Identification of Environmental Fungal Species in Clinical Services of University Hospital of Angre, Abidjan (Cote d’Ivoire)
Introduction: In hospital’s environment, hygiene of premises and ambient air quality are essential for healthcare. Airborne fungal agents constitute a health concern for patients in these premises. Objective: To identify the fungal agents of the environment in the clinical services of University Hospital of Angre. Materials and Methods: This was a descriptive cross-sectional study was carried out in the clinical services of the University Hospital of Angre from February to May 2024. Samples were taken by swabbing and exposing sterile Petri dishes to the air; then they were plated on Sabouraud-Chloramphenicol medium and incubated in oven at 37° C. Identification of yeast strains was performed using chromogenic medium and the VITEK 2Ò Compact. Molds identification was based on the macroscopic characteristics and microscopic examination of colonies. Results: Among 429 samples, 206 positive cultures (48%) with a higher positivity rate in the surgical emergency service (93.1%). The most isolated fungal agents were molds (84%) with Aspergillus niger at 41.4%. Candida parapsilosis and Candida krusei species were the most prevalent yeasts isolated respectively at 42.3% and 23.1%. The frequency rate of fungal species was correlated to clinical services and sampling sites (p
Introduction
Nosocomial fungal infections or more broadly, fungal infections related to healthcare and the hospital environment, remain dreaded diseases [1, 2]. These diseases are common complication among hospitalized patients especially between who is immunocompromised [3, 4]. Environmental fungal contamination has been associated with health consequences including infectious diseases, toxic effects and allergies. The great diversity of fungal agents constitutes a risk of environmental contamination and the onset of human diseases; they may also come from clinical waste samples [1, 5].
The last decade has seen the emergence of new opportunistic fungal agents, including yeasts and molds. Research has shown that filamentous fungi with translucent mycelia of the Aspergillus genus are the most frequently observed airborne and hospital environmental fungal flora [4, 6]. These fungal agents represent a major concern for intensive care units and a significant challenge for physicians and microbiologists [7].
Furthermore, the emergence of these fungal agents in the environment and their predominance in certain departments such as hospitalization and intensive care, combined with their variable resistance to certain antifungal agents, is one of the causes of therapeutic failure. This makes it difficult to manage patients in these services [7, 8].
In Cote d’Ivoire, as little is known on a national scale, the impact of these fungal agents causing nosocomial infections in immunocompromised patients is estimated by healthcare staff for better management of nosocomial infections in hospital wards [6]. Hygiene in health establishments is defective, and the prevalence of nosocomial infections is alarmingly high. Thus, the prevalence of nosocomial infections is estimated 9% and 12% in the university hospital of Cocody and Yopougon [9]. Therefore, measures must set up to prevent the contraction of nosocomial fungal infections within the various health structures. However, there is no data on environmental fungal contamination of clinical services and consequently no knowledge of the likely fungal species present. This study aimed to determine the biodiversity of environmental fungal flora in clinical services of the University Hospital of Angre.
Material and Methods
Study design and areas
This was a descriptive cross-sectional study carried out over 4 months from February to May 2024 in clinical services at University Hospital of Angre, Abidjan. The services involved in this study were intensive care, neonatology, gynecological consultation and hospitalization, operating room, surgical, gynecological and medical emergencies. The hospital receives patients from all the municipalities of Abidjan and other cities. It boasts high-quality technical facilities, modern health infrastructures and a wide range of services.
Samples collection
Samples were taken from the ambient air, main door, air-conditioner, incubator the nursing staff’s bench, chariot, storage cabinet, etc. A sheet was drawn up for data collection. Samples were collected by swabbing (surfaces) and exposure in Petri dishes containing Sabouraud-Chloramphenicol agar.
