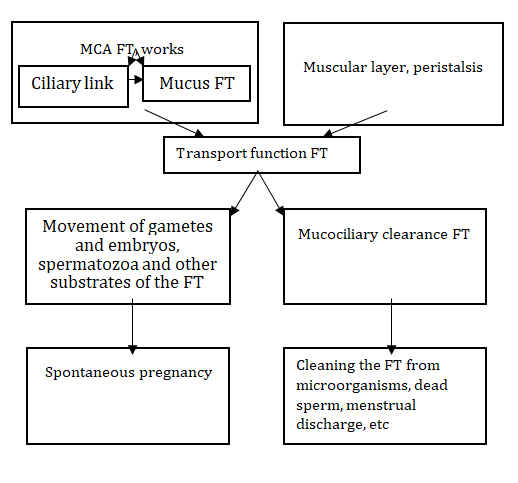
It should be noted that the transport function of the MCF FT, in contrast to, for example, the respiratory tract, where it is normally the only one, is supplemented by another component - peristalsis of the fallopian tubes. The latter is carried out due to the presence of a muscular membrane in the FT and its contractions towards the uterus, as a result of which the embryo is moved into the uterus, especially in the isthmic part of the FT at the morula stage, where the muscular layer is thickest and, as mentioned above, there is a smaller number of ciliated cells [16]. The contractions are most pronounced in the isthmic part of the FT, i.e. where the activity of the MCA decreases due to a decrease in the number of cilia and the frequency of their beating, and it is necessary to ensure the passage of the zygote into the uterus. At the same time, in their ampullar part only pendulum-like movements occur, apparently ensuring the capture of the egg. It has been established that the directions of the wave of FT contractions are associated with the site of application of irritation (egg, sperm) and can be directed from the ampulla to the uterus (properistalsis) and from the uterus to the FT (antiperistalsis). Thus, they facilitate the movement of sperm and ensure the movement of the egg, zygote or embryo into the uterus [18]. With a decrease in estrogen levels, the excitability of the FT is reduced, reactions to irritation are weakened, which can lead to a decrease or absence of perception of the egg and disruption of the mechanism of its transport. With the onset of menopause, the tone and excitability of the muscular membrane are significantly reduced, and contractions in the fimbrial part of the FT are absent [19].
However, the key role in the transport of the egg is given to the MCA. Thanks to a certain approach to the study of the functional patency of the FT, providing a differentiated assessment of the contribution of the ciliary and muscular links, the leading role of the MCA was established, and this role significantly prevails over the contribution of the muscular component [20]. In addition to the transport function, which ensures reproductive processes, the MCA FT performs the function of their clearance. In this case, the cleansing of the fallopian tubes by the FT occurs from possible contents: secretion, microorganisms that have entered it, dead spermatozoa and menstrual discharge, which largely corresponds to the function of the mucociliary system of the respiratory tract, which is also based on the work of the MCA [4, 8, 21]. The probability of this process is significantly reduced by the disruption of the motor activity of the cilia and/or the death of ciliated cells, as well as the loss of cilia or disruption of the efficiency of their movement and discoordination of beating under the influence of various causes and, obviously, primarily under the influence of an infectious factor [3, 4]. All this, ultimately, has its resulting clinical equivalent - the development of infertility. In this case, there is not so much anatomical as functional obstruction, when tubal infertility can occur with the patency of the FT for a contrast agent during hysterosalpingography or a dye during laparoscopy, and the diagnosis of tubal infertility is clinically excluded. In this case, there is functional obstruction, when a delay or disruption in the movement of the egg along the FT will lead to termination of pregnancy even before the implantation of the embryo to the uterine wall.
