"Role of Hysteroscopy in Cases of Perimenopausal Abnormal Uterine Bleeding and its Correlation with Histopathology"
Introduction: Abnormal uterine bleeding (AUB) is a common clinical issue among perimenopausal women aged 40-49 years, often requiring multifaceted diagnostic approaches. This study aimed to evaluate the role of hysteroscopy in diagnosing causes of AUB in this demographic profile and correlate its finding with histopathological results to enhance diagnostic accuracy and treatment outcomes. Material & Methods: This prospective observational study included 60 perimenopausal women aged 40-49 years presenting with AUB at the Department of Obstetrics and Gynaecology, Shri Ram Murti Smarak Institute of Medical Sciences, between August 2022 and January 2024. Participants underwent a comprehensive clinical assessment, including blood tests, transvaginal sonography, and diagnostic hysteroscopy followed by endometrial sampling. The findings were correlated with histopathological reports, and statistical analysis was performed using SPSS version 23 to determine significance and correlations. Results: The largest age group was 48-49 years (23%). Socioeconomic status was evenly distributed across lower middle, upper lower, and lower classes each (25%), with upper primary education being the most common educational status (33%). Frequent and heavy bleeding was the predominant symptom 37%, with 50% of participants experiencing symptoms for less than 12 months. For diagnosing endometrial polyp histopathology being the gold standard demonstrated the highest sensitivity and specificity of 98% and 100% respectively, followed by hysteroscopy with 90% sensitivity at 95% specificity and TVS with sensitivity of 85% at specificity of 90% respectively. For diagnosing secretory endometrium, submucous leiomyoma, endometrial carcinoma histopathology remains the gold standard with highest sensitivity and specificity followed by hysteroscopy and TVS. Conclusion: The study found that TVS, hysteroscopy and histopathology are effective diagnostic tools for AUB in perimenopausal women, with histopathology being the gold standard. Combining these methods enhances diagnostic accuracy and confirms better treatment planning, underscoring the importance of a comprehensive approach in managing AUB.
Abbreviations
AUB: Abnormal Uterine Bleeding; HMB: Heavy Menstrual Bleeding; TVS: Transvaginal Sonography; SIS: Saline Infusion Sono Hysterography.
Introduction
Abnormal uterine bleeding (AUB) is a prevalent clinical issue that gynaecologists frequently encounter, especially among perimenopausal women aged 40-49 years. It has been reported that up to 33% of women attending gynaecological outpatient clinics present with AUB, with this proportion increases significantly in peri- and postmenopausal women [1]. AUB should be characterized based on four specific symptomatic components: cycle frequency, duration, volume, and regularity [2]. Acute AUB refers to excessive bleeding that requires immediate medical attention to prevent further blood loss, while chronic AUB is defined as bleeding that persists for most of the past six months [2, 3, 4]. Dysfunctional uterine bleeding (DUB), now more commonly referred to as heavy menstrual bleeding (HMB), is diagnosed after excluding pregnancy, medications, iatrogenic causes, genital tract pathology, and systemic conditions. HMB is defined as excessive menstrual blood loss that interferes with a woman’s physical, emotional, social, and material quality of life, either alone or in combination with other symptoms [5].
The diagnostic approach to AUB is multifaceted, involving a comprehensive medical history, detailed physical examination, blood tests, imaging techniques, and histopathological analysis. Transvaginal sonography (TVS) is often the first-line imaging technique due to its non-invasive nature, although it has limitations in detecting intracavitary lesions, where saline infusion Sono hysterography (SIS) may be more effective [6]. Hysteroscopy is considered the gold standard for evaluating AUB, as it allows direct visualization of the uterine cavity, enabling targeted biopsies and immediate treatment of pathologies such as polyps and submucosal fibroids [7]. This ‘see-and-treat’ approach enhances diagnostic accuracy and treatment planning, potentially replacing blind diagnostic curettage.
Office hysteroscopy has emerged as a valuable technique for diagnosing and treating uterine pathologies in an outpatient setting without the need for general anaesthesia or sedation. This procedure, facilitated by the narrow width of modern hysteroscopes, offers several advantages, including reduced costs, patient satisfaction, and the ability for patients to resume normal activities immediately after the procedure [8].
Despite the potential for discomfort during the procedure, the benefits of immediate diagnosis and treatment, reduced waiting times, and cost savings make office hysteroscopy an attractive option for both patients and gynaecologists.