Mycological analysis
Surface samples were taken with two sterile swabs: one for direct examination and the other for culture on Sabouraud-chloramphenicol medium poured into tubes. Exposed Petri dishes and inoculated tubes were incubated at 37°C for 3 to 4 days. Fungal agents isolated after culture were identified macroscopically by the appearance of their colonies. Yeast colonies were whitish, smooth, hairless, moist, shiny or matte. In the case of molds, downy, woolly or cottony colonies of varying colors were observed, depending on the species. Yeasts were identified using chromogenic medium method (CHROMagarTM Candida). The Vitek 2 Compact® (Biomerieux) was used according to manufacturer’s procedures in case of yeast diagnosis difficulty.
Molds isolated from culture were identified by their microscopic appearance in lactophenol blue between slide and coverslip at x40 magnification. Thus, for Aspergillus genus, ́identification was based on the identification of conidiophores, of variable length depending on the species, which terminated in aspergillate heads (uniseriate or biseriate heads) consisting of ́a set of vesicles, phialides and conidia.
Statistical analysis
Data analysis was performed using SPSS 21 software (Statical Package for Social Science, IBM SPSS Statistics). All variables were classified in a group and the Fisher exact test was used to compare proportions. P-value < 0.05 was considered significant.
Results
Overall results
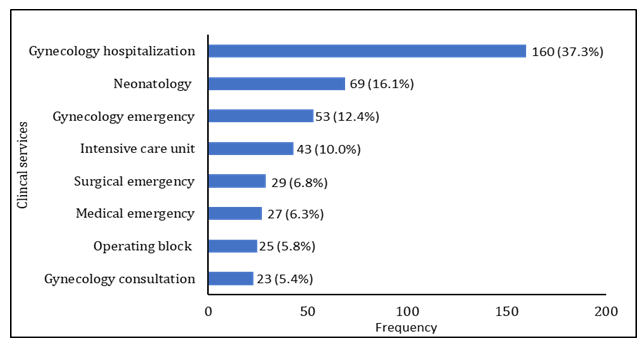
A total of 429 samples were collected from eight clinical services and 12 sampling sites at University Hospital of Angre, Abidjan. Samples were distributed unevenly between the various clinical services. The gynecological hospitalization service has the largest proportion with 37.3%, followed by neonatology with 16.1%. Gynecological emergencies and intensive care have less significant proportions, with 12.3% and 10% respectively. Medical emergencies, surgical emergencies, operating block and gynecological consultations have the lowest frequencies (Figure 1).
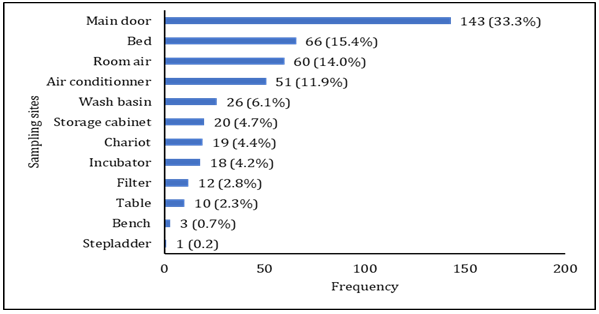
Door handles are the most frequent sampling sites, accounting for 33.3%. Beds followed with 66 samples (15.4%), indicating a high level of potential contamination. Air conditioners and room air show significant proportions of 11.9% and 14% respectively. Sinks and cupboards had proportions of 6.1% and 4.7% respectively. Other sites, such as tables, benches, carts, filters, incubators and slings, represent lower percentages, indicating varying levels (Figure 2).
Mycological results
From 429 collected samples, 206 gave a positive culture with an environmental fungal colonization with a rate of 48%. A statistically significant difference between services and culture results was observed (p=0.0001). Surgical emergency service had the high frequency in positive samples (93.1%) following by medical emergency (85.2%) service and operating block (80%). The lowest positive frequency was observed in intensive care unit at 25.6%. The distribution of positive samples by clinical services is shown in Table 1.