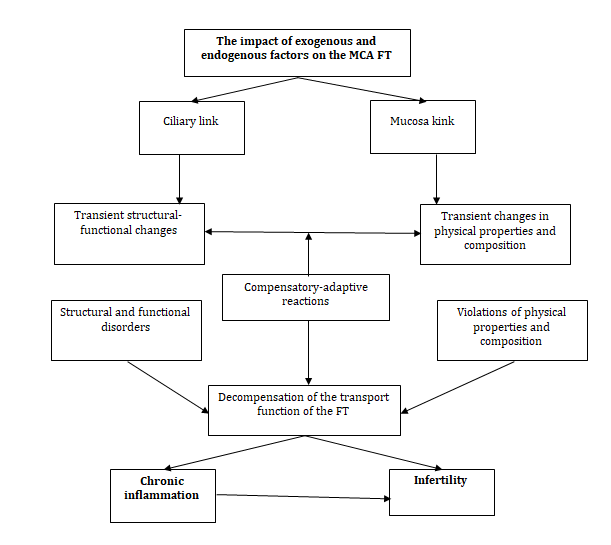
Thus, it seems that a decrease in the evacuation of mucous contents from the FT under the influence of a pathogenic factor can contribute to the development of inflammation in them or maintain the existing one, which entails or aggravates disorders of the FT transport function, leading to its decompensation, chronic inflammation and infertility, thus causing a “vicious circle” (Figure 4).
Impact of Diverse Factors on the MCA in the Reproductive System
Endogenous Factors: The structural and functional state of the mucous membrane of the FT is significantly influenced by neurohumoral regulation and is subject to cyclic changes under the influence of the physiological dynamics of the hormonal status of a woman [22]. In the follicular phase of the menstrual cycle, there is intensive ciliogenesis and more ciliated cells are formed, while in the luteal phase - secretory cells [16]. In this case, the height of the cells of the mucous membrane of the FT and the number of ciliated cells increase significantly shortly before ovulation and especially at the time of its [23, 24]. In post menopause, there is a decrease in the proliferative and functional activity of the ciliated epithelium to the initial level. The formation and growth of ciliated cells are promoted by estrogens, which stimulate the differentiation of cells from secretory to ciliated. In their absence, ciliated cells become secretory. In a relatively low concentration (10 μmol/l) they do not affect the ciliary beat frequency, while reducing the suppressive effect of progesterone, which suppresses the ciliary beat rate by 40– 50% in such a concentration, and at a concentration of 2 ng/l 50–70% of cilia are paralyzed [25].
Data were obtained indicating the presence of receptors for angiotensin II on the epithelial cells of FT and its stimulating effect on the ciliary activity of FT. Evidence of this was the possibility of blocking these receptors with a specific antigen - losartan, which is used as an antihypertensive agent and is an angiotensin II receptor blocker, and also has high selectivity and affinity for receptors [26].
Under the influence of hormonal shifts, there may be dynamics not only of the state of the ciliary apparatus, but also of the mucous link of the MCA FT. In the second phase of the menstrual cycle, the secretory cells acquire a goblet shape and protrude above the ciliated cells due to a simultaneous decrease in the height of the ciliated cells. Their activity becomes maximal, and the secretion produced by them accumulates in small quantities in the lumen of the FT. It contains glycoproteins, prostaglandins F2α and other biologically active substances that increase the ability of spermatozoa to fertilize and ensure the transport and development of the fertilized egg in the FT [27]. In this phase, the activity of acid phosphatase increases, the content of glycogen and the amount of RNA decrease.
The state of the muscular membrane of the FT, which ensures the transport of the egg to the uterus, also experiences a similar neurohumoral influence. The excitability and contractions of this membrane, as well as the mucous membrane, change depending on the phase of the menstrual cycle. Thus, in the proliferative phase, the excitability and tone of the FT wall increase sharply, which leads to changes in their shape and position relative to the ovary, bringing the FT ampulla closer to it and thereby ensuring the perception of the egg. In the secretory phase, the tone and excitability of the FT wall decrease, its contractions acquire a peristaltic character, ensuring the movement of the egg [18, 28].
Endogenous factors can also include defects in the genes that control the motor protein dynein, due to which the work of the MCA and the transport function of the FT are carried out. However, we will dwell on them separately below.
