Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
Optic nerve hypoplasia (ONH) is a congenital anomaly characterized by a structurally small optic nerve head with reduced retinal ganglion cell axons. It is commonly recognized in childhood often associated with visual dysfunction or systemic abnormalities. However, rare cases may present in adulthood with normal visual acuity and atypical optic disc morphology that may create diagnostic uncertainty. We report a 26-year-old lady with a small optic disc and larger cup-to-disc ratio in one eye, mimicking Normal tension glaucoma (NTG). Despite normal intraocular pressure, visual field testing and optical coherence tomography revealed defects suggesting optic neuropathy. Neuroimaging confirmed focal hypoplasia of the retrobulbar optic nerve. This case highlights the diagnostic complexity of optic nerve hypoplasia and the importance of integrated evaluation to differentiate congenital anomalies from glaucoma.
Aung KH¹* and Aye MTH²
¹Department of Ophthalmology, University of Medicine 2, Yangon, Myanmar ²Department of Ophthalmology, University of Medicine 1, Yangon, Myanmar Retinal Nerve Fiber Layer Thinning
Abbreviations
ONH: Optic Nerve Hypoplasia; NTG: Normal Tension Glaucoma; BCVA: Best Corrected Visual Acuity; VCDR: Vertical Cup-To-Disc Ratio; RNFL: Retinal Nerve Fibre Layer; OCT: Optical Coherence Tomography.
Introduction
Optic nerve hypoplasia (ONH) is a congenital, non- progressive developmental anomaly of the optic nerve characterized by a reduced number of axons, resulting in a small optic disc and variable degrees of visual impairment [1]. ONH was first described in the 1910s, but its clinical significance became more widely recognized after increased reporting in the latter half of the 20th century [2]. It is now considered one of the most common congenital optic nerve anomalies worldwide with an estimated prevalence from 7 to 11 per 100,000 children [3]. The condition can be isolated or occur as part of systemic syndromes, particularly involving midline brain malformations and endocrinopathies [4, 5].
The characteristic features of ONH include a small optic disc, “double ring” sign and increased disc–macula distance to disc diameter (DM/DD) ratio, typically greater than 3 [6]. The condition is frequently diagnosed in infancy or childhood when visual loss, nystagmus, or strabismus prompts ophthalmologic evaluation. In contrast, mild or unilateral ONH may remain undetected until adulthood particularly when visual acuity is preserved. These cases are uncommon and may be discovered incidentally during routine eye examinations [7].
A particularly challenging scenario arises when ONH presents with an enlarged cup-to-disc ratio in a small disc as this can mimic glaucomatous optic neuropathy. NTG is often considered in young adults with normal intraocular pressures, optic disc cupping, and corresponding visual field defects [8]. Both conditions may present with retinal nerve fiber layer thinning on OCT, visual field loss, and optic disc changes that make differentiation difficult based on fundus examination alone [9, 10].
The absence of the classic double ring sign or borderline DM/DD ratios may further obscure diagnosis. Neuroimaging can be crucial to confirm optic nerve hypoplasia and exclude compressive lesions or other acquired optic neuropathies [11]. This differentiation is essential because glaucoma and ONH differ fundamentally in pathophysiology, management, and prognosis. ONH is a congenital anomaly and non- progressive whereas glaucoma is a progressive optic neuropathy that required life-long treatment to prevent visual loss [12].
Most of the previously published ONH cases were bilateral diseases with significant visual impairment. Unilateral ONH with normal central vision, optic disc asymmetry, and overlapping features with NTG is rare and diagnostically challenging. Here, we report such a case in a 26-year-old lady and discuss the critical role of detailed clinical evaluation and integrated imaging in establishing the diagnosis.
Case Presentation
A 26-year-old woman presented for a routine refraction. Her best corrected visual acuity (BCVA) was 6/6 in both eyes. Intraocular pressures were within normal limits. There was no history of visual problems. Anterior segment examination was unremarkable bilaterally.
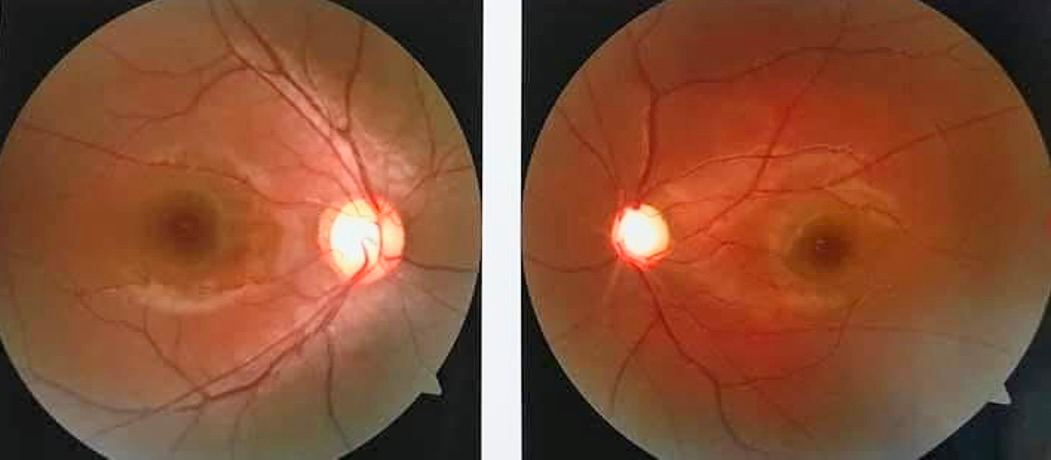
Posterior segment examination revealed an asymmetry in the optic disc. The left optic disc was smaller but vertical cup-to-disc ratio (VCDR) was larger 0.8 in the left eye and 0.6 in the right eye. Due to the smaller optic nerve head and increased VCDR, ONH was suspected. The characteristic signs like double-ring sign was not observed and the (DM/ DD) ratio was 3 which is at the borderline for ONH (Figure 1).
