Diversity of Candida sp and Antifungal Susceptibility Patterns in Digestive Candidiasis among People Living with HIV in CHU of Libreville, Gabon
Background: Intestinal candidiasis is a common opportunistic condition in people living with HIV (PLHIV). Limited data are available in Africa on prevalence, species diversity, and antifungal susceptibility of intestinal Candida, particularly in asymptomatic or mildly symptomatic patients. This study assessed prevalence, species distribution, and resistance patterns of Candida sp isolated from stools of HIV-infected individuals in Libreville, Gabon. Methods: A descriptive cross-sectional study was conducted from October to November 2021 at the University Hospital of Libreville and the Department of Parasitology, Mycology and Tropical Medicine. Adult PLHIV (≥18 years), without recent antifungal therapy or other predisposing chronic diseases, were enrolled. Stool samples were cultured on chromogenic medium; species were identified by colony colour. Antifungal susceptibility (fluconazole, ketoconazole, clotrimazole, nystatin, miconazole, amphotericin B) was assessed by disc diffusion. Results: Of 107 participants (median age 42 [35–49] years, sex ratio 2.3), median CD4 count was 185 [100–348] cells/mm³. Candida sp was isolated in 68.2% of samples. C. albicans (32.7%) and C. glabrata (31.8%) predominated; C. krusei accounted for 7.5%, while C. tropicalis was absent. Among 61 tested isolates, 19.7% were susceptible to all agents, 24.6% resistant to all, and 50.8% showed multidrug resistance. Resistance was highest to miconazole (75.4%) and fluconazole (70.5%). Conclusion: Intestinal Candida colonisation is frequent in PLHIV in Libreville, with high prevalence of non-albicans species and substantial azole resistance, underscoring the need for enhanced antifungal resistance monitoring and adapted treatment strategies.
Introduction
Digestive candidiasis refers to fungal infections caused by colonisation and invasion of the gastrointestinal tract by yeasts of the genus Candida. These yeasts are usually commensal fungi of the digestive tract but can become opportunistic pathogens in situations of immunosuppression [1, 2, 3, 4]. PLHIV are particularly at risk because of the profound decline in CD4 cell counts, making candidiasis one of the leading aetiologies of opportunistic fungal infections and an AIDS-defining condition [5, 6, 7, 8].
The prevalence of oropharyngeal and/or intestinal candidiasis varies across countries and largely depends on patients’ access to antiretroviral therapy (ART) [6]. Nevertheless, oropharyngeal candidiasis is generally more common in PLHIV compared with intestinal forms. Gastrointestinal T lymphocytes are a primary target of HIV infection, leading to increased permeability of the intestinal mucosa where these cells normally reside [4, 6, 7, 8]. The reduction of gastrointestinal CD4+ T cells has been associated with dysbiosis, which may weaken the antagonistic effect of intestinal microbiota bacteria. Combined with immunosuppression, dysbiosis can promote fungal infections [8, 9]. Interestingly, in some countries such as Cameroon, intestinal candidiasis has been reported to be more prevalent than oropharyngeal candidiasis [10].
Although Candida albicans remains the most frequently isolated species in digestive colonisations, recent studies highlight a shift in this profile, with an increasing proportion of non-albicans Candida species, particularly in cases of prolonged immunosuppression [6, 11, 12, 13]. Frequent antifungal exposure among immunocompromised patients is thought to promote the emergence of non-albicans Candida species, which are often more resistant to azoles [6, 14].
In Gabon, oropharyngeal candidiasis is highly prevalent among PLHIV and often represents one of the first clinical manifestations leading to HIV diagnosis [14]. However, available data on candidiasis in the context of AIDS are outdated (over 10 years old). Furthermore, very limited information is available on intestinal candidiasis in PLHIV, and no data exist regarding the resistance of Candida sp to azole antifungals, despite the widespread use of fluconazole prophylaxis.
This study was therefore designed to determine the prevalence of intestinal colonisation by Candida sp, describe the fungal diversity, and assess the antifungal susceptibility profiles of Candida sp isolated from stool samples of PLHIV in Libreville, Gabon.