Exogenous Factors Mechanical and Pharmacological Impacts: Mechanical impacts on the FT can have a damaging effect on the epithelial cover. Thus, using light and electron microscopy, it was found that the use of intratubal contraceptives contributes to a 2-fold decrease in the percentage of ciliated cells [28]. This, according to researchers of this effect, can contribute to a decrease in the transport of sperm and egg, which, accordingly, predisposes to tubal pregnancy and an abnormal embryon [26]. Medicinal contraceptives can also have a negative effect on the MCA FT due to their hormonal effect [29, 30]. Thus, it has been convincingly shown that progesterone and its derivatives, in particular levonorgestrel, can significantly reduce the frequency of FT ciliary beating [31]. Thus, the pathological role of this group of drugs in the transport of the egg and zygote along the FT is manifested [32]. Data on the effect of combined contraceptive drugs on the mucociliary system links have not been identified. Other medications that affect progesterone levels may also have an effect on the MCA [25]. The introduction of human chorionic gonadotropin contributed to an increase in the number of secreting cells and an intensification of secretion in the ampullar and isthmic sections of the FT, which correlated well with an increase in the rate of gamete transport. Antihypertensive drugs such as losartan can also reduce the function of the MCA by blocking angiotensin II receptors [26]. We would like to separately emphasize the extremely negative effect of tobacco smoking on the MCA of the reproductive organs, given that this pathogenic factor is one of the leading ones in pulmonary pathology and plays a huge role in the development of diseases of multifactorial and monogenic nature. It was shown that all tested components of tobacco smoke, including nicotine, formaldehyde, phenol and a number of others, reduced the ciliary beat frequency by 30-50 times, and infertility, FT obstruction and ectopic pregnancy were more common in smoking women [33, 34]. At the same time, a significant decrease in the motor activity of the cilia, adhesive contacts between the cilia receptors and the cumulus cells of the egg and the movement of oocytes by them under the influence of chemicals in cigarette smoke was established [11]. It should be emphasized, and this is repeatedly pointed out by researchers studying the problem of MCA FT, that normal FT patency does not always correspond to the situation when women, under the influence of the above-mentioned reasons, may experience various types of ciliary apparatus disorders (pattern of its motor activity, anthropometric nature, etc.), leading to termination of pregnancy and infertility, as well as to ectopic pregnancy. This is evidenced by studies of the ciliary apparatus in women with infertility, indicating the negative role of ciliary dyskinesia [18, 22, 35, 36].
Infectious Agents and Inflammatory Products
Most often, significant influence on the function of the ciliary apparatus is exerted directly by infectious agents and inflammatory products occurring in gynecological diseases. In a significant part of them, pathology of the FT is found together with infertility [37]. The infection, which plays a leading role in this, is usually transmitted sexually, spreading to the upper parts of the female genital tract, gets into the FT, and leads to their functional damage and infertility [38]. In more than 1/5 of patients suffering from salpingitis, the etiologic factor is chlamydia. The prevalence of chlamydial infection is 4.7% in women aged 14-24 years, which suggests the advisability of annual screening in women of this age [39, 40]. A feature of this infection is the ability to persist in the cells of the ciliated epithelium, forming inclusions that allow it to avoid the mechanism of phagocytosis, destroy cells, releasing chlamydial bodies and starting another development cycle after 48-72 hours [41]. In this case, the frequency of ciliary activity in the presence of this infection decreases several times [42]. The host response, including the formation of proinflammatory cytokines and other biologically active substances, is another important pathogenetic link that promotes the formation of scars and fibrosis. They, in turn, lead to occlusion of the FT and infertility [43]. A significant role in the development of salpingitis also belongs to gonococci and mycoplasmas. However, mixed infections often occur. The most pronounced damage to the epithelium of the FT is observed with Neisseria gonorrhea, when the motor activity of the cilia decreases several times [44]. Less damage to the ciliary epithelium occurred when evaluating Chlamydia trachomatis and Mycoplasma genitalium, but not Mycoplasma hominies [45]. A significant role in the inflammatory process of the pelvic tract is played by infection after childbirth, miscarriage, termination of pregnancy or installation of mechanical endometrial contraceptives, postoperative pelvic infection (e.g. perforated appendix, ovarian cyst), and endometriosis. Significant damage to the pelvic tract mucosa is also observed in tuberculosis and viral infections [46]. Pelvic tuberculosis is a common cause of tubal infertility, especially in developing countries. Tuberculosis bacteria enter the pelvic tract from the lungs through the bloodstream, causing significant damage to their mucous membrane [47, 48]. Chronic inflammation in the pelvic tract mucosa usually leads to atrophic changes in the epithelium. The latter, accompanied by a decrease in the height and number of ciliated cells, their replacement with cuboidal epithelium and the appearance of areas devoid of cilia, and the development of sclerosis, in turn disrupt the function of the pelvic tract and lead to infertility. Of particular interest are the results of in vitro evaluation of ciliary activity using laser spectroscopy, indicating a decrease in the oscillation frequency in the case of infertility [49]. Morphological examination of the ciliary apparatus of the respiratory tract and FT often shows a similar picture, but it has not yet been decided what level of gradation of the motor activity of FT cilia can serve as a diagnostic criterion, although searches in this direction seem quite promising to us.