According to positive samples number by sampling site, main door had the highest number of positive samples (63), followed by ambient air (41) and air conditioners (34). But in terms of frequency rate, filter and wash basin were the most contaminated sites with 83.7% and 76.1% respectively. The difference between sampling sites and positive samples is statistically significant (p-value = 0.0001). Table 2 shows the distribution of positive samples by sampling sites.
| Clinical services | Negative culture | Positive culture | |||
|---|---|---|---|---|---|
| Total | Frequency (n) | Percentage (%) | Frequency (n) | Percentage (%) | |
| Gynecology hospitalization | 160 | 93 | 58.1 | 67 | 41.9 |
| Neonatology | 69 | 40 | 58 | 29 | 42 |
| Gynecology emergency | 53 | 37 | 69.8 | 16 | 30.2 |
| Intensive care unit | 43 | 32 | 74.4 | 11 | 25.6 |
| Surgical emergency | 29 | 2 | 6.9 | 27 | 93.1 |
| Medical emergency | 27 | 4 | 14.8 | 23 | 85.2 |
| Operating block | 25 | 5 | 20 | 20 | 80 |
| p-value | 0.0001 |
Table 1: Distribution of negative and positive samples by clinical services.
| Sampling sites | Negative culture | Positive culture | |||
|---|---|---|---|---|---|
| Total | Frequency (n) | Percentage (%) | Frequency (n) | Percentage (%) | |
| Main door | 143 | 81 | 56.7 | 63 | 43.3 |
| Bed | 66 | 46 | 69.7 | 20 | 30.3 |
| Room air | 60 | 19 | 31.7 | 41 | 68.3 |
| Air conditioner | 51 | 17 | 33.3 | 34 | 66.7 |
| Wash basin | 26 | 6 | 23.1 | 20 | 76.1 |
| Storage cabinet | 20 | 15 | 75 | 5 | 25 |
| Chariot | 19 | 15 | 78.9 | 4 | 21.1 |
| Incubator | 18 | 13 | 72.2 | 5 | 27.8 |
| Filter | 12 | 2 | 16.7 | 10 | 83.7 |
| Table | 10 | 7 | 70 | 3 | 30 |
| Bench | 3 | 1 | 33.3 | 2 | 66.7 |
| Stepladder | 1 | 1 | 100 | 0 | 0 |
| p-value | 0.0001 |
Table 2: Distribution of negative and positive samples by sampling sites.
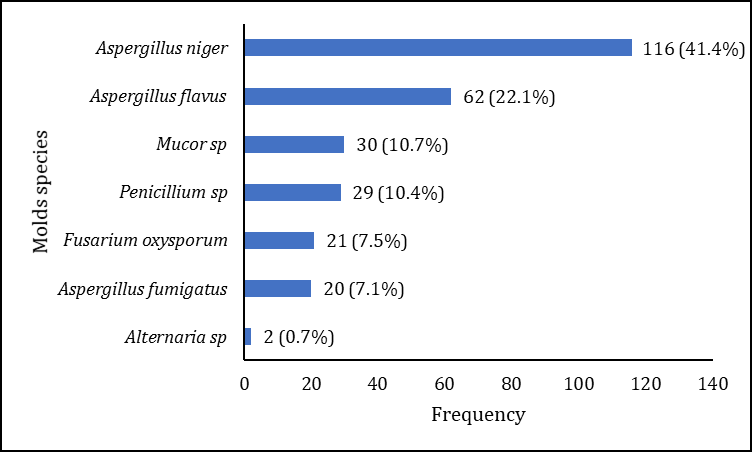
In positive culture, molds were the most frequently identified at 84% following by yeasts (11.2%). Association between molds and yeasts was found at 4.8%. In the molds group, Aspergillus niger is the most frequently isolated species, accounting for 41.4% of cases, followed by Aspergillus flavus with 22.1%. Other Aspergillus species are also present, such as Aspergillus fumigatus (7.1%). In addition to Aspergillus species, other molds were identified, such as Fusarium oxysporum (7.5%), Mucor sp. (10.7%) and Penicillium sp. (10.4%). Alternaria sp. was the least frequent molds with 0.7% of cases (Figure 3).