Methods
Study Design and Population
This was a descriptive cross-sectional study with prospective data collection conducted from October to November 2021 in the Infectious Diseases Ward of the Centre Hospitalier Universitaire de Libreville (IDW-CHUL) and the Department of Parasitology-Mycology and Tropical Medicine of the Université des Sciences de la Santé (USS). The study was nested within a prevalence survey of opportunistic infections among PLHIV. Participants included in the study, who agreed to provide a stool sample, met the following inclusion criteria: age ≥18 years, no antifungal therapy within the previous three months, provision of oral informed consent, and absence of any other chronic condition known to predispose to candidiasis.
Study Procedures
Participants completed a questionnaire, and additional clinical information was retrieved from their medical records when missing. Collected variables included age, sex, date of HIV diagnosis, use of antiretroviral therapy (ART), CD4 cell count (when available), and WHO clinical stage of HIV infection. After the interview, each participant received a sterile stool container and instructions on proper sample collection to avoid contamination with urine. Samples were returned immediately after collection to the study staff.
Laboratory Diagnosis
Each stool specimen was cultured on a selective and differential chromogenic medium (Chromatic™ Candida, LIOFILCHEM) for species identification. Plates were incubated at 37 °C for 18-24 hours. Only specimens yielding more than 10 colonies were considered positive. Colony colours were interpreted according to the manufacturer’s recommendations: C. albicans (green), C. glabrata (beige), C. krusei (pink with pale edges), C. tropicalis (blue), and C. parapsilosis (pale pink-white) [5, 6, 15]. A 0.5 McFarland inoculum was prepared from a suspension of five colonies in 5 mL of physiological saline. The suspension was streaked on Mueller-Hinton (MH) agar using a sterile swab [11, 12, 13, 16, 17, 18].
Antifungal Susceptibility Testing
Antifungal susceptibility was assessed using the disc diffusion method according to the manufacturer’s instructions, with a 0.5 McFarland inoculum for each isolate. Quality control was ensured using C. albicans ATCC 90028 and C. tropicalis ATCC 750 strains for both identification and susceptibility testing. The antifungal discs tested were fluconazole (25µg), ketoconazole (15µg), clotrimazole (10µg), nystatin (10µg), miconazole (10µg), and amphotericin B (10µg). Discs were placed on MH agar inoculated with Candida isolates and incubated at 37 °C for 24 hours [12, 13, 16, 17]. For data analysis, isolates with intermediate susceptibility were considered resistant to the antifungal agent tested. Multidrug resistance was defined as resistance to at least three antifungal agents.
Statistical Analysis
Data were entered into Microsoft Excel (Microsoft Corporation, Seattle, USA) and analysed using Statview software V5.0. Statistical significance was considered with p < 0.05. Qualitative variables were compared using Chi- square or Fisher’s exact test as appropriate.
Ethical Considerations
The study protocol was approved by the National Ethics Committee for Research (Protocol N° 0027/2022/CNER/ SG/P). Research authorisations were also obtained from CHUL authorities. Oral informed consent was obtained from each participant (or guardian when applicable) after study explanations. Confidentiality was maintained by anonymising participants with identification numbers. All study participants received medical care at the IDW-CHUL.
Results
Epidemiological Characteristics of the Study Population
A total of 107 PLHIV provided stool samples for analysis. The median age was 42 [35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49] years with a sex ratio of 2.3 (Table 1). More than three-quarters of participants were single, and 47.6% (n=51/107) had been diagnosed with HIV for 2-10 years. Only 13.1% (n=14/107) were not receiving ART. Among those with recent CD4 counts available, more than half were immunosuppressed, with a median CD4 count of 185 [100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148, 149, 150, 151, 152, 153, 154, 155, 156, 157, 158, 159, 160, 161, 162, 163, 164, 165, 166, 167, 168, 169, 170, 171, 172, 173, 174, 175, 176, 177, 178, 179, 180, 181, 182, 183, 184, 185, 186, 187, 188, 189, 190, 191, 192, 193, 194, 195, 196, 197, 198, 199, 200, 201, 202, 203, 204, 205, 206, 207, 208, 209, 210, 211, 212, 213, 214, 215, 216, 217, 218, 219, 220, 221, 222, 223, 224, 225, 226, 227, 228, 229, 230, 231, 232, 233, 234, 235, 236, 237, 238, 239, 240, 241, 242, 243, 244, 245, 246, 247, 248, 249, 250, 251, 252, 253, 254, 255, 256, 257, 258, 259, 260, 261, 262, 263, 264, 265, 266, 267, 268, 269, 270, 271, 272, 273, 274, 275, 276, 277, 278, 279, 280, 281, 282, 283, 284, 285, 286, 287, 288, 289, 290, 291, 292, 293, 294, 295, 296, 297, 298, 299, 300, 301, 302, 303, 304, 305, 306, 307, 308, 309, 310, 311, 312, 313, 314, 315, 316, 317, 318, 319, 320, 321, 322, 323, 324, 325, 326, 327, 328, 329, 330, 331, 332, 333, 334, 335, 336, 337, 338, 339, 340, 341, 342, 343, 344, 345, 346, 347, 348] cells/mm³ (Table 1). The WHO clinical stage was reported for 106 participants; 41.5% (n=44/106) were in an advanced stage of disease. The mean interval between HIV diagnosis and inclusion in the study was 7.3 (±5.4) years.
