Retinal Nerve Fiber Layer Thickness and Optic Disc Parameters in Anisometropic Amblyopia by Cirrus HD OCT in Pediatric Population
Background: To compare the peripapillary retinal nerve fiber layer (RNFL) thickness and characteristics of optic disc parameters in amblyopic and fellow eyes in pediatric patients with an isometropic amblyopia by Cirrus HD OCT. Method: This study was a prospective, cross-sectional, study including thirty-five subjects of newly diagnosed anisometropic amblyopia. All children underwent an ophthalmic examination that included visual acuity, and optical coherence tomography (Cirrus OCT Zeiss, 'Optic Disc Cube 200×200' protocol). Measurement of the Retinal nerve fiber layer and optic nerve head parameters (ONH) was done for both amblyopic and normal fellow eyes. Results: The mean best corrected visual acuity (log MAR scale) of the normal eyes and the amblyopic eye was statistically significant (P
Neelam P*, Kshitij S, Meenakshi R, Devendran M and Ramakrishnan R
Aravind Eye Hospital, India
layer and optic nerve head parameters (ONH) was done for both amblyopic and normal fellow eyes.
parameters were significantly different between the investigated eyes.
significantly different.
Cirrus HD OCT
Introduction
Amblyopia is defined as a decrease of visual acuity for which no causes can be detected by the physical examination of the eye, caused by vision deprivation or abnormal binocular interaction [1]. Amblyopia is the one of the most common cause of visual loss in children affecting 0.2% to 1.1% of school going children. The causes of amblyopia in decreasing order of prevalence are strabismic, anisometropic, mixed, ametropic, meridional and sensory deprivation amblyopia [1, 2]. A difference in refractive error between the two eyes (anisometropia) is a common cause of amblyopia, being present as the only identifiable amblyogenic factor in 37% of cases and present concomitantly with strabismus in an additional 24% of clinical populations [2]. The literature and experimental studies had described the pathophysiology structural changes in amblyopia at different levels of the visual information processing pathway. The anatomical changes have been described at the cortical, lateral geniculate body and retinal levels [3]. There tinal nerve fiber layer thickness (RNFL) thickness studies with optical coherence tomography (OCT) have been done in various ethnic population in pediatric and adult age group with amblyopia [3, 4, 5, 6, 7, 8, 9, 10]. Various studies have described changes in all children irrespective of whether they were newly diagnosed, persistent or resistant to occlusion and refractory therapy. Changes in peripapillary and macular area have been shown to be inconsistently related to the amblyopic status of the eye [11, 12, 13, 14, 15, 16, 17]. Studies using OCT imaging of the retina have variable results, some studies have found an increased peripapillary RNFL or/and macular thickness in amblyopic eyes, whereas others have found no significant differences between amblyopic and healthy eyes [17, 18, 19, 20, 21, 22, 23, 24].
There has been scarcity of literature describing the changes in optic nerve parameters (ONH) and twelve sector RNFL changes in anisometropic ambylopia. Hence, the present study was done to evaluate the changes in thickness of RNFL and optic disc parameters in pediatric patients with newly diagnosed anisometropic amblyopia.