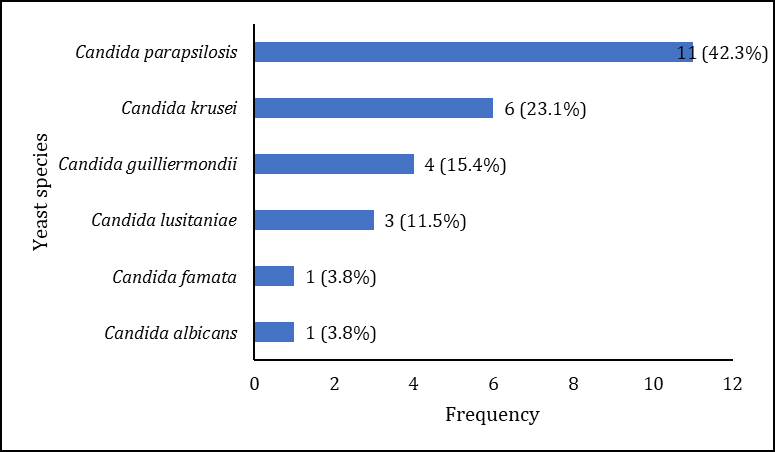
Candida parapsilosis was the most frequently isolated species at 42.3% of cases. Other Candida species were also present, such as C. krusei (23.1%), C. guilliermondii (15.4%), and C. lusitaniae at 11.5%. Candida albicans and Candida famata are the least frequent species, each accounting for 3.8% of cases (Figure 4).
The distribution of isolated mold species by clinical services shows that A. niger and A. flavus were identified from all services with a high frequency in gynecology hospitalization service at 43.1% and 30.6% respectively. Penicillium sp. and Mucor sp. were also observed in this service (Table 3). In the same time, surgical emergency, gynecological hospitalization and medical emergency were the services with the most yeast species, such as C. parapsilosis, C. guilliermondii and C. krusei (Table 4).
| Clinical services | A. niger | A. flavus | A. fumigatus | Alternaria sp | Penicillium sp | Mucor sp | Fusarium oxysporum |
|---|---|---|---|---|---|---|---|
| Operating block | 2 | 8 | 0 | 2 | 8 | 0 | 9 |
| Intensive care unit | 4 | 3 | 1 | 0 | 0 | 1 | 0 |
| Surgical emergency | 10 | 11 | 1 | 0 | 0 | 0 | 10 |
| Medical emergency | 15 | 1 | 4 | 0 | 0 | 0 | 1 |
| Neonatology | 11 | 6 | 3 | 0 | 9 | 0 | 0 |
| Gynecology consultation | 10 | 2 | 0 | 0 | 0 | 1 | 0 |
| Gynecology hospitalization | 50 | 19 | 5 | 0 | 11 | 28 | 1 |
| Gynecology emergency | 14 | 12 | 1 | 0 | 1 | 0 | 0 |
| Total | 116 | 62 | 15 | 2 | 29 | 30 | 21 |
Table 3: Distribution of mold species by clinical services.
A : Aspergillus Table 3: Distribution of mold species by clinical services.
| C. parapsilosis | C. guilliermondii | C. lusitaniae | C. krusei | C. famata | C. albicans | |
|---|---|---|---|---|---|---|
| Operating block | 0 | 0 | 0 | 0 | 0 | 0 |
| Intensive care unit | 1 | 0 | 1 | 2 | 0 | 0 |
| Surgical emergency | 0 | 5 | 0 | 0 | 1 | 0 |
| Medical emergency | 0 | 0 | 0 | 4 | 0 | 1 |
| Neonatology | 2 | 1 | 2 | 0 | 0 | 0 |
| Gynecology consultation | 3 | 1 | 0 | 0 | 0 | 0 |
| Gynecology hospitalization | 4 | 0 | 0 | 0 | 0 | 0 |
| Gynecology emergency | 1 | 0 | 0 | 0 | 0 | 0 |
| Total | 11 | 7 | 3 | 6 | 1 | 1 |
Table 4: Distribution of yeast species by clinical services.