| N | % | |
|---|---|---|
| Age group | ||
| < 55 years | 94 | 87.9 |
| ≥ 55 years | 13 | 12.1 |
| Gender | ||
| Male | 32 | 29.9 |
| Female | 75 | 70.1 |
| Occupation | ||
| Manager | 29 | 27.1 |
| Worker | 45 | 42 |
| Unemployed | 33 | 30.9 |
| Matrimonial status | ||
| Single | 84 | 78.5 |
| Married/widowed | 23 | 21.5 |
| Alcohol consumption | 41 | 38.3 |
| Time since HIV diagnosis | ||
| 1 year | 22 | 20.5 |
| 2-5 years | 27 | 25.2 |
| 6-10 years | 24 | 22.4 |
| > 10 years | 34 | 31.8 |
| ART | 93 | 86.9 |
| CD4 count measurement | 96 | 89,7 |
| CD4 group (cell/mm3) | ||
| ≤ 200 | 60 | 62,5 |
| 201-499 | 23 | 23,9 |
| > 499 | 13 | 13,5 |
| Antifungal therapy | 42 | 39,3 |
| WHO Stage | ||
| I | 52 | 48,6 |
| II | 10 | 9,3 |
| III | 42 | 39,3 |
| IV | 2 | 2,8 |
| Gastrointestinal symptoms | ||
| Diarrhoea | 15 | 14,0 |
| No diarrhoea | 92 | 86,0 |
Table 1: General Characteristics of Study Population.
Frequency of Intestinal Colonisation by Candida sp
Candida sp was isolated from 73 stool samples, representing a colonisation prevalence of 68.2%. Women (79.7%) were significantly more frequently colonised than men (p=0.04) (Table 2). No significant association was found between Candida colonisation and age, ART status, CD4 count, WHO stage, or the presence of diarrhoea (Table 2).
| n | % | p | |
|---|---|---|---|
| Age group | |||
| < 55 years | 64 | 68.1 | |
| ≥ 55 years | 9 | 69.2 | |
| Sex | |||
| Male | 17 | 53.1 | |
| Female | 56 | 74.7 | |
| ART | |||
| Yes | 64 | 68.8 | |
| No | 9 | 64.3 | |
| CD4 group (cell/mm3) | |||
| [0-200] | 41 | 68.3 | |
| [201-499] | 16 | 69.6 | |
| >499 | 9 | 69.3 | |
| OMS Stage | |||
| I | 38 | 73.1 | |
| II | 8 | 80 | |
| III | 26 | 61.9 | |
| IV | 1 | 50 | |
Table 2: Prevalence of Intestinal Candidiasis According to the Characteristics of the Study Population.
Candida Species Isolated from Stool Samples
Of the 73 positive samples, species identification was successful in 71. C. albicans (32.7%; n=35) and C. glabrata (31.8%; n = 34) were the most frequently isolated species. C. krusei was detected in 8 samples (7.5%), while C. tropicalis was not identified. In 4 cases (5.6%), C. albicans was found in association with another species, either C. krusei or C. glabrata.