Materials and Methods
This study was conducted at the Department of Pediatric Ophthalmology at Aravind Eye Hospital. This study adhered to the Declaration of Helsinki and was approved by the institutional review board. Informed consent was taken from parents or guardians. Unilateral amblyopia was defined as a best corrected visual acuity (BCVA) of at least a two-line difference between the amblyopic and fellow eye. All the patients aged 5 to 17 yrs with newly diagnosed anisometropic amblyopia (defined as 1 D or greater in spherical equivalent, or a 1.5 D or greater difference in astigmatism between both the eyes in the absence of any measurable heterotropia at distance or near) with normal appearing disc, cup and neuroretinal rim on examination of the optic nerve head with + 90D aided stereoscopic slit - lamp indirect ophthalmoscopes were enrolled in the study. Patients with strabismus, ocular motility disorders, any pathologies of retinal nerve fibre layer or disc, family history of glaucoma or any intraocular surgery or any kind of laser therapy, mentally challenged children, any systemic diseases affecting eye were excluded from study. All subjects received a full ophthalmic examination including cycloplegic refraction, assessment of ocular motility, slit-lamp biomicroscopic evaluation, dilated fundus examination and axial length by IOL master© (Carl Zeiss Meditec, Dublin, CA) (ver. 5.2.1). Pupils were dilated with tropicamide 1% and cyclopentolate 1% drops, depending on age of the subject. RNFL was measured through dilated pupils using a 3rd generation optical coherence tomographer (Cirrus OCT©, model HD-OCT 4000, Carl Zeiss Meditec, Dublin, CA) (ver.3.0.0.64). Peripapillary measurements were measured using the fast scan protocol (fast RNFL thickness scan). Three 200×200-cube optic disc scans were done successively, with a total acquisition time of 1.5 s. The average of the 3 scans was analyzed. All scans were performed by the same investigator. An internal fixation target was used in all scans, and the location of each scan on the retina was monitored on the built-in infrared-sensitive video camera. The mean RNFL thicknesses at 256 cubes of the RNFL thickness were recorded and the average RNFL thicknesses in all quadrants were analyzed. RNFL thickness (all four quadrants: superior, nasal, inferior and temporal, average, and clock hours), RNFL symmetry, rim area, disc area, average C/D ratio, vertical C/D ratio and cup volume were recorded. For the clock hour RNFL thicknesses, twelve 30° sectors were defined in clockwise order for the right and left eyes; in that respect, clock hour 1 in the right eye corresponded to clock hour 11 in the left eye, clock hour 2 in the right eye corresponded to clock hour 10 in the left eye, 3–9, 4–8, 5– 7 respectively, etc.
Statistical Analysis
The BCVA was transformed to logarithm of the minimum angle of resolution (log MAR) units for the statistical analysis. Mean (SD) or frequency (percentage) was used to describe summary data. Paired t-test / Wilcoxon Signed Rank test was used to test mean difference of retinal nerve fibre layer thickness and ocular parameters between amblyopic eye and normal eye. P-value less than 0.05 were considered as statistically significant. All the statistical analysis was performed using STATA 11.1© (Texas, U.S.A).
Results
The mean age of patients was 9.83 ±3 (5-17 years). There were 19 myopic and 16 hypermetropic anisometropes. The clinical characteristics of normal and amblyopic eyes are described in (Table1). The average RNFL thickness in the normal eye was 96.34 ± 9.3 µm (range 76 – 122 µm) while that of the amblyopic eye was 97.94 ± 11 µm (range 77-125 µm) which was not significant (P= 0.294).
| Normal Eye | Amblyopic Eye | P - value | |
|---|---|---|---|
| Axial length(mm) | 23.04(1.0) | 23.07(1.4) | 0.544 |
| Axial length(mm) | 20.75 - 25.33 | 20.65 - 27.08 | 0.544 |
| BCVA Log mar | 0(0) | 0.55(0.3) | <0.001 |
| BCVA Log mar | 0 - 0 | 0.3 - 1.18 | <0.001 |
| Spherical Equivalent | -0.24(1.2) | -0.41(4.2) | 0.780 |
| Spherical Equivalent | -5.25 to 1.75 | -13 to 7.5 | 0.780 |
| RNFL(μm) | 96.34(9.3) | 97.94(11.0) | 0.294 |
| RNFL(μm) | 76 - 122 | 77 - 125 | 0.294 |
Table1: Clinical characteristics of the 35 patients with anisometopic amblyopia included in the study.
SD Standard Deviation, RNFL, retinal nerve fiber layer. The (Table 2) shows the relationship of the average peripapillary RNFL thickness in all the four quadrants between normal and amblyopic eyes. The relationship between mean RNFL in the inferior, superior, temporal quadrant of the normal and amblyopic eye were not statistically significant except in nasal quadrant (P= 0.027).