C : Candida Table 4: Distribution of yeast species by clinical services.
We recorded 77 mixed species in our study with a rate of 37.6%. Table 5 shows the fungal species isolated in mixed cultures for all sectors sampled from clinical services. So, for all sampling sites, Aspergillus niger - Aspergillus flavus association predominated at a frequency of 20.8%, followed by Aspergillus niger - Aspergillus flavus - Mucor sp. (11.6%), Aspergillus niger - Mucor sp. (10.4%) and Aspergillus niger- Aspergillus fumigatus (7.8%). Also, association with Fusarium oxysporum - Penicillium sp. and Aspergillus niger- Aspergillus flavus- Fusarium oxysporum were observed at 5.2%°.
| Fungal species | Frequency (n) | Percentage (%) |
|---|---|---|
| Aspergillus niger - Aspergillus flavus | 16 | 20.8 |
| Aspergillus niger-Aspergillus flavus-Mucor sp. | 9 | 11.6 |
| Aspergillus niger - Mucor sp. | 8 | 10.4 |
| Aspergillus niger - Aspergillus fumigatus | 6 | 7.8 |
| Fusarium oxysporum - Penicillium sp. | 4 | 5.2 |
| Aspergillus niger-Aspergillus flavus-Fusarium oxysporum | 4 | 5.2 |
| Aspergillus niger- Candida krusei | 3 | 3.9 |
| Aspergillus niger - Candida guilliermondii | 3 | 3.9 |
| Penicillium sp. -Aspergillus flavus -Mucor sp | 3 | 3.9 |
| Aspergillus niger-Penicillium sp. -Aspergillus flavus | 3 | 3.9 |
| Aspergillus niger- Penicillium sp. | 2 | 2.6 |
| Aspergillus niger - Fusarium oxysporum | 2 | 2.6 |
| Fusarium oxysporum - Aspergillus flavus | 2 | 2.6 |
| Aspergillus niger- Aspergillus flavus -Candida parapsilosis | 2 | 2.6 |
| Aspergillus niger-Mucor sp. - Aspergillus fumigatus | 2 | 2.6 |
| Aspergillus niger- Aspergillus fumigatus- Aspergillus flavus | 2 | 2.6 |
| Penicillium sp. - Aspergillus fumigatus | 1 | 1.3 |
| Aspergillus flavus - Mucor sp. | 1 | 1.3 |
| Penicillium sp. - Mucor sp. | 1 | 1.3 |
| Aspergillus flavus - Aspergillus fumigatus | 1 | 1.3 |
| Penicillium sp. -Aspergillus flavus-Fusarium oxysporum | 1 | 1.3 |
| Aspergillus niger-Aspergillus fumigatus-Fusarium oxysporum | 1 | 1.3 |
Table 5: Distribution of fungal species in mixed culture.
Discussion
This cross-sectional study carried out in eight clinical services at the University Hospital of Angre in Cote d’Ivoire showed unequal distribution of samples between clinical services. The gynecological hospitalization service has the largest sample size. The global frequency rate of environmental fungal colonization was 48%. Higher results than ours were reported in Senegal [4] and Burkina Faso [10]. This high frequency in his study could be explained by a smaller sample size, which was 73 samples. Furthermore, results similar to ours were observed in Cote d’Ivoire at the University Hospital of Bouake, central part of Cote d’Ivoire with a fungal colonization rate of 48.4% [6].
The fungal colonization frequency was highest in the gynecological and neonatology services, and lowest in the intensive care unit. These findings could be explained by the high number of workers in the services which can lead to the surfaces contamination. In contrast, studies carried out in Dakar showed a high frequency in pediatric oncology service and a low positivity rate in neonatology [4]. The difference in frequencies observed may be due to the small sample size in these different studies. We noted a high frequency of colonization at doors and in ambient air. These Similar results were reported in the environment of intensive care units in Bobo-Dioulasso [10]. These results justify to the dissemination of fungal spores in hospital services which penetrate inside buildings. The presence of these fungal agents is a major public health concern, economic and social implications [3, 11].