In perimenopausal women, structural causes such as fibroids and polyps are common contributors to AUB, with the highest incidence of endometrial polyps occurring in women aged 40-44 years [9]. The International Federation of Gynaecology and Obstetrics (FIGO) classification system categorizes non-gestational causes of AUB using the PALM- COEIN acronym, which includes structural and non-structural causes [5]. Understanding these causes and their correlation with histopathological findings obtained through dilation and curettage is crucial for effective management. This study aimed to evaluate the role of hysteroscopy in diagnosing AUB in perimenopausal women and to correlate these findings with histopathological results, thereby enhancing diagnostic accuracy and improving treatment outcomes.
Materials and Method
This hospital-based prospective observational study was conducted among perimenopausal women aged 40- 49 years presenting with abnormal uterine bleeding at the Department of Obstetrics and Gynaecology, Shri Ram Murti Smarak Institute of Medical Sciences. The study spanned from August 1, 2022, to January 31, 2024, including 60 women who met the inclusion and exclusion criteria. Participants were selected based on specific criteria, which included various forms of abnormal uterine bleeding such as menorrhagia, metrorrhagia, polymenorrhea, infrequent bleeding, intermenstrual bleeding, and light bleeding. Exclusion criteria involved severe anemia, active pelvic infection, certain surgical and medical complications, cervical carcinoma, and pregnancy-related issues.
Data were collected through patient histories, clinical examinations, and investigative findings. Patients underwent a comprehensive clinical assessment, including a detailed local and systemic examination. Blood investigations included a full blood count, bleeding and clotting time, blood group determination, thyroid profile, and kidney function tests along with transvaginal sonography. Diagnostic hysteroscopy was performed during the proliferative phase of the menstrual cycle in a fully equipped operating theatre, after an informed consent. The procedure involved using a rigid continuous flow hysteroscope (30°) with fiber optic light, distending the uterine cavity with saline solution. Endometrial sampling was performed during hysteroscope withdrawal, and samples were sent for histopathological examination. The findings of hysteroscopy were meticulously correlated with histopathological reports to evaluate diagnostic efficacy. Statistical analysis was performed using SPSS version 23, where data were scrutinized through various statistical tests to determine significance and correlations within the dataset, ensuring a robust analysis of the study findings.
Results
Table 1 & Figure 1: Shows the Age Distribution of Study
Participants
Included 60 perimenopausal women aged 40-49 years with abnormal uterine bleeding. The age distribution revealed that the largest group was 48-49 years (23%).
| Age Group (Years) | Number of Participants | Percentage of Total Participants |
|---|---|---|
| 40-41 | 9 | 15 |
| 42-43 | 12 | 20 |
| 44-45 | 13 | 22 |
| 46-47 | 12 | 20 |
| 48-49 | 14 | 23 |
| Total | 60 | 100 |
| Mean age | 43.5±5 |
Table 1: Shows the Age Distribution of Study Participants.
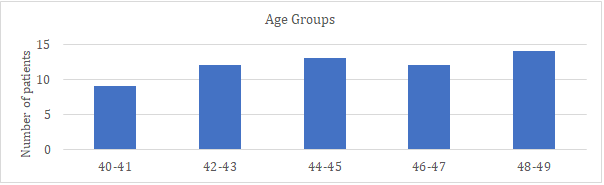
Table 2 & Figure 2 & Figure 3: Depicts the distribution of study participants according to their socioeconomic status
| Socioeconomic Status | Number of Pa- tients (SES) | Percentage (SES) |
|---|---|---|
| Upper class | 5 | 8 |
| Upper middle class | 10 | 17 |
| Low middle class | 15 | 25 |
| Upper lower class | 15 | 25 |
| Lower class | 15 | 25 |
| Total | 60 | 100 |
Table 2: Depicts the Distribution of Study Participants According to their Socioeconomic Status.
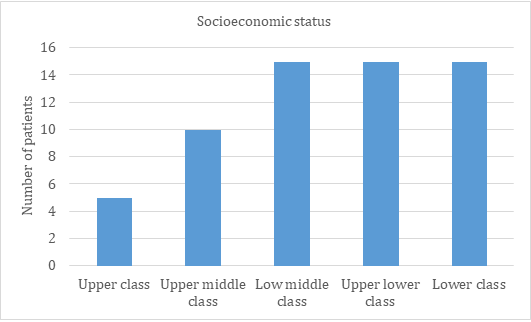
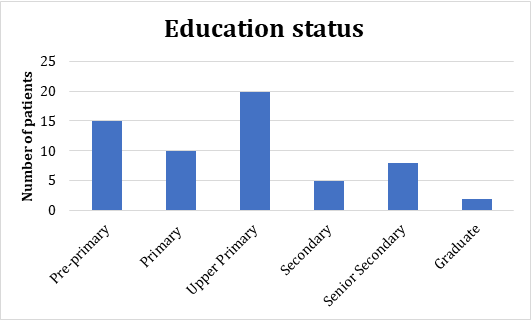
Table 3 & Figure 4 & Figure 5: Shows the Distribution of study participants according to their education level. The educational status was predominantly upper primary (33%), with a significant portion having pre-primary education (25%).