Antifungal Susceptibility of Candida spp Isolates
Antifungal susceptibility testing was performed for 61 isolates (Table 3). Overall, 12 isolates (19.7%) were susceptible to all antifungals tested, 13 (21.3%) were resistant to a single agent, and 15 (24.6%) showed resistance to all six antifungals tested. The overall prevalence of multidrug- resistant Candida spp was 50.8% (n=31).
| C. albicans (N=31) | C. krusei (N=5) | C. glabrata (N=25) | ||
|---|---|---|---|---|
| Fluconazole | Resistant n (%) | 25 (80.6) | 5 (100.0) | 13 (53.0) |
| Ketoconazole | Resistant n (%) | 12 (38.7) | 2 (40.0) | 11 (44.0) |
| Miconazole | Resistant n (%) | 23 (74.2) | 5 (100.0) | 18 (72.0) |
| Amphotericin B | Resistant n (%) | 13 (41.9) | 4 (80.0) | 10 (40.0) |
| Clotrimazole | Resistant n (%) | 12 (38.7) | 2 (40.0) | 10 (40.0) |
| Nystatin | Resistant n (%) | 8 (25.8) | 2 (40.0) | 7 (28.0) |
Table 3: In Vitro Susceptibility of Candida Spp. Isolates to the Different Antifungal Agents Tested.
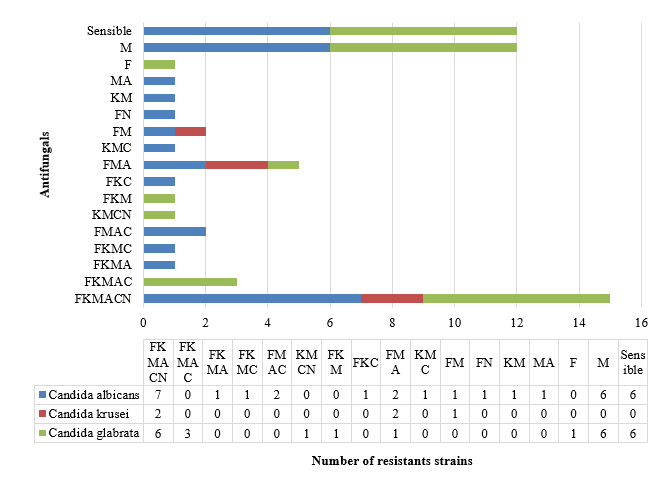
In vitro susceptibility testing revealed that C. albicans isolates were resistant in 22.6% (n=7), had intermediate susceptibility in 58.1% (n=18), and were fully susceptible in 19.3% (n=6) of cases. C. glabrata isolates showed resistance in 24.0% (n=6), intermediate susceptibility in 52.0% (n=13), and full susceptibility in 24.0% (n=6). C. krusei isolates displayed reduced susceptibility in three of five cases, while the remaining two were resistant (Figure 1). In subsequent analyses, isolates with intermediate susceptibility were categorised as resistant.
Overall, resistance was most frequently observed to miconazole (75.4%; n=46), followed by fluconazole (70.5%;
n=43), ketoconazole (41.0%; n=25), clotrimazole (39.3%; n=24), amphotericin B (44.3%; n=27), and nystatin (27.9%; n = 17).
More than half of C. albicans isolates (51.6%) were resistant to fluconazole, and 74.2% were resistant to miconazole. All C. krusei isolates were resistant to fluconazole. Among C. glabrata isolates, 72% were resistant to miconazole, and one isolate was resistant to five antifungal agents. At least one isolate of each of the three tested species (C. albicans, C. glabrata, C. krusei) exhibited resistance to fluconazole, miconazole, and amphotericin B (Figure 1).
Discussion
There are limited African data on intestinal colonisation by Candida spp in PLHIV, even though these yeasts are integral components of the intestinal mycobiome, which plays a crucial role in maintaining microbiota balance, metabolic stability, and host immune responses [3]. Within the gut mycobiome, Candida albicans has been associated with modulation of local mucosal immune responses, as well as innate and adaptive immunity [3]. Moreover, the onset of candidemia in immunocompromised individuals is often preceded by heavy intestinal colonisation with C. albicans detected in stool [3]. Alterations of the intestinal microbiota, including an overgrowth of Candida sp, have been implicated in progression to AIDS [1, 19]. If the suggested links between intestinal colonisation, mycobiome alterations, AIDS progression, and the risk of invasive candidiasis are confirmed, assessing the diversity and density of intestinal fungal populations could serve as an indicator for invasive candidiasis or disease progression.