There is evidence that under the influence of any infectious agent, in particular Chlamydia trachomatis, and the production of cytokines, abnormal expression of the CFTR protein (cystic fibrosis transmembrane conductance regulation) can occur [50, 51]. This, in turn, can disrupt the epithelial sodium channel and electrolyte balance in FT and, by increasing their content, increase the fluid level due to an increase in its passive transport into the lumen of the FT. The presence of hydrosalpinx fluid that enters the uterus contributes to the disruption of the transport of the ovum of the CFTR and the disruption of embryo implantation, or the receptivity of the endometrium of the transferred embryos during in vitro fertilization (IVF), reducing its effectiveness [52]. Ultimately, this leads to infertility. Taking into account these pathogenetic features associated with the fluid and transport function of the CFTR is important, since, on the one hand, about 30% of infertile women who need assisted reproductive treatment have hydrosalpinx. On the other hand, this will stimulate the improvement of the approach to infertility treatment using CFTR-specific inhibitors in combination with antibiotics as a significant potential addition. This will significantly improve the results of IVF and optimize the strategy and tactics of infertility treatment and may be a more attractive option for most patients than salpingectomy.
Endometriosis
It has been established that endometriosis is a significant factor negatively affecting the MCA FT. Its association with infertility is known. However, the mechanisms underlying this association, as well as the disease itself, remain poorly understood. The effect of peritoneal fluid in women with early endometriosis on the ciliary epithelium beat frequency of the human fallopian tubes was shown. For this purpose, peritoneal fluid from women with early endometriosis and from fertile women without signs of endometriosis for control, as well as fallopian tubes from hysterectomy specimens were used. A comparative assessment of the ciliary beat frequency between the fallopian tubes exposed to peritoneal fluid in women with and without endometriosis showed a significantly lower ciliary beat frequency in women with endometriosis than in the control group, indicating a negative effect of endometriosis on the activity of the MCA FT and fertility [53]. Other studies have demonstrated that impaired fertility in women with endometriosis may be due to impaired sperm binding to the tubal epithelium [54]. A certain clarification of this may be provided by studies of the ciliary beat frequency on FT samples obtained as a result of hysterectomy and salpingectomy in patients with endometriosis and uterine leiomyoma (control group) using the appropriate technique. They showed a significant decrease in the motor activity of cilia (p < 0.001) and a lower percentage of them on the mucosal surface [55]. The pathogenetic role of proinflammatory cytokines in infertility in this disease has been established [55]. In particular, an increase in the level of interleukin-6 (IL-6) contributes to a decrease in the ciliary activity of FT by 24% [56, 57]. Therefore, modern and effective treatment of endometriosis, against which the MCA FT deficiency develops, involves the use of drugs that regulate the level of estrogen and, accordingly, interleukins under its influence [58, 59]. However, these drugs have significant side effects, significantly limiting the possibilities of their use. At the same time, from this position, certain prospects are traced in the use of leukotriene receptor antagonists, which can potentially neutralize the negative effect of leukotrienes on the activity of MCA FT [60]. At the same time, it was shown that with their use, more rapid and significant dynamics of morphological changes and clinical symptoms were noted, which was accompanied by the onset of pregnancy in some of the women. This indicates a high potential for using drugs of this type.