| Education Status | Number of Patients (Edu) | Percentage (Edu) |
|---|---|---|
| Pre-primary | 15 | 25 |
| Primary | 10 | 17 |
| Upper Primary | 20 | 33 |
| Secondary | 5 | 9 |
| Senior Secondary | 8 | 13 |
| Graduate | 2 | 3 |
| Total | 60 | 100 |
Table 3: Shows the Distribution of Study Participants According to their Education Level.
| Menstrual Symptoms | Number of Patients | Percentage (%) |
|---|---|---|
| Frequent and heavy bleeding | 22 | 37 |
| Infrequent and light bleeding | 11 | 18 |
| Intermenstrual Bleeding | 17 | 28 |
| Prolonged bleeding | 10 | 17 |
| Total | 60 | 100 |
Table 4: Assessed Menstrual Symptoms in 60 Perimenopausal Women. The Most Common Symptom was Frequent and Heavy Bleeding (37%), F
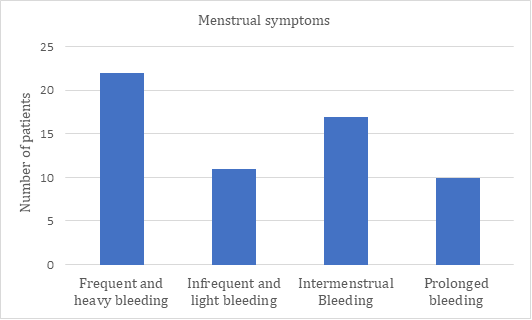
Table 5 and Figure 7- Depicts the distribution of study participants according to their menstrual complaint at time of presentation. Regarding the duration of symptoms, half of the participants reported symptoms lasting less than 12 months, while 33% had symptoms for 12-24 months.
| Duration of Symp- toms | Number of Par- ticipants (Dura- tion) | Percentage (Duration) |
|---|---|---|
| <12 months | 30 | 50 |
| 12-24 months | 20 | 33 |
| >24 months | 10 | 17 |
| Total | 60 | 100 |
Table 5: Depicts the Distribution of Study Participants According to their Menstrual Complaint at Time Of Presentation.
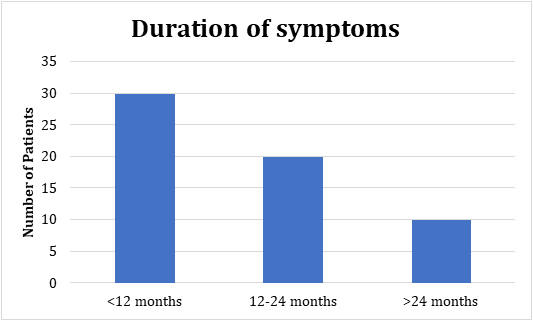
Table 6 and Figure 8, Figure 9: Compared TVS, hysteroscopy and histopathology findings among 60 participants. Endometrial polyps were detected in 30% through histopathology and 32% via hysteroscopy.
Proliferative endometrium was found in 20% through histopathology and 18% via hysteroscopy. Secretory endometrium was identified in 27% by histopathology and 25% by hysteroscopy.
| Finding | TVS | Histopathology Frequency/ percentage | Hysteroscopy Participants |
|---|---|---|---|
| Endometrial Polyps | 16(27) | 18(30) | 19(32) |
| Proliferative Endometrium | 11(18) | 12(20) | 11(18) |
| Secretory Endometrium | 13(22) | 16(27) | 15(25) |
| Chronic Endometritis | 5(8) | 7(12) | 3(5) |
| Endometrial Hyperplasia | 3(5) | 2(3) | 2(3) |
| Submucous Leiomyoma | 7(12) | 3(5) | 6(10) |
| Endometrial cancer | 2(3) | 2(3) | 2(3) |
| Adenomyosis | 2(3) | 0 | 1(2) |
| A-V malformation | 1(2) | 0 | 1(2) |
Table 6: Compared TVS, Hysteroscopy and Histopathology Findings Among 60 Participants. Endometrial Polyps were Detected in 30% th
Table 6: Compared TVS, Hysteroscopy and Histopathology Findings Among 60 Participants. Endometrial Polyps were Detected in 30% through Histopathology and 32% via Hysteroscopy. Proliferative Endometrium was Found In 20% Through Histopathology and 18% via Hysteroscopy. Secretory Endometrium was Identified in 27% by Histopathology and 25% by Hysteroscopy.