The prevalence of intestinal Candida colonisation was 68.2%, with more than three-quarters of cases being asymptomatic. This rate is considerably higher than those reported in India (9.7%) and Iran (0.05%) [15, 20]. Only few studies have specifically assessed intestinal colonisation in PLHIV; most investigations of digestive candidiasis in this population have focused on oropharyngeal and oesophageal infections, which are recognised as major opportunistic infections. Nevertheless, intestinal colonisation rates comparable to ours have been reported in Ghana (75.3%), Chad (34%), Ethiopia (37.5%), and Cameroon (42%) [8, 21, 22, 23]. The high prevalence observed in our study may be explained by the high proportion (>60%) of immunocompromised patients, since gastrointestinal CD4+ T lymphocytes are preferential HIV targets. Their depletion leads to mucosal barrier damage, disruption of the gut microbiota, and enhanced susceptibility to colonisation [24].
Candida colonisation was significantly more frequent in women (74.7%) than in men. This finding could reflect the greater vulnerability of women to HIV infection as well as their higher rates of healthcare attendance. Colonisation was not significantly associated with age, ART exposure, CD4 count, or WHO stage. The relatively small sample size and the predominance of older participants (>55 years), most of whom were on ART and had CD4 counts <500 cells/ mm³, may have limited the statistical power to detect such associations. Previous studies have consistently shown a relationship between CD4 cell count and candidiasis, particularly oropharyngeal forms [7, 8, 19, 25].
Esebelahie NO, et al. [5] reported that CD4 counts <200 cells/µL in ART-naïve patients were predictive of candidiasis.
ART-mediated immune reconstitution, through CD4 recovery, is known to reduce the incidence of candidiasis [1]. In our study, intestinal colonisation was comparable between ART users and non-users, which could be partly explained by poor adherence to ART a factor not directly assessed here. Barriers such as financial constraints, lack of psychosocial support, limited awareness of the need for regular follow- up, adverse drug effects, stigma, and asymptomatic disease progression are known to affect ART adherence and thus favour opportunistic infections [14, 26].
The predominance of non-albicans Candida species is another important finding. C. glabrata (47.9%) was more frequent than C. albicans (43.7%). C. glabrata has been associated with more severe and treatment-refractory infections compared to C. albicans [27]. While C. albicans remains the most common cause of candidiasis, increasing rates of non-albicans species in digestive infections among PLHIV and other immunocompromised populations have been increasingly documented [6, 10, 15]. Selective antifungal pressure, particularly from fluconazole widely used for both treatment and prophylaxis of cryptococcal meningitis may contribute to the emergence of non-albicans species [28]. This selective pressure is especially relevant for C. krusei and C. glabrata, which are intrinsically resistant or dose- dependent susceptible to fluconazole, respectively [29, 30]. Co-infections, also observed in our cohort, may further enhance azole resistance [31].
More than 80% of isolates were resistant to at least one antifungal, with resistance being more common to azoles than to polyenes. The highest resistance rates were observed to miconazole (75.2%), fluconazole (70.5%), and ketoconazole (41.0%). Comparable findings have been reported in Uganda, where resistance to fluconazole (77.1%) and amphotericin B (94.1%) was observed in PLHIV [32]. Conversely, an Ethiopian study reported fluconazole susceptibility in 85.6% of isolates [30]. High resistance rates to azoles may be attributed to their frequent use as therapeutic alternatives to amphotericin B [33]. Fluconazole, is widely used in Gabon due to its affordability, availability, oral formulation, and lower toxicity. High resistance to miconazole has also been reported in Brazil (65.6%) [34]. Cross-resistance among azoles, due to shared mechanisms of action, likely explains the high rates of resistance observed in our setting, even though miconazole use is limited. Amphotericin B is the second most commonly used antifungal in hospital settings, which may account for the higher resistance rates observed compared to literature reports, where susceptibility often exceeds 95% [8, 34]. By contrast, most isolates remained susceptible to nystatin, which is rarely used in clinical practice. This suggests that nystatin could be considered as an alternative in settings where azole efficacy continues to decline.