| Normal Eye | Amblyopic Eye | P - value | |
|---|---|---|---|
| Superior | 120.74(14.9) | 122.77(23.7) | 0.706 |
| Superior | 95 - 170 | 75 - 183 | 0.706 |
| Temporal | 63.17(9.4) | 66.42(14.0) | 0.209 |
| Temporal | 48 - 87 | 46 - 116 | 0.209 |
| Inferior | 129.09(13.2) | 125.89(18.5) | 0.456 |
| Inferior | 104 - 162 | 70 - 158 | 0.456 |
| Nasal | 72.37(12.1) | 76.86(12.7) | 0.027 |
| Nasal | 46 - 96 | 49 - 101 | 0.027 |
Table 2: Comparison of the Quadrant RNFL parameters between the amblyopic and fellow eyes Table 2: Comparison of the Quadrant RNF
| Optic Nerve Head parameters Mean(SD) Range | Normal Eye | Amblyopic Eye | P - value |
| Rim Area (mm2) | 1.59±0.3 | 1.62±0.3 | 0.526 |
| Rim Area (mm2) | 1.02-2.4 | 1.09-2.33 | 0.526 |
| Disc area(mm2) | 2.22(0.5) | 2.15(0.3) | 0.413 |
| 1.46 - 3.66 | 1.67 - 2.83 | ||
| Average CD ratio | 0.49(0.2) | 0.45(0.2) | 0.042 |
| Average CD ratio | 0.09 - 0.74 | 0.06 - 0.72 | 0.042 |
| Vertical CD ratio | 0.47(0.2) | 0.43(0.2) | 0.059 |
| Vertical CD ratio | 0.07 - 0.7 | 0.05 - 0.74 | 0.059 |
| Cup volume (mm³) | 0.19(0.2) | 0.16(0.2) | 0.023 |
| Cup volume (mm³) | 0 - 0.68 | 0 - 0.673 | 0.023 |
Table3: Comparison of the ONH parameters between the amblyopic and fellow eyes.
Abbreviations: C/D, cup-to-disc
There was a positive correlation between spherical equivalent and RNFL thickness in amblyopic eye (Correlation coefficient 0.5123, P =0.0017). There was a negative correlation between axial length and RNFL thickness of the amblyopic eye (Correlation coefficient - 0.5124, P =0.0016) (Figure a & b).
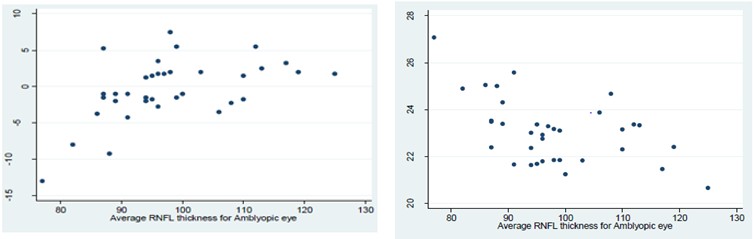
Figure a: Correlation between Spherical Equivalent and RNFL thickness in Amblyopic eye.
Figure b: Correlation between Axial length and RNFL thickness in Amblyopic eye.
There was a positive correlation between spherical equivalent and RNFL thickness (P=0.0017) while negative correlation between Axial length and RNFL thickness in ambyloic eyes. (P =0.0016) The (Table 4) shows relationship between the mean disc area, mean rim area, and mean vertical CD ratio of the normal eye and the amblyopic eye to be statistically insignificant (P >0.05). The mean average cup-to-disc area ratio and cup volume was lesser in the amblyopic eyes than in the fellow eyes (P=0.042, P=0.023 respectively).