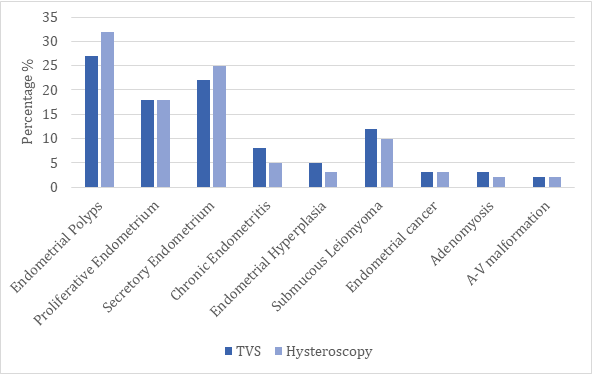
Figure 8: Compared TVS, Hysteroscopy and Histopathology Findings Among 60 Participants. Endometrial Polyps were Detected in 30% Through Histopathology and 32% Via Hysteroscopy. Proliferative Endometrium was Found in 20% Through Histopathology and 18% Via Hysteroscopy. Secretory Endometrium was Identified in 27% by Histopathology and 25% by Hysteroscopy.
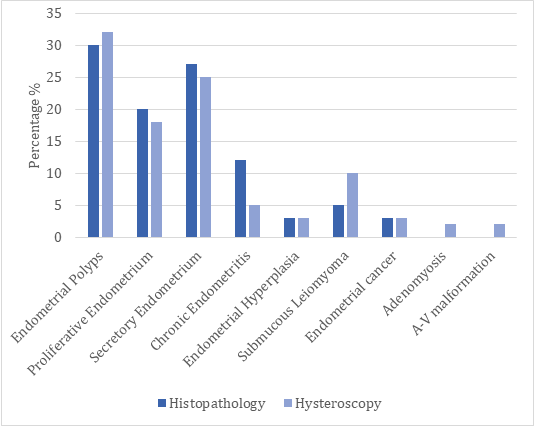
Figure 9: Compared TVS, Hysteroscopy and Histopathology Findings Among 60 Participants. Endometrial Polyps were Detected in 30% Through Histopathology and 32% Via Hysteroscopy. Proliferative Endometrium was Found in 20% Through Histopathology and 18% Via Hysteroscopy. Secretory Endometrium was Identified in 27% by Histopathology and 25% by Hysteroscopy.
| Condition | Test Method | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| Endometrial Polyp | Histopathology | 98% | 100% | 100% | 99% |
| Hysteroscopy | 90% | 95% | 94% | 92% | |
| Transvaginal Sonography (TVS) | 85% | 90% | 88% | 87% | |
| Proliferative Endometrium | Histopathology | 95% | 97% | 96% | 95% |
| Hysteroscopy | 80% | 85% | 83% | 82% | |
| Transvaginal Sonography (TVS) | 70% | 75% | 72% | 73% | |
| Secretory Endometrium | Histopathology and Hysteroscopy | 95% | 95% | 93% | 96% |
| Transvaginal Sonography (TVS) | 80% | 80% | 75% | 85% | |
| Chronic Endometritis | Histopathology | 60% | 85% | 75% | 70% |
| Hysteroscopy | 55% | 80% | 65% | 72% | |
| Transvaginal Sonography (TVS) | 50% | 75% | 60% | 65% | |
| Endometrial Hyperplasia | Histopathology | 90% | 92% | 88% | 93% |
| Hysteroscopy | 85% | 87% | 80% | 91% | |
| Transvaginal Sonography (TVS) | 75% | 80% | 78% | 77% | |
| Submucous Leiomyoma | Histopathology | 95% | 99% | 98% | 96% |
| Hysteroscopy | 90% | 95% | 93% | 92% | |
| Transvaginal Sonography (TVS) | 88% | 93% | 90% | 91% | |
| A-V Malformation | Hysteroscopy | 70% | 85% | 75% | 80% |
| Transvaginal Sonography (TVS) | 65% | 80% | 70% | 75% | |
| Endometrial Malignancy | Histopathology | 99% | 100% | 100% | 99% |
| Hysteroscopy | 90% | 95% | 93% | 92% | |
| Transvaginal Sonography (TVS) | 85% | 90% | 87% | 88% | |
| Adenomyosis | Hysteroscopy | 75% | 80% | 78% | 77% |
| Transvaginal Sonography (TVS) | 80% | 85% | 83% | 82% |
Table 7: Evaluated the Sensitivity and Specificity of Various Test Methods for different Conditions. Histopathology Showed the Hi
Table 7: Evaluated the Sensitivity and Specificity of Various Test Methods for different Conditions. Histopathology Showed the Highest Sensitivity and Specificity for Detecting Endometrial Polyps (98% and 100%, Respectively). Hysteroscopy and Transvaginal Sonography also Provided Valuable Diagnostic Accuracy, Though Slightly Lower than Histopathology.