Primary Ciliary Dyskinesia
The presence of genetically determined pathology associated with its ciliary link may affect the MCA of the FT. Thus, in primary ciliary dyskinesia, there are ultrastructural disorders of the axoneme of the tubules as a result of defects in the genes, including those controlling the motor protein dynein. This leads to dyskinesia of the cilia, which is the result of a disorder in their motor activity, which is accompanied by corresponding changes in the organs in which there is MCA. This may concern the respiratory and reproductive organs, in which the ultrastructural structure of the cilia, genetic defects of dynein (its external handles axoneme, DNAH5, DNAH9, DNAH11, etc.), and their corresponding disorders are identical in nature and manifest themselves accordingly as sinusitis, bronchiectasis and infertility. In this case, there is a possibility of complete or partial inversion of the internal organs (situs viscerum inversus totalis or partialis), which, according to one hypothesis, is the result of the absence of their intrauterine inversion, which occurs under the influence of the motor activity of the ciliary link [61]. The combination of pansinusitis, bronchiectasis and situs inversus, which occurs in approximately 20% of cases of primary ciliary dyskinesia, is also called the Sievert-Kartagener syndrome. This syndrome, which concerns bronchopulmonary pathology, was discovered by the Russian physician of the Kyiv province of the Russian Empire A.N. Sievert in 1902 [62] and described in more detail by the German researcher M.
Kartagener more than 30 years later [63]. The syndrome is often used as a model for isolating and studying the MCA as an object of research, due to more reliable and easier diagnostics due to the presence of situs inversus. At the same time, since the composition of the motor protein dynein and the function of the cilia of the FT in this pathology resemble those of the cilia of the respiratory tract, women with such changes often, but not necessarily, suffer from infertility and can spontaneously become pregnant, along with the fact that some of them had a significant violation of the clearance of the respiratory tract [64].
Perhaps this indicates that the transport of the egg does not completely depend on the work of the MCA, and its insufficiency can be compensated for by other additional mechanisms that can take place in this case in the FT, but are absent in the respiratory tract, in particular, the above- mentioned muscular peristalsis, the composition and properties of the mucus of the FT, etc. However, the role of the latter has not been studied regardless of the motor activity of the cilia. In addition, epidemiological studies are needed to more accurately determine the degree of subfertility in these women [64]. However, where infertility already exists, it is important to confirm it with morphofunctional studies to determine further tactics and strategies for managing this group of patients.
Conclusion
Impairments of the FT transport function may be of various genesis. They contribute to the development of inflammation and infertility and are often the key link in this. At the same time, in a significant part of these functional disorders, the anatomical patency of the FT, assessed by conventional research methods (for example, using hysterosalpingography), can be preserved. Along with the lack of informativeness of invasive research methods in this case, they can even be associated with aggravation of the functional obstruction of the FT due to additional surgical trauma to the MCA FT. Therefore, it would be fundamentally important here to assess the morphofunctional state of the MCA FT using non-invasive, preferably direct, research methods that have not been developed to date. A similar situation applies to the methods of correcting FT patency disorders. There are only general, standard methods of treating various diseases and pathological conditions of the reproductive organs, including inflammatory diseases of infectious genesis. These methods can only indirectly have a corrective effect on the MCA. The main methods of treating FT obstruction remain invasive methods, which contradicts modern trends in medicine. At the same time, given the significant similarity in the structure of MCA FT and respiratory tract and the identity of their morphological structure, it seems appropriate to use studies on MCA of the bronchi for assessing the therapeutic effect on MCA of the reproductive organs, where this problem is presented more informatively and accessibly.
References
-
De Angelis C, Nardone A, Garifalos F, Pivonello C, Sansone A, et al. (2020) Smoke, alcohol and drug addiction and female fertility. Reprod Biol Endocrinol 18(1): 21.
-
Lyons RA, Saridogan E, Djahanbakhch (2006) The reproductive significance of human Fallopian tube cilia. Hum Reprod Update 12(4): 363-372.
-
Marra AN, Li Y, Wingert RA (2016) Antennas of organ morphogenesis: the roles of cilia in vertebrate kidney development. Genesis 54(9): 457-469.
-
Van der Linden PJ (1996) Theories on the pathogenesis of endometriosis. Hum Reprod 11(S3): 53-65.
-
Sleigh MA, Blake JR, Liron N (1988) The propulsion of mucus cilia. Am Rev Respir Dis 137(3): 726-741.