| Normal Eye | Amblyopic Eye | P - value | |
|---|---|---|---|
| S | 124.17(20.9) | 126.60(31.9) | 0.787 |
| S | 83 - 203 | 71 - 196 | 0.787 |
| SN | 113.34(24.6) | 116.74(31.0) | 0.451 |
| SN | 70 - 165 | 72 - 198 | 0.451 |
| NS | 93.31(17.0) | 98.34(19.9) | 0.184 |
| NS | 61 - 128 | 51 - 140 | 0.184 |
| N | 57.20(11.0) | 60.40(12.3) | 0.376 |
| N | 27 - 78 | 27 - 78 | 0.376 |
| NI | 67.51(14.3) | 72.14(16.7) | 0.101 |
| NI | 41 - 101 | 47 - 111 | 0.101 |
| IN | 111.91(18.3) | 108.09(27.4) | 0.755 |
| IN | 69 - 152 | 48 - 163 | 0.755 |
| I | 145.43(21.7) | 141.83(30.4) | 0.961 |
| I | 48 - 163 | 46 - 188 | 0.961 |
| IT | 130.14(22.6) | 127.43(25.1) | 0.403 |
| IT | 90 - 184 | 67 - 181 | 0.403 |
| TI | 65.69(12.1) | 71.20(26.6) | 0.606 |
| TI | 47 - 101 | 40 - 180 | 0.606 |
| T | 49.49(7.1) | 54.43(12.5) | 0.045 |
| T | 29 - 61 | 38 - 102 | 0.045 |
| TS | 73.49(13.9) | 73.31(19.1) | 0.876 |
| TS | 38 - 102 | 38 - 102 | 0.876 |
| ST | 124.29(27.4) | 125.77(36.2) | 0.812 |
| ST | 57 - 182 | 57 - 182 | 0.812 |
Table 5: Comparison of the 12 clock hour RNFL parameters between the amblyopic and fellow eyes Table 4: Comparison of the 12 cloc
Table 4: Comparison of the 12 clock hour RNFL parameters between the amblyopic and fellow eyes Table 4: Comparison of the 12 clock hour RNFL parameters between the amblyopic and fellow eyes (S-Superior, SN-Superior-nasal, NS -Nasal-superior, N –Nasal, NI-Nasal-inferior, IN -Inferior-nasal, I-Inferior, IT-Inferior- temporal, TI-Temporal-inferior, T-Temporal , TS-Temporal-superior, ST -Superior-temporal)
Discussion
In this study we assessed the RNFL and ONH parameters of the pediatric patients with newly diagnosed unilateral amblyopia using OCT imaging. Previous OCT studies of RNFL thickness in anisometropic amblyopia have yielded inconsistent findings [10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25]. In our study, the mean average RNFL thickness in the normal eye and the amblyopic eye was insignificant (P= 0.294). In the normal eyes the RNFL thickness was well in agreement with the pediatric normative data studied by Pawar N et al. by Stratus OCT with an average RNFL thickness of (± SD) 106.11 ± 9.5 μm (range 82.26 - 146.25) [20]. Kee et al enrolled 26 unilateral amblyopic children (6 strabismic, 15 anisometropic, 5 combined amblyopes), and found no difference in RNFL between neither the amblyopic eye and fellow eye, nor between values of these amblyopic patients and 42 normal control children using time-domain OCT [5]. In the Sydney Childhood Eye Study, Huynh et al investigated 48 unilateral amblyopes (17 strabismic, 19 hyperopic anisometropia) and reported that Peripapillary RNFL thickness was not significantly different between amblyopic and normal fellow eyes or normal eyes of non- amblyopic children [6]. Repka et al. in 2006 and 2009 evaluated 17 and 37 subjects of strabismic and anisometropic amblyopia respectively and found no difference in RNFL thickness between amblyopic and sound eyes using TD-OCT [8]. Al Haddad et al found that mean RNFL thickness was similar in amblyopic (95.4 μm) and fellow eyes (94.0 μm) in strabismic and anisometropic amblyopia [11]. Bandopadhaya SK et al. in their study with anisometropic amblyopia found no changes in the peripapillary RNFL [12]. Firat et al. and Ersan et al. in their study on anisometropic and strabismic amblyopic patients found no significant difference in the mean RNFLT between the amblyopic eye, fellow eye and the eye of normal subjects (P >0.05) [13, 15].
Dickmann evaluated 15 strabismic (esotropic) and 15 anisometropic amblyopic patients, and found no inter eye differences in cpRNFL [18]. Yalcin et al. did a comparative study of peripapillary RNFL which included three groups, amblyopic and fellow normal eye of 30 hypermetropic anisometropic amblyopic subjects and normal eye of 30 normal subjects. They concluded that difference between the three groups was statistically insignificant (P = 0.285) [21]. Yassin SA et al. in their study investigated the difference in RNFL thickness between amblyopic eyes, fellow eyes of the amblyopic patients, and normal eyes of the emmetropic subjects and found no clinically significant difference between both recovered and persistent ambylopia [23]. Demircan S et al. with hyperopic anisometropic amblyopia study, found no significant difference between the amblyopic and the fellow eye [25]. Our study is consistent with previous studies showing no difference in RNFL between amblyopic and normal fellow eyes. Table 5 describes summary of previous studies employing optical coherence tomography of the RNFL thickness in pediatric patients with amblyopia.