Discussion
Our study corroborates with study by Mishra A [10] that the age group 48-49 years had the highest prevalence of abnormal uterine bleeding among perimenopausal women. Socioeconomic and educational distributions were similar, though Mishra noted a slightly higher percentage of participants with primary education (30%) compared to the present study’s (17%). A study by Aas-Eng A, et al. [11] focused on the diagnostic evaluation of abnormal uterine bleeding, reporting a higher detection rate of endometrial polyps through histopathology (35%) compared to 30% in the present study. However, the detection rate through hysteroscopy was similar at 34%, compared to 32% found in the current research. This indicates a consistent reliability of both diagnostic methods across different study populations.
On co-relating hysteroscopic findings and histopathological findings for perimenopausal abnormal uterine bleeding a p- value of >0.05 found which is not significant because of small sample size. The sensitivity and specificity of various test methods were evaluated, showing that TVS shows sensitivity and specificity of 85% and 90% respectively, hysteroscopy shows 90% sensitivity at 95% specificity, with respect to histopathology 98% sensitivity at 100% specificity for detecting endometrial polyp indicating that hysteroscopy is the best modality for diagnosing intrauterine pathology and histopathology remains the gold standard to confirm the diagnosis. Aydeniz B, et al. [12] evaluated the laboratory and imaging methods for abnormal uterine bleeding, highlighting a sensitivity and specificity for histopathology at 97% and 98%, respectively, for detecting endometrial polyps. These findings are slightly lower than the present study’s sensitivity of 98% and specificity of 100%. Similarly, Ayde niz reported hysteroscopy’s sensitivity and specificity at 88% and 92%, respectively, which are comparable to the current study’s 90% and 95%. Transvaginal sonography showed a sensitivity and specificity of 80% and 85% in Aydeniz’s study, slightly lower than the present study’s 85% and 90%.
For detecting secretory endometrium TVS showed a sensitivity of 80% and specificity of 80%hysteroscopy showed sensitivity of 95% at specificity of 95% with respect to histopathology shows sensitivity and specificity of 95% each, indicating hysteroscopy and histopathology equally effective for diagnosis. The study by Telner A, et al. [13] on the primary care approach to managing abnormal uterine bleeding found that histopathology and hysteroscopy had similar detection rates for secretory endometrium, at 26% and 24% respectively, closely aligning with the present study’s findings of 27% and 25%. This consistency across studies reinforces the reliability of these diagnostic methods for evaluating abnormal uterine bleeding.
For detecting submucous leiomyoma TVS showing sensitivity 85%and specificity 93% hysteroscopy showed sensitivity of 90% and specificity of 95% with respect to histopathology shows sensitivity 95% and specificity of 99% indicating that hysteroscopy is the best modality for diagnosing intrauterine pathology and histopathology remains the gold standard to confirm the diagnosis.
For detecting endometrial carcinoma TVS shows sensitivity of 85% and specificity of 90% ,hysteroscopy showed sensitivity of 90% and specificity of 95% with respect to histopathology shows sensitivity 99% and specificity of 100% indicating that hysteroscopy is the best modality for diagnosing intrauterine pathology.
Other causes like proliferative endometrium, A-V malformation, adenomyosis, endometrial hyperplasia, chronic endometritis sensitivity and specificity were less than 90%, it was conclusive, indicating that further large randomized case control studies are needed for diagnosis of different causes of AUB by hysteroscopy .Overall, the findings underscore the diagnostic accuracy of combining histopathology and hysteroscopy for evaluating abnormal uterine bleeding in perimenopausal women.