According to the distribution of the different fungal groups observed, molds were the main ones isolated. Filamentous fungi, such as molds were isolated in tertiary care hospital in previous studies [12, 13]. The predominance of these fungal groups has also been described in the literature [4, 8, 14]. Furthermore, when conditions are favorable, molds produce a large number of mature spores that can be transported by air currents or by humans, and find their way into homes and buildings, including hospitals. The production of spores aerosolized by air can disperse over great distances and to their diversity [10, 15]. In the current study, Aspergillus and Penicillium were the most frequently isolated mold genus. The predominance of the genus Aspergillus was also observed in Cote d’Ivoire [6]. Elsewhere in Brazil, similar studies were conducted in various cities where Penicillium sp. was more identified [16, 17]. Aspergillus and Penicillium genus are ubiquitous, cosmopolitan filamentous fungi that are very abundant in the environment. Aspergillus niger was the most prevalent species. In general, this species is widespread in the outdoor environment as a saprophyte [18, 19]. The spores were associated with positive reactions allergen in human body [20]. In another study, A. niger was among the most prevalent fungal agents in samples from houses of mold-allergic patients and hospital air samples [21]. Aspergillus flavus and A. fumigatus identified in our study were also observed in air in different areas of a hospital [10, 22]. Studies conducted in hospitals have shown that A. flavus can be present in dust inside homes, in ventilation ducts and on contaminated building materials. In a study carried out in Nigeria, A. flavus was identified in wall surface samples taken from damp homes [23]. Aspergillus flavus has also been identified in filters, which can serve as a source of indoor contamination in hospitals [10]. Aspergillus fumigatus identified in our study has been reported elsewhere. The small size of A. fumigatus spores may favor their deposit in the upper respiratory tract [24].
Molds in hospital environment have been observed to exacerbate respiratory presentations with Aspergillus sp., Penicillium sp., and Alternaria sp. found to comprise the predominant allergenic airborne spores [25, 26]. These fungal agents produce numerous small, light spores that remain in the air for a long time, dispersing more rapidly. This can be life-threatening for severely immunocompromised patients [27, 28].
As for the yeast species isolated in the current study, Candida parapsilosis and C. guilliermondii were the predominant species, followed by Candida albicans, C. lusitaniae and C. krusei. Candida parapsilosis is a fungal agent that lives on human body without causing clinical symptoms. If it gets into a wound, surgical incision or implanted medical device, this species could be involved in a serious infection [29]. In addition, the isolation of Candida non-albicans species in our study confirms the emerging nature of these yeasts, which is linked to the increase in the number of immunocompromised patients as a result of the growing number of risk factors (HIV, corticosteroid therapy, chemotherapy, diabetes, etc.). The presence of yeasts in the hospital environment could be associated with care (fibroscopy and oxygen therapy); with the use of medical devices (catheter); with patients and/or nursing staff [30].
Mixed culture in the current study was observed with the association between molds species. These results indicated the potential of hospital services as reservoirs for fungal species [31, 32].
Conclusion
These results highlight the need for measures to prevent the spread of fungal agents in the hospital environment, particularly in clinical wards where patients are at high risk. These measures can include air renewal, disinfection of work surfaces and raising staff awareness of practices such as hand washing and managing mobility between wards. This study is very important for the implementation of rigorous hygiene measures to avoid possible nosocomial infections.
Acknowledgments
The authors would like to express their gratitude to all clinical services of the University Hospital of Angre, as well as those of the Medical Biology service for their availability and support in the successful completion of this work.
References
-
Meheust D, Le Cann P, Reboux G, Millon L, Gangneux JP (2014) Indoor fungal contamination: health risks and measurement methods in hospitals, homes and workplaces. Crit Rev Microbiol 40(3): 248‑260.