| Study (first author, year) | Country | No. of patients | Age (years) Range | Type of amblyopia | OCT type | AL data | Spherical Equivalent | RNFL | |
|---|---|---|---|---|---|---|---|---|---|
| Yen MY 2004 | Taiwan | 38 | 26.4±18.3 | Mixed (S, A, R) | Oct-00 | Measured but not mentioned values | 0.17±3.59 | Significant in Strabismic | |
| Altintas 2005 | Turkey | 14 | 10.43±4.09 (5-18) | S | 3-Oct | ND | Nd | Not significant | |
| YoonSW 2005 | Korea | 31 | 7.7 (5-12) | Hypermetr opicamblyopia | Oct-00 | ND | 3.71 (+2 to +6.5) | Significant,Thicker | |
| Kee 2006 | Korea | 26 AE 42 NE | 8 8.5 | Mixed (S, A, AS) | 3-Oct | ND | ND | Not significant | |
| Repka 2006 | USA | 17 | 10.7 (5-30) | Mixed (S, A, AS) | Stratus OCT | ND | <+5 | Not significant | |
| Dickmann 2009 | Italy | 40 | 15.2 (5-56) | Mixed (S, A) | Stratus OCT | ND | S ≤5D AS ≤3D | Not significant | |
| Huynh 2009 | Australia | 65 | 6-12 | Mixed (S, A, AS) | Stratus OCT | IOL Master | 2.0 ±4.6 | Not significant |
| Repka 2009 | USA | 37 | 9.2±1.5 (7-12) | Mixed (S, A, AS) | Stratus OCT | ND | 2.03±1.70 | Not significant | |
| Miki 2010 | Japan | 26pesitent 25 recovered | 10.9±6.3 8.4±6 | Mixed (S, A, AS) | Stratus OCT | ND | 3.46±3.941 3.37±3.49 | Not significant | |
| Al Haddad 2011 | Lebanon | 45 | 20±12.3 | Mixed (S, A) | Cirrus HD OCT | ND | 0.8±5.2 | Not significant | |
| Dickmann 2011 | Italy | 30 | 19.7 (10-38) | Mixed (S, R) | Stratus OCT | ND | S 1±2.8 R 0.73±4.25 | Not significant | |
| Ersan 2012 | Turkey | 65 | 11.34±4.53 (5-18) | Mixed (S, A) | 3-Oct | ND | +8.5to-6.5 | Not significant | |
| Alotaibi 2011 | Saudi Arabia | 93 | 8.73 ±2.21 (5-12) | Mixed (S, A, AS) | Stratus OCT | ND | ND | Significant, Thicker | |
| Bandoupa dhaya 2012 | Indian | 39 | 16-May | A | Stratus OCT | ND | ND | Not significant | |
| Wu 2013 | China | 72 | 9.7 1.9 (5-16) | Hypermetr opic amblyopia | 3D OCT TOPCO N | ND | +2to +6.5 | Significant, Thicker | |
| Firat 2013 | Turkey | 36AE 32 normal | 12.6±5.4 (5-23) (4-24) | Mixed (S, A) | Nidek OCT RS3000 | ND | S ≤5D AS ≤3D | Not significant P=0.18 | |
| Andalib 2013 | Iran | 50 | 18-Jun | Mixed (S, A) | Stratus OCT | ND | ND | Not significant | |
| Yalcin 2014 | Turkey | 60 | 8-14 10.5 | Hypermetr opic amblyopia | Cirrus HD OCT | ND | AE +4.75 (+3 to +6) FE +1 (+0.50 to +2) | Not significant P = 0.285 | |
| Araki S 2014 | Japan | 21 | 8.5±3.5 (4-18) | Mixed (S, A, AS) | RT Vue 100 | ND | AE +3.51±3.6 NE +0.77 ±1.58 | Significant, Thicker | |
| Demircan 2015 | Turkey | 18 | 8.56±1.92 (5-12) | Hypermetr opic amblyopia | Spectralis OCT | IOL Master | AE 5.16 ±2.98 NE 1.27 ±0.83 | Not significant | |
| Our study | Indian | 37 | 9.83±3 (5-17) | Anisometropic amblyopia | Cirrus HD OCT | IOL master | NA -0.24±1.2 AE -0.41±4.2 | Not significant P=0.294 |
Table 7: Summary of previous studies employing optical coherence tomography of the RNFL thickness in pediatric Table 5: Summary o
Abbreviations: ND: no data, type of amblyopia: anisometropic amblyopia: A, strabismic amblyopia: S, combined amblyopia patients with strabismus and anisometropia: AS, AE Ambylopic eye, NE normal eye, RNFL, retinal nerve fiber layer In contrary to previous mentioned studies Yen et al. studied 38 patients of refractive, strabismic and anisometropia amblyopia and found that RNFL between the amblyopic eyes and the normal fellow eyes was statistically significant (P < 0.05) [3].