Species-specific resistance patterns were also evident. All five C. krusei isolates were resistant to at least two antifungals, including fluconazole and miconazole, reflecting their intrinsic resistance to azoles and reduced susceptibility to other antifungals, including amphotericin B [35]. Prolonged fluconazole use may also explain the progressive replacement of C. albicans by resistant non-albicans species. Among C. glabrata isolates, all strains resistant to miconazole also exhibited multidrug resistance involving fluconazole; nearly 50% (n=9/19) were resistant to at least five antifungals, compared with less than 30% (n=7/25) of C. albicans isolates. Profiles of multidrug resistance involving 4-6 antifungals have rarely been reported in sub-Saharan Africa [36]. Lackner M, et al. [37] highlighted that pan- azole and amphotericin B resistance, though uncommon, is not rare [37]. Such resistance is linked to mutations in ERG2, ERG3, and ERG5 genes, particularly in C. glabrata and C. parapsilosis. The first case of pan-azole and polyene resistance was reported by Sida H, et al. [7].
This study has some limitations. First, it was a monocentric study, conducted among PLHIV with advanced disease, which limits the generalisability of findings to other populations. Second, budgetary constraints precluded the use of more advanced identification methods such as MALDI-TOF, PCR, or sequencing. Nonetheless, our study provides valuable preliminary insights into the diversity and resistance profile of intestinal Candida sp in PLHIV in Gabon, a field with limited data both locally and globally. Further studies including molecular characterisation of isolates, larger and more diverse samples (including asymptomatic PLHIV, HIV-negative individuals, children, and pregnant women) are needed.
Conclusion
Intestinal colonisation by Candida sp is highly prevalent among PLHIV in Gabon, with an increasing emergence of non- albicans species. Most isolates were resistant to fluconazole, the most widely used antifungal agent in both outpatient and inpatient settings. These findings underscore the urgent need to expand epidemiological and resistance surveillance of candidiasis in PLHIV and to update therapeutic guidelines for the management of these infections.
Acknowledgements
We would like to thank the participating patients, as well as the technical staff of the Department of Parasitology and Mycology at the University of Health Sciences of Libreville and the Infectious Diseases Ward of the University Hospital of Libreville for their support in providing reagents, collecting biological material, and analysing the samples.
References
-
Meng P, Zhang G, Ma X, Zhang Y, Li H, et al. (2024) Characterization of intestinal fungal community diversity in people living with HIV/AIDS (PLWHA). AIDS Res Ther 21-1: 10.
-
Kumamoto CA, Gresnigt MS, Hube B (2020) The gut, the bad and the harmless: Candida albicans as a commensal and opportunistic pathogen in the intestine. Curr Opin Microbiol 56: 7-15.
-
Koh AY (2013) Murine models of Candida gastrointestinal colonization and dissemination. Eukaryot Cell 12(11): 1416-1422.
-
Oyom AP, Okello E, Acam V, Odur B, Oyet C, et al. (2020) Prevalence and antifungal susceptibility of gastrointestinal candidiasis among diabetic patients: cross-sectional study. Afr J Lab Med 9(1): 1-7.
-
Esebelahie NO, Enweani IB, Omoregie R (2013) Candidiasis colonisation in asymptomatic HIV patients attending a tertiary hospital in Benin City, Nigeria. Lybian J Med 8: 20322-20326.
-
Kaur R, Mehra B, Dhakad MS, Goyal R, Sharma A, et al. (2018) Clinico-mycological analysis and antifungal resistance pattern in human immunodeficiency virus- associated candidiasis: an indian perspective. Indian Journal of Sexually Transmitted Diseases and AIDS 39(2): 111-119.
-
Sida H, Pethani J, Dalal P, Patel D, Shah M, et al. (2017) Study of Changing Trend in the Clinical Distribution of Candida Species in Various Clinical Samples at Tertiary Care Hospital, Ahmedabad, Gujarat. Ntl J Community Med 8(3): 109-111.