-
Mosayebi M, Eslamirad Z, Hajihossein R, Ghorbanzadeh B, Shahverdi M, et al. (2017) Evaluating of fungal contamination in hospital wet cooling systems in Markazi province, Central Iran. J Mycol Med 27(3): 334‑338.
-
Perdelli F, Cristina ML, Sartini M, Spagnolo AM, Dallera M, et al. (2006) Fungal contamination in hospital environments. Infect Control Hosp Epidemiol 27(1): 44‑47.
-
Diongue K, Badiane AS, Seck MC, Ndiaye M, Diallo MA, et al. (2017) Qualitative fungal composition of services at risk of nosocomial infections at Aristide Le Dantec Hospital (Dakar). J Mycol Med 25(1): e39-43.
-
Noman EA, Al-Gheethi EA, Norulaini N, A Talip B, Nagao H, et al. (2017) Identification of Fungi Isolated from Clinical Wastes. Journal of Science and Technology 9(4): 64‑69.
-
Monemo, Adoubryn K. Monemo P, Adoubryn KD (2016) Etude microbiologique environnementale du service de reanimation du CHU Bouake: Resultat d’une enquête preliminaire. Bibliothèque UFR Sciences Medicales Abidjan.
-
Fisher MC, Hawkins NJ, Sanglard D, Gurr SJ (2018) Worldwide emergence of resistance to antifungal drugs challenges human health and food security. Science 360(6390): 739‑742.
-
Caggiano G, Napoli C, Coretti C, Lovero G, Scarafile G, et al. (2014) Mold contamination in a controlled hospital environment: a 3-year surveillance in southern Italy. BMC Infect Dis 14(1): 595.
-
Malick DY, Fulbert T (2022) Hygiene Hospitaliere et Prevention des Infections Nosocomiales en Cote d’Ivore: Cas de l’Hopital General de Dabou. ESJ 18(33): 281.
-
Matotou HRS, Sangare I, Bisseye C, Akotet MKB, Bamba S (2021) Biodiversite de la flore fongique isolee au service de reanimation du Centre Hospitalo-Universitaire Souro Sanou de Bobo-Dioulasso, Burkina Faso. Pan Afr Med Jour 38: 299.
-
Ferreras-Antolín L, Sharland M, Warris A (2019) Management of Invasive Fungal Disease in Neonates and Children. Pediatr Infect Dis Jour 38(6S Suppl 1): S2‑S6.
-
Panagopoulou P, Filioti J, Petrikkos G, Giakouppi P, Anatoliotaki M, et al. (2002) Environmental surveillance of filamentous fungi in three tertiary care hospitals in Greece. J Hosp Infect 52(3): 185‑191.
-
Hao Z feng, Ao J hong, Hao F, Yang RY, Zhu H, Zhang J (2011) Environment surveillance of filamentous fungi in two tertiary care hospitals in China. Chin Med J (Engl) 124(13): 1970‑1975.
-
Lugauskas A, Sveistyte L, Ulevicius V (2003) Concentration and species diversity of airborne fungi near busy streets in Lithuanian urban areas. Ann Agric Environ Med 10(2): 233‑239.
-
Fang Z, Ouyang Z, Hu L, Wang X, Zheng H, et al. (2005) Culturable airborne fungi in outdoor environments in Beijing, China. Sci Total Environ 350(1‑3): 47‑58.
-
Storti LR, Pasquale G, Scomparim R, Galastri AL, Alterthum F, et al. (2012) Candida spp. isolated from inpatients, the environment, and health practitioners in the Pediatric Unit at the Universitary Hospital of the Jundiaí Medical College, State of São Paulo, Brazil. Rev Soc Bras Med Trop 45(2): 225‑231.
-
Gonçalves CL, Mota FV, Ferreira GF, Mendes JF, Pereira EC, et al. (2018) Airborne fungi in an intensive care unit. Braz J Biol 78(2): 265‑270.