Wu SQ, et al. studied hyperopic anisometropic amblyopia and found thicker peripapillary RNFL than the contra lateral eyes in children [16]. Alotaibi, et al. in their study in 93 patients with strabismic, anisometropic and mixed ambylopia found a significantly thicker RNFL in amblyopic eye (P < 0.0001). For anisometropic amblyopic patients the mean total thickness of the retinal fiber there was statistically significant in amblyopic eyes and normal fellow eyes [17]. Araki S, et al. in their study of 21 patients with unilateral amblyopia (14 anisometropic, 4 strabismic amblyopia, and 3 with both) using spectral-domain OCT found the cpRNFL thickness (P<0.01) significantly thicker in the amblyopic eyes than in the fellow eyes. Among the ONH parameters, the rim area was significantly larger and the cup-to-disc area ratio was smaller in the amblyopic eyes than in the fellow eyes (P<0.05). None of the other ONH parameters were significantly different between the studied eyes. In our study, relationship between the mean disc area, mean rim area, and mean vertical CD ratio of the normal eye and the amblyopic eye was statistically insignificant (P >0.05) and amblyopic eyes had small average CD ration and cup volume [23]. Yoon, et al. concluded that RNFLT in the amblyopic eyes was significantly (P =0.019) thicker than the normal eyes in subjects with hyperopic anisometropic amblyopia [24]. Li J et al. in their meta-analysis of 28 clinical trials involving 408 patients observed that pRNFL thickness in the amblyopic eyes was thicker than in the fellow eyes (P= 0.016) [24]. In our study, mean RNFLT was 4.94 µm thicker in the temporal clock hour of amblyopic eye than the fellow eye, which was statistically significant (P-value 0.045). Similarly, the mean RNFLT was 4.49 µm thicker in nasal quadrant of the amblyopic than the fellow eye, the difference being statistically significant (P –value 0.027). In contrary to our study, studies done by Repka, et al. [8] Dickman, et al. [7] Firat, et al. [15] Kee SY, et al. [5] Bandhopadhya, et al. [12] Huynh, et al. [6] Quoc EB, et al. [9] and Wang, et al. [19] found no significant difference in all the four quadrants between the amblyopic and fellow eyes. Demircan, et al. [25] found no significant difference in all four quadrants and the 12 sectors when individually compared between anisometropic eye and normal eye. In present study the mean RNFL was 4.49 µm thicker in nasal quadrant of the amblyopic than the fellow eye, the difference being statistically significant (P =0.027). In contrary to our study, studies done by Repka, et al. Dickman, et al. Firat, et al. Kee SY, et al. Bandhopadhya, et al. Huynh, et al. Quoc EB, et al. and Wang et al found no significant difference in all the four quadrants between the amblyopic and fellow eyes [5, 6, 7, 8, 9, 12, 14, 15, 16, 17, 18]. Ersan, et al. reported in the hyperopic anisometropic group, temporal RNFL thickness was thinner in amblyopic eyes (66.32 ± 16.84 μm) compared to their fellow eyes (71.23 ± 15.00 μm) (P=.03), whereas in the myopic anisometropic group, superior RNFL thickness was significantly thinner in the amblyopic eyes (112.12 ± 18.54 μm) than their fellow eyes (123.12 ± 20.85 μm) (P = .05) [13]. Demircan, et al. found no significant difference in all four quadrants and the each 6 sectors centered on the optic disc ( temporal, temporal superior, temporal inferior, nasal, nasal inferior, nasal superior) by Spectralis OCT between anisometropic amblyopic and normal fellow eye [25]. We did not find any studies describing 12 clock hour sector analyses between normal and anisometropic amblyopic eyes. Few studies have taken in account of axial length