-
Sanderson MJ, Sleigh MA (1981) Ciliary activity of cultured rabbit tracheal epithelium: beat pattern and metachrony. J Cell Sci 47: 331-347.
-
Paltieli Y, Weichselbaum A, Hoffman N, Eibschitz I, Kam Z (1995) Physiology: Laser scattering instrument for real time in vivo measurement of ciliary activity in human Fallopian tubes. Hum Reprod 10(7): 1638-1641.
-
Raidt J, Werner C, Menchen T, Dougherty GW, Olbrich H, et al. (2015) Сiliary function and motor protein composition of Human Fallopian Tubes. Hum Reprod 30(12): 2871-2880.
-
Anokhin PK (1998) Selected works. Cybernetics of functional systems. In: Sudakov KV (Eds.), [Izbrannye trudy. Kibernetika funkcional’nyh sistem. Pod red. K.V. Sudakova]. Moscow: Medicina, Russia, pp: 400.
-
Vasques G, Boeckx W, Brosens I (1995) Prospective study of tubal mucosal lesions and fertility in hydrosalpinges. Hum Reprod 10(5): 1075-1078.
-
Tabolt P, Geiske C, Knoll M (1999) Oocyte pickup by the mаmmalian oviduct. Mol Biol Cеll 10(1): 5-8.
-
Di Carlantonio G, Shaoulian R, Knoll M, Magers T, Talbot P (1995) Analysis of ciliary beat frequencies in hamster oviducal explants. J Exp Zool 272(2): 142-152.
-
Leese HJ, Tay JI, Reischl J, Downing SJ (2001) Formation of Fallopian tubal fluid: role of a neglected epithelium. Reproduction 121(3): 339-346.
-
Saint-Dizier M, Schoen J, Chen S, Banliat C, Mermillod P (2020) Composing the early embryonic microenvironment: physiology and regulation of oviductal secretions. Int J Mol Sci 21(1): 223.
-
Paltieli Y, Eibschitz I, Ziskind G, Ohel G, Silbermann M, et al. (2000) High progesterone levels and ciliary dysfunction: a possible cause of ectopic pregnancy. J Assist Reprod Genet 17(2): 103-106.
-
Abe H, Oikawa T (1993) Observations by scanning electron microscopy of oviductal epithelial cells from cows at follicular and luteal phases. Anat Rec 235(3): 399-410.
-
Abdul Halim MS, Dyson JM, Gong MM, O’Bryan MK, Nosrati R (2024) Fallopian tube rheology regulates epithelial cell differentiation and function to enhance cilia formation and coordination. Nat Commun 15(1): 7411.
-
Rozhdestvenskaya AI (1947) Egg transport from the ovary to the uterus (Motor ability of the human fallopian tube). Leningrad: tipografiya im. Lohankova.
-
Schwaiger T (2020) An updated review on hormone replacement therapy for menopausal women. Natural Medicine J 12(2)
-
Halbert SA, Becer DR, Szal SE (1989) Ovum transport in the rat oviductal ampulla in the absence of muscle contractility. Biol Reprod 40(6): 1131-1136.
-
Becker-Heck A, Loges NT, Omran H (2012) Dynein dysfunction as a cause of primary ciliary dyskinesia and other ciliopathies. In: King SM, (Eds.), Dyneins Structure, Biology and Disease. (Edn.), Academic Press: Elsevier, pp: 602-627.
-
Shirley B, Reeder RL (1996) Cyclic changes in the ampulla of the rat oviduct. J Exp Zool 276(2): 164-173.
-
Frappart L, Berger G, Bethouart M, Palayer C, Bremond A, et al. (1980) The tubal epithelium. Scanning electron microscopy during the menstrual cycle, pregnancy and menopause. J Gynecol Obstet Biol Reprod (Paris) 9(3): 307-313.
-
Hagiwara H, Shibasaki S, Ohwada N (1992) Ciliogenesis in the human oviduct epithelium during the normal menstrual cycle. J Electron Microsc (Tokyo) 41(5): 321- 329.