-
Mulu A, Kassu A, Anagaw B, Alemayehu M, Moges B, et al. (2013) Frequent detection of ‘azole’ resistant Candida species among late presenting AIDS patients in northwest Ethiopia. BMC Infectious Diseases 13: 82-91.
-
Gonsu Kamga H, Tchaptchet A, Ndebi M, Nouetchognou JS, Ndam EC, et al. (2014) Antifungal sensitivity of Candida spp. isolated from digestive candidiasis in HIV- positive subjects in Yaoundé, Cameroon. Health Sci Dis 15(3): 1-6.
-
Andambounou TAS, Gbadamassi AG, Efalou P, Tagbor KC, Awoke K, et al. (2020) Factors associated with death in tuberculosis/HIV co-infected patients in Togo. Review of current respiratory diseases 12(1): 164-5.
-
Daef E, Moharram A, Eldin SS, Hassan A, Fawzi M, et al. (2014) Evaluation of chromogenic media and seminested PCR in the identification of Candida species. Braz J Microbiol 45: 255-262.
-
Wayne PC (2018) Clinical and Laboratory Standards Institute (CLSI). Method for Antifungal Disk Diffusion Susceptibility Testing of Yeasts. 3rd ed. CLSI guidelines M44.
-
Khadka S, Sherchand JB, Pokhrel BM, Adhikari N, Rijal KR, et al. (2017) Isolation, speciation and antifungal susceptibility testing of Candida isolates from various clinical specimens at a tertiary care hospital, Nepal. BMC Res Notes 10: 218.
-
Manomba Boulingui C, Moutombi Ditombi B, Mihindou JC, Owono F, Nkoghe D, et al. (2023) Adverse effects related to antiretroviral drugs in people living with HIV in Gabon: frequency, severity and relationship with adherence. Health Sci Dis 24(3): 16-23.
-
Kaur R, Dhakad MS, Goyal R, Kumar R, Chakrabarti A, et al. (2016) Spectrum of opportunistic fungal infections in HIV/AIDS patients in Tertiary Care Hospital in India. Canadian Journal of Infectious Diseases and Medical Microbiology: 1-7.
-
Beighton D, Ludford R, Clark DT, De Silva S, Brailsford S, et al. (1995) Use of CHROM agar Candida medium for isolation of yeasts from dental samples. J Clin Micro 33(11): 3025-3027.
-
Lamichhane K, Adhikari N, Bastola A, Khatri B, Poudel P, et al. (2020) Biofilm-Producing Candida Species Causing Oropharyngeal Candidiasis in HIV Patients Attending Sukraraj Tropical and Infectious Diseases Hospital in Kathmandu, Nepal. HIV/AIDS - Research and Palliative Care 12: 211–220.
-
Zhang F, Aschenbrenner D, Yoo JY, Zuo T, Ng SC, et al. (2022) The gut mycobiome in health disease and clinical application in association with the gut bacterial microbiome assembly. Lancet Microbe 3(12): e969-e983.
-
Gerges MA, Fahmy YA, Hosny T, El-Shenoufy M, Elmasry A, et al. (2023) Biofilm formation and aspartyl proteinase activity and their association with azole resistance among Candida albicans causing vulvovaginal candidiasis, Egypt. Infection and drug resistance 16: 5283-93.
-
Anwar Khan P, Malik A, Subhan Khan H (2012) Profile of candidiasis in HIV infected patients. Iranian Journal of Microbiology 4(4): 204-9.
-
Kwamin F, Nartey NO, Codjoe FS, Boahene I, Glover R, et al. (2013) Distribution of Candida species among HIV-positive patients with oropharyngeal candidiasis in Accra, Ghana. J Ingect Dev Ctries 7(1): 41-5.
-
Taverne-Ghadwal T, Kuhns M, Buhl T, Eberle J, Frickmann H, et al. (2022) Epidemiology and prevalence of oral candidiasis in HIV patients from Chad in the post-HAART Era. Front Microbiol 13: 844069.
-
Ambe NF, Longdoh NA, Tebid P, Atanga MB, Njim T, et al. (2020) The prevalence, risk factors and antifungal sensitivity pattern of oral candidiasis in HIV/AIDS patients in Kumba district Hospital, Southwest Region, Cameroon. Pan Afr Med J 36: 23.