in amblyopic eyes [3, 6, 25]. We found a positive correlation between the spherical equivalent and peripapillary RNFL thickness in amblyopic eye, similar to study by Ersan, et al. who found that RNFL measurements showed a significant positive correlation with spherical equivalent in the anisometropic group (both myopic and hypermetropic) [13]. While Yen, et al. showed that there was no significant correlation between RNFL thickness and spherical equivalence (P = 0.956) among all amblyopic eyes [3]. Repka, et al. also had similar conclusion of no association between RNFL thickness and hypermetropic refractive error in the amblyopic eye (P=0.81) or sound eye (P = 0.28) [8]. We had negative correlation between the axial length and RNFL of the amblyopic eyes. In contrary to our study, Yen et al. showed that there was no significant correlation between RNFL and axial length (P = 0.655) among all amblyopic eyes [3]. Araki S, et al. showed that the differences in the peripapillary RNFL thickness were significantly correlated with the difference in axial length (P<0.05, r=−0.48) and refractive error (P<0.05, r=0.50) [22]. However our study has few limitations. If a larger study population had been taken, it would be more beneficial to assess the changes mentioned above. The results can then be extrapolated to the general population. We also did not have a control group of subjects. The variables of the normal fellow eye can then be compared with the eye of the control subjects. The data obtained from our study applies only to Cirrus HD-OCT. It cannot be compared to that obtained by other spectral domain OCT machine. We did not include a correction factor in relation to age, axial length, refraction and magnification in RNFL, before subjecting it to further statistical analysis.
Conclusion
We found no difference between RNFL thickness in amblyopic and normal fellow eye however nasal quadrant, temporal clock hour sector, average CD ratio, cup volume showed significant differences. Thus some of the morphological measurements between the amblyopic and fellow eyes in patients with unilateral amblyopia were significantly different. Further studies, including histopathlogical and individual retinal layer analysis with a greater number of patients, are required to ascertain the differences between amblyopic and normal eyes.
References
-
Pediatric Eye Disease Investigator Group (2002) The clinical profile of moderate amblyopia in children younger than 7 years. Arch Ophthalmol 120(3): 281- 287.
-
Menon V, Chaudhuri Z, Saxena R, Gill K, Sachdev MM (2005) Profile of amblyopia in a hospital referral practice. Indian J Ophthalmol 53(4): 227-234.
-
Yen MY, Cheng CY, Wang AG (2004) Retinal nerve fiber layer thickness in unilateral amblyopia. Invest Ophthalmol Vis Sci 45(7): 2224-2230.
-
Altinas O, Yüksel N, Ozkan B, Caglar Y (2005) Thickness of the retinal nerve fiber layer, macular thickness, and macular volume in patients with strabismic amblyopia. J Pediatr Ophthalmol Strabismus 42(4): 216-221.
-
Kee SY, Lee SY, Lee YC (2006) Thicknesses of the fovea and retinal nerve fiber layer in amblyopic and normal eyes in children. Korean J Ophthalmol 20(3): 177-181.
-
Huynh SC, Samarawickrama C, Wang XY, Rochtchina E, Wong TY, et al (2009) Macular and nerve fiber layer thickness in amblyopia: the Sydney Childhood Eye Study. Ophthalmology 116(9):1604–1609.
-
Dickmann A, Petroni S, Salerni A, Roberto D, Emilio B (2009) Unilateral amblyopia: an optical coherence tomography study. JAAPOS 13(2): 148-150.
-
Repka MX, Kraker RT, Tamkins SM, Donny WS, Nicholas AS, et al (2009) Retinal nerve fiber layer thickness in amblyopic eyes. Am J Ophthalmol 148(1): 143-147.