-
Gheith S, Ranque S, Bannour W, Ben Youssef Y, Khelif A, et al. (2015) Hospital environment fungal contamination and aspergillosis risk in acute leukaemia patients in Sousse (Tunisia). Mycoses 58(6): 337‑342.
-
Diba K, Jangi F, Makhdoomi K, Moshiri N, Mansouri F (2019) Aspergillus diversity in the environments of nosocomial infection cases at a university hospital. J Med Life 12(2): 128‑132.
-
Segvić Klarić M, Kosalec I, Mastelić J, Piecková E, Pepeljnak S (2007) Antifungal activity of thyme (Thymus vulgaris L.) essential oil and thymol against moulds from damp dwellings. Lett Appl Microbiol 44(1): 36‑42.
-
Price DL, Simmons RB, Crow SA, Ahearn DG (2005) Mold colonization during use of preservative-treated and untreated air filters, including HEPA filters from hospitals and commercial locations over an 8-year period (1996-2003). J Ind Microbiol Biotechnol 32(7): 319‑321.
-
Ortiz G, Yagüe G, Segovia M, Catalán V (2009) A study of air microbe levels in different areas of a hospital. Curr Microbiol 59(1): 53‑58.
-
Odebode A, Adekunle A, Stajich J, Adeonipekun P (2020) Airborne fungi spores distribution in various locations in Lagos, Nigeria. Environ Monit Assess 192(2): 87.
-
Pasqualotto AC (2009) Differences in pathogenicity and clinical syndromes due to Aspergillus fumigatus and Aspergillus flavus. Med Mycol 47(Suppl1): 261-270.
-
Ziaee A, Zia M, Goli M (2018) Identification of saprophytic and allergenic fungi in indoor and outdoor environments. Environ Monit Assess 190(10): 574.
-
Hughes KM, Price D, Torriero AAJ, Symonds MRE, Suphioglu C (2022) Impact of Fungal Spores on Asthma Prevalence and Hospitalization. Int J Mol Sci 23(8): 4313.
-
Vonberg RP, Gastmeier P (2006) Nosocomial aspergillosis in outbreak settings. J Hosp Infect 63(3): 246‑254.
-
Shah K, Deshpande M, Shah P (2024) Healthcare- associated fungal infections and emerging pathogens during the COVID-19 pandemic. Front Fungal Biol 5: 1339911.
-
Govrins M, Lass-Flörl C (2024) Candida parapsilosis complex in the clinical setting. Nat Rev Microbiol 22(1): 46‑59.
-
Simões S de AA, Leite Júnior DP, Hahn RC (2011) Fungal microbiota in air-conditioning installed in both adult and neonatal intensive treatment units and their impact in two university hospitals of the central western region, Mato Grosso, Brazil. Mycopathologia. 172(2): 109‑116.
-
Noman EA, Al-Gheethi AA, Rahman NNNA, Nagao H, Ab Kadir MO (2016) Assessment of relevant fungal species in clinical solid wastes. Environ Sci Pollut Res Int 23(19): 19806‑19824.
-
Chen L, Song Z, Zhou X, Yang G, Yu G (2024) Pathogenic bacteria and fungi in bioaerosols from specialized hospitals in Shandong province, East China. Environmental Pollution 341: 122922.
- Diversity of Candida sp and Antifungal Susceptibility Patterns in Digestive Candidiasis among People Living with HIV in CHU of Libreville, Gabon
- Vulvovaginal candidiasis: Retrospective study (2019- 2021) at the Centre Hospitalier National de Pikine, Suburban Dakar, Senegal
- New Location of some Gasteroid Basidiomycetes in Western Kazakhstan
- Evaluation of Various Extracellular Enzymes of Ectomycorrhizal Mushrooms
- Morphology and Phylogeny of Lactarius Wallichianae sp. nov and Xerula magnispora sp. nov. from India
- Growth of Pleurotus Florida (Oyster Mushroom) on Different Media