-
Mahmood T, Saridogan E, Smutna S, Habib AM, Djahanbakhch O, et al. (1998) The effect of ovarian steroids on epithelial ciliary beat frequency in the human Fallopian tube. Hum Reprod 13(11): 2991-2994.
-
Saridogan E, Djahanbakhch O, Puddefoot JR, Demetroulis C, Collingwood K, et al. (1996) Angiotensin II receptors and angiotensin II stimulation of ciliary activity in human fallopian tube. J Clin Endocrinol Metab 81(7): 2719-2725.
-
Rizos D, Maillo V, Lonergan P (2016) Role of the oviduct and oviduct-derived products in ruminant embryo development. Anim Reprod 13(3): 160-167.
-
Eddy CA, Pauerstein CJ (1980) Anatomy and physiology of the fallopian tube. Clin Obstet Gynecol 23(4): 1177- 1193.
-
Wollen AL, Flood PR, Sandvei R, Steier JA (1984) Morphological changes in tubal mucosa associated with the use of intrauterine contraceptive devices. Br J Obstet Gynaecol 91(11): 1123-1128.
-
Brosens IA, Vasgues G (1976) Fimbrial microbiopsy. J Reprod Med 16(4): 171-178.
-
Zhao W, Yan M, Li Ch, Yuan J, Qin G, et al. (2015) Levonorgestrel decreases cilia beat frequency of human fallopian tubes and rat oviducts without changing morphological structure. Clin Exp Pharmacol Physiol 42(2): 171-178.
-
Li C, Zhang H, Liang Y, Xia W, Zhu Q, et al. (2018) Effects of Levonorgestrel and progesterone on Oviductal physiology in mammals. Reprod Biol Endocrinol 16(1): 59.
-
Talbot P, Lin S (2011) The effect of cigarette smoke on fertilization and pre-implantation development: assessment using animal models, clinical data, and stem cells. Biol Res 44(2): 189-194.
-
Knoll M, Talbot P (1998) Cigarette smoke inhibits oocyte cumulus complex pick-up by the oviduct in vitro independent of ciliary beat frequency. Reprod Toxicol 12(1): 57-68.
-
Leng Z, Moore DE, Mueller BA, Critchlow CW, Patton DL, et al. (1998) Characterization of ciliary activity in distal Fallopian tube biopsies of women with obstructive tubal infertility. Hum Repro 13(11): 3121-3127.
-
Guerri G, Maniscalchi T, Barati S, Dhuli K, Busetto GM, et al. (2019) Syndromic infertility. Acta Biomed 90(10-S): 75-82.
-
Healy DL, Trounson AO, Andersen AN (1994) Female infertility: course and treatment Lancet 343(8912): 1539-1544.
-
Hafner LM (2015) Pathogenesis of fallopian tube damage caused by Chlamydia trachomatis infections. Contraception 92(2): 108-115.
-
Torrone E, Papp J, Weinstock H (2014) Prevalence of Chlamydia trachomatis genital infection among persons aged 14–39 years – United States, 2007- 2012. MMWR Morb Mortal Wkly Rep 63(38): 834-838.
-
Geisler WM (2015) Diagnosis and management of uncomplicated Chlamydia trachomatis infections in adolescents and adults: summary of evidence reviewed for the 2015 Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines. Clin Infect Dis (Suppl 8): S774-S784.
-
Wyrick PB (2000) Intracellular survival by Chlamydia. Cell Microbiol 2(4): 275-282.
-
Patton DL, Moore DE, Spadoni LR, Soules MR, Halbert SA, et al. (1989) A comparison of the fallopian tube’s response to overt and silent salpingitis. Obstet Gynecol 73(4): 622-630.
-
Schuchardt L, Rupp J (2018) Chlamydia trachomatis as the cause of infectious infertility: acute, repetitive or persistent long-term infection?. Curr Top Microbiol Immunol 412: 159-180.
-
Lenz JD, Dillard JP (2018) Pathogenesis of Neisseria gonorrhoeae and the host defense in ascending infections of human Fallopian tube. Front Immunol 9: 2710.
-
Baczynska A, Funch P, Fedder J, Knudsen HJ, Birkelund S, et al. (2007) Morphology of human Fallopian tubes after infection With Mycoplasma genitalium and Mycoplasma hominis – in vitro organ culture study. Hum Reprod 22(4): 968-979.