-
Quoc EB, Delepine B, Tran TH (2009) Thickness of retinal fiber layer and macular volume in children and adults with strabismic and anisometropic amblyopia. J Fr Ophtalmol 32(7): 488-495.
-
Miki A, Shirakashi M, Yaoeda K, Kabasawa Yu, Satoshi U, et al (2010) Retinal nerve fiber layer thickness in recovered and persistent amblyopia. Clin Ophthalmol 20(4): 1061-1064.
-
Al-Haddad CE, Mollayess EL, Cherfan CG,Dalida J, Bashshur Z(2011) Retinal nerve fibre layer and macular thickness in amblyopia as measured by spectral-domain optical coherence tomography. Br J Ophthalmol 15(1): 11.
-
Bandyopadhyay SK, Chatterjee A, Banerjee R (2012) Peripapillary nerve fibre layer thickness and macular thickness in children with anisometropic amblyopia attending a referral centre in Eastern India. J Indian Med Assoc 110(8): 542-545.
-
Ersan I, Zengin N, Bozkurt B, Ozkagnici A (2013) Evaluation of retinal nerve fiber layer thickness in patients with anisometropic and strabismic amblyopia using optical coherence tomography. J Pediatr Ophthalmol Strabismus 50(2): 113-11.
-
Andalib D, Javadzadeh A, Nabai R, Amizadeh Y (2013) Macular and retinal nerve fiber layer thickness in unilateral anisometropic or strabismic amblyopia. J Pediatr Ophthalmol Strabismu 50(4):218-221.
-
Firat PG, Ozsoy E, Demirel S, Cumurcu T, Abuzer G (2013) Evaluation of peripapillary retinal nerve fiber layer, macula and ganglion cell thickness in amblyopia using spectral optical coherence tomography. Int J Ophthalmol 6(1): 90-94.
-
Wu SQ, Zhu LW, Xu QB,Xu JL, Zhang Y (2011) Macular and peripapillary retinal nerve fiber layer thickness in children with hyperopic anisometropic amblyopia. Int J Ophthalmol 6(1): 85-89.
-
Alotaibi AG, Enazi BA (2011) Unilateral amblyopia: Optical coherence tomography findings. Saudi Journal of Ophthalmology 25(4): 405-409.
-
Dickmann A, Petroni S, Perrotta V, Parrilla R, Aliberti S (2012) Measurement of retinal nerve fiber layer thickness, macular thickness, and foveal volume in amblyopic eyes using spectral-domain optical coherence tomography. JAAPOS 16(1): 86-88.
-
Wang BZ, Taranath D (2012) A comparison between the amblyopic eye and normal fellow eye ocular architecture in children with hyperopic anisometropic amblyopia. JAAPOS 16(5):428-430.
-
Pawar N, Maheshwari D, Ravindran M, Ramakrishnan R (2014) Retinal nerve fiber layer thickness in normal Indian pediatric population measured with optical coherence tomography. Indian J Ophthalmol 62(4): 412-418.
-
Elvan Yalcin, OzlemBalci (2014) Peripapillary retinal nerve fiber layer and foveal thickness in hypermetropic anisometropic amblyopia. Clinical Ophthalmology 8: 749-753.
-
Syunsuke Araki, Atsushi Miki, Yamashita T,Goto K, Haruishi K, et al(2014) A comparison between amblyopic and fellow eyes in unilateral amblyopia using spectral-domain optical coherence tomography. Clin Ophthalmol 8(7): 2199-2207.
-
Yassin SA, Al-Tamimi ER, Al-Hassan S (2015) Macular and retinal nerve fiber thickness in recovered and persistent amblyopia. Int Ophthalmol 35(6):833-842.
-
Li J, Ji P, Yu M (2015) Meta-analysis of retinal changes in unilateral amblyopia using optical coherence tomography. Eur J Ophthalmol 25:400-409.
-
Demircan S, Gokce G, Yuvaci I, Mustafa A, Burhan Başkan, et al (2015) The Assessment of Anterior and Posterior Ocular Structures in Hyperopic Anisometropic Amblyopia. Med Sci Monit 21:1181- 1188.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report