Conclusion
The study of 60 perimenopausal women aged 40-49 years with abnormal uterine bleeding found the most common age group to be 48-49 years (23%), with socioeconomic status evenly distributed across various classes. Frequent and heavy bleeding was the predominant symptom 37%, with 50% of participants experiencing symptoms for less than 12 months. Histopathology and hysteroscopy showed similar detection rates for endometrial polyps 30% and 32% and proliferative endometrium 20% and 18%, with no significant differences .On co-relating hysteroscopic findings and histopathological findings for perimenopausal abnormal uterine bleeding a p- value of >0.05 found which is not significant because of small sample size Histopathology had the highest sensitivity and specificity for endometrial polyps (98% and 100%), followed by hysteroscopy and transvaginal sonography. For detecting secretory endometrium TVS shows sensitivity and specificity of 80% ,hysteroscopy showed sensitivity of 95% at specificity of 95% with respect to histopathology shows sensitivity and specificity of 95% each. For detecting submucous leiomyoma TVS shows sensitivity of 88% and specificity of 93%, hysteroscopy showed sensitivity of 90% and specificity of 95% with respect to histopathology shows sensitivity 95% and specificity of 99%. For detecting endometrial carcinoma TVS shows sensitivity of 85% and specificity of 90% respectively, hysteroscopy showed sensitivity of 90% and specificity of 95% with respect to histopathology shows sensitivity 99% and specificity of 100%. The results highlight the effectiveness of combining histopathology and hysteroscopy for accurate diagnosis in this patient group.
Hysteroscopy is a valuable, simple, low risk technique which allows an adequate visualization of the entire uterine cavity and prompt diagnosis and treatment in the same sitting of specific intrauterine pathologies. It does not substitute other diagnostic procedures, rather it complements them.
For management of AUB patients we can go for screening with noninvasive imaging TVS followed by invasive hysteroscopy according to the pathology detected in TVS and then supported by histopathology. Hysteroscopy should be done prior to subjecting the women with AUB to major operative procedures.
References
-
Mohamed AH, Ismail MT, Abu Shady YA, Mostafa TM (2020) Role of Office Hysteroscopy in Evaluation of Perimenopausal Bleeding Patients Attending Outpatient Gynecologic Clinic. Al-Azhar Medical Journal 49(4): 1753-1764.
-
Munro MG, Critchley HO, Broder MS, Fraser IS (2011) FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet 113(1): 3-13.
-
Munro MG (2024) Abnormal uterine bleeding. Int J Gynaecol Obstet.
-
Whitaker L, Critchley HO (2016) Abnormal uterine bleeding. Best Pract Res Clin ObstetGynaecol 34: 54-65.
-
Chodankar R, Harpur A, Mahmood T (2018) Heavy menstrual bleeding. Obstetrics, Gynaecology & Reproductive Medicine 28(7): 196-202.
-
Chapa HO, Venegas G (2015) Vaginoscopy compared to traditional hysteroscopy for hysteroscopic sterilization. A randomized trial. J Reprod Med 60(1-2): 43-47.
-
Birinyi L, Daragó P, Török P, Csiszár P, Major T, et al. (2004) Predictive value of hysteroscopic examination in intrauterine abnormalities. Eur J Obstet Gynecol Reprod Biol 115(1): 75-79.
-
Dongen HV, De Kroon CD, Jacobi CE, Trimbos JB, Jansen FW (2007) Diagnostic hysteroscopy in abnormal uterine bleeding– A systematic review &meta-analysis. BJOG 114(6): 664-675.
-
Patil SG, Bhute SB, Inamdar SA, Acharya NS, Shrivastava DS (2009) Role of Diagnostic Office Hysteroscopy in Abnormal Uterine Bleeding and its Histopathologic Correlation. J Gynecol Endosc Surg 1(2): 98-104.
-
Mishra A (1988) Clinical symptoms of AUB. JAMA 260(14): 2106-2107.
-
Aas-Eng MK, Langebrekke A, Hudelist G (2017) Diagnostic evaluation AUB 96(12): 1399-1403.
-
Aydeniz B, Gruber IV, Schauf B, Kurek R, Meyer A, et al. (2002) Laboratory evaluation AUB. Eur J Obstet Gynecol Reprod Biol 104(2): 160-164.
-
Telner A, Cravello L, Bretelle F, Shojai R, Roger V, et al. (2002) Primary care approach to the evaluation and management of abnormal uterine bleeding (AUB). 9(3): 264-247.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’