-
Biolatti B, Pau S, Galloni M (1989) The epithelial pathology of bovine genital tuberculosis. J Comp Pathol 100(2): 137-144.
-
Ahmadi F, Zafarani F, Shahrzad G (2014) Hysterosalpingographic appearances of female genital tracttuberculosis: Part I. Fallopian tube. Int J Fertil Steril 7(4): 245-252.
-
Chowdhury NN (1996) Overview of tuberculosis of the female genital tract. J Indian Med Assoc 94(9): 345-356.
-
Kurilo LF, Lyubashevskaya IA, Dubinskaya VP, Gaeva GN (1993) Karyological analysis of the count of immature germ cells of the ejaculate. Urologiya i nefrologiya (2): 45-47.
-
Ajonuma LC, Ng EH, Chow PH, Hung CY, Tsang LL, et al. (2005) Increased cystic fibrosis transmembrane conductance regulator (CFTR) expression in the human hydrosalpinx. Hum Reprod 20(5): 1228-1234.
-
He Q, Tsang LL, Ajonuma LC, Chan HC (2010) Abnormally up-regulated cystic fibrosis transmembrane conductance regulator expression and uterine fluid accumulation contribute to Chlamydia trachomatis-induced female infertility. Fertil Steril 93(8): 2608-2614.
-
Mansour RT, Aboulghar MA, Serour GI, Riad R (1991) Fluid accumulation of the uterine cavity before embryo transfer: a possible hindrance for implantation. J Vitro Fert Embryo Transfer 8: 157-159.
-
Lyons RA, Djahanbakhch O, Saridogan E, Naftalin AA, Mahmood T, et al. (2002) Peritoneal fluid, endometriosis, and ciliary beat frequency in the human fallopian tube. Lancet 360(9341): 1221-1222.
-
Reeve L, Lashen H, Pacey A (2005) Endometriosis affects spermendosalpingeal interactions. Hum Reprod 20(2): 448-451.
-
Xia W, Zhang D, Ouyang J, Liang Y, Zhang H, et al. (2018) Effects of pelvic endometriosis and adenomyosis on ciliary beat frequency and muscular contractions in the human fallopian tube. Reprod Biol Endocrinol 16(1): 48.
-
Papathanasiou А, Djahanbakhch O, Saridogan E, Lyons RA (2008) The effect of interleukin-6 on ciliary beat frequency in the human fallopian tube. Fertil Steril 90(2): 391-394.
-
Lyons RA, Djahanbakhch O, Mahmood T, Saridogan E, Sattar S, et al. (2002) Fallopian tube ciliary beat frequency in relation to the stage of menstrual cycle and anatomical site. Hum Reprod 17(3): 584-588.
-
Polyanskikh LS, Petrosyan MA, Morozkina SN, Baziyan EV (2019) Current understanding of selective estrogen receptor modulators. Journal of Obstetrics and Women’s Diseases 68(6): 99-106.
-
Barra F, Romano A, Grandi G, Facchinetti F, Ferrero S (2019) Future directions in endometriosis treatment: discovery and development of novel inhibitors of estrogen biosynthesis. Expert Opin Investig Drugs.; 28(6): 501-504.
-
Sugamata M, Ihara T, Uchiide I (2015) A new therapy for human endometriosis: the therapeutic value of leukotriene receptor antagonist for endometriosis. Open J Obstet Gynecol 5(6): 313-318.
-
Afzelius BA (2000) Ciliary structure in health and disease. Аcta Otorhinolaryngol Belg 54(3): 287-291.
-
Zivert AN (1902) A case of congenital bronchiectasis in a patient with situs inversus. Russkij vrach 1(38): 1361- 1362.
-
Kartagener M (1933) On the hatogenesis of bronchiectasis. I. Met division: bronchiectasis in situs viscerum inversus. Contributor Klein Tuberk 83: 498- 501.
-
Raid J, Werner C, Menchen T, Dougherty GW, Olbrich H, et al. (2015) Ciliary function and motor protein composition of human fallopian tubes. Hum Reprod 30(12): 2871-280.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’