-
Bandera A, De Benedetto I, Bozzi G, Gori A, Clerici M, et al. (2018) Altered gut microbiome composition in HIV infection: causes, effects and potential intervention. Curr Opin HIV AUD 13(1): 73-80.
-
El-Kholy MA, Shawky SM, Helaly GF, Fahmy HS, Fayed L, et al. (2018) Virulence factors, antifungal susceptibility profile and possible mechanisms of azole resistance among Candida tropicalis isolates, Alexandria, Egypt. Revista Română de Medicină de Laborator Supliment 2 26(3): S27-S28.
-
Loveday M, Hlangu S, Manickchund P, Lalla-Edward S, Osman M, et al. (2024) Not taking medications and taking medication, it was the same thing: perspectives of antiretroviral therapy among people hospitalized with advanced HIV disease. BMC Infect Dis 24(1): 819.
-
Moges B, Bitew A, Shewaamare A, (2016) Spectrum and the in vitro antifungal susceptibility pattern of yeast isolates in Ethiopia HIV patients with oropharyngeal candidiasis. Int J Micobiol 3037817.
-
Ruhnke M (2006) Epidemiology of Candida albicans infections and role of non-Candida albicans yeasts. Curr Drug Targets 7(4): 495-540.
-
Chabasse D, Pihet M, Bouchara JP (2009) Emergence of new pathogenic fungi in medicine: a general review. French-language journal of laboratories 416: 71-86.
-
Seyoum E, Bitew A, Mihret A (2020) Distribution of Candida albicans and non-albicans Candida species isolated in different clinical sample and their in vitro antifungal susceptibility in Ethiopia. BMC Infect Dis 20(1): 231.
-
Terças AL, Marques SG, Moffa EB, Figueiredo-Godoi LMA, Vieira MMF, et al. (2017) Antifungal drug susceptibility of Candida species isolated from HIV-positive patients recruited at a public hospital in Sao Luis, Maranhao, Brazil. Front Microbiol 8: 298.
-
Benson M, Turyamuhika L, Mwesigwa A, Luwangula D, Namugga J, et al. (2024) Distribution and antifungal susceptibility profile of oropharyngeal Candida species isolated from people living with HIV in the era of universal test and treat policy in Uganda. Ther Adv Infect Dis 11: 1-15.
-
Deorukhkar SC, Saini S (2013) Vulvovaginal candidiasis due to non albicans Candida: its species distribution and antifungal susceptibility profile. Int J Curr Microbiol App Sci 2(12): 323-328.
-
Quieroz Freitas VA, Santana Santos A, Amâncio Zara ALS, Oliveira PM, Ribeiro FC, et al. (2022) Distribution and antifungal susceptibility profiles of Candida species isolated from people living with HIV/AIDS in a public hospital in Goiânia, GO, Brazil. Braz J Microbiol 54(1): 125-133.
-
Lyon GM, Karatela S, Sunay S, Adiri Y, Blumberg HM, et al. (2010) Antifungal susceptibility testing of Candida isolates from the Candida surveillance study. J Clin Microbiol 48(4): 1270-1275.
-
Müller FMC, Weig M, Peter J, Seibold M, Holl R, et al. (2000) Azole cross-resistance to ketoconazole, fluconazole, itraconazole and voriconazole in clinical Candida albicans isolates from HIV-infected children with oropharyngeal candidosis. J Antimcrob Chemother 46: 338-341.
-
Lackner M, Martin-Vincente A, Lass-Florl C, (2015) Multidrug- and cross-resistant Candida: the looming threat. Curr Fungal Infection Rep 9: 23-36.
- Vulvovaginal candidiasis: Retrospective study (2019- 2021) at the Centre Hospitalier National de Pikine, Suburban Dakar, Senegal
- Identification of Environmental Fungal Species in Clinical Services of University Hospital of Angre, Abidjan (Cote d’Ivoire)
- New Location of some Gasteroid Basidiomycetes in Western Kazakhstan
- Evaluation of Various Extracellular Enzymes of Ectomycorrhizal Mushrooms
- Morphology and Phylogeny of Lactarius Wallichianae sp. nov and Xerula magnispora sp. nov. from India
- Growth of Pleurotus Florida (Oyster Mushroom) on Different Media