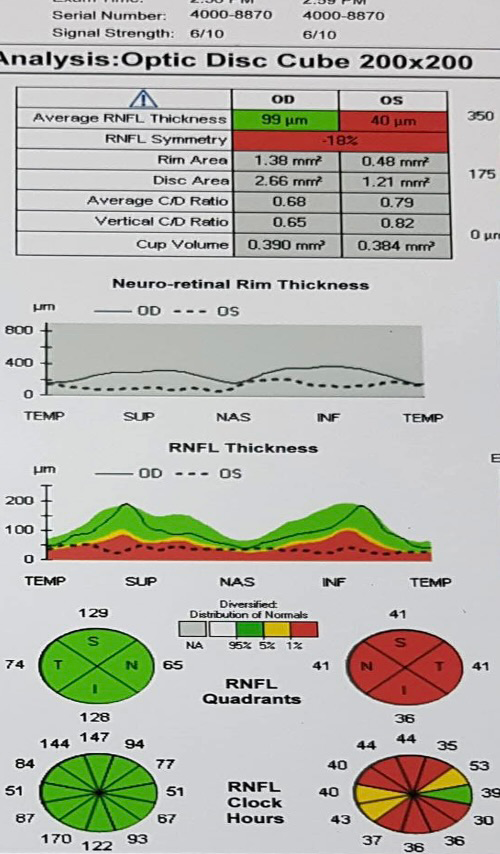
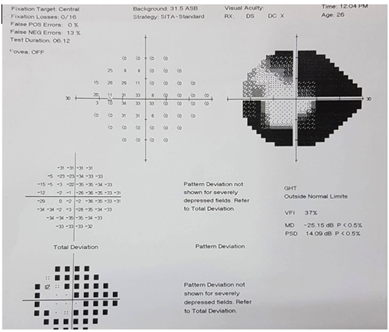
Then, differential diagnosis of ONH versus NTG was made. Humphrey visual field testing demonstrated a concentric visual field defect in the left eye and a normal field in the right (Figure 2). Optical coherence tomography (OCT) of the optic nerve head and retinal nerve fibre layer (RNFL) revealed generalized RNFL thinning in the left eye, with the right eye remaining within normal limits (Figure 3).
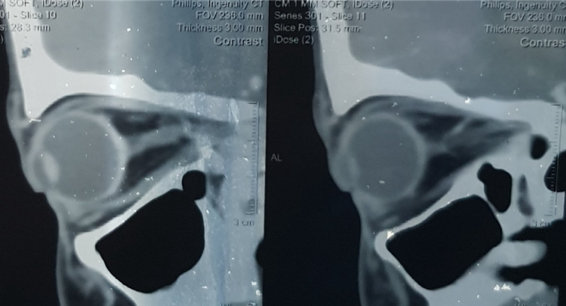
Neuroimaging with CT of the head and orbits was performed to exclude compressive optic neuropathy. The imaging showed focal atrophy or hypoplasia of the retrobulbar segment of the left optic nerve. Based on clinical and imaging findings, a diagnosis of left ONH was established (Figure 4).
Discussion
ONH is typically diagnosed in infancy or early childhood often in association with systemic or neurological abnormalities. In adults, particularly those with unilateral or mild disease, the presentation may be subtle, with incidental detection during routine examinations. This patient had preserved visual acuity, a large cup-to-disc ratio in the affected eye and borderline DM/DD ratio making the initial diagnosis challenging.
In glaucoma, increased cupping reflects progressive ganglion cell loss and excavation of the disc. In ONH, however, the optic disc is congenitally small and the cup may appear disproportionately large relative to the disc size that mimic glaucomatous cupping. This overlap can lead to misdiagnosis, especially in young adults with normal intraocular pressure and minimal symptoms [8, 9].
The absence of a double ring sign does not rule out ONH, as this sign may be subtle or absent in borderline cases. Visual field defects in ONH are variable, but concentric visual field defect is well documented and may mimic early glaucomatous field loss. OCT and neuroimaging are critical adjuncts in such scenarios. OCT helps identify RNFL thinning patterns, while neuroimaging confirms structural hypoplasia or atrophy of the optic nerve and excludes compressive lesions [10, 11].
This case is particularly notable because of its rare unilateral presentation, normal central vision, and overlapping features with NTG. The diagnostic challenge is intensified by the absence of classic ONH features that emphasize the need for high clinical suspicion and comprehensive evaluation.
Conclusion
Unilateral optic nerve hypoplasia with normal visual acuity is uncommon and can closely mimic glaucomatous optic neuropathy. This case demonstrates the importance of a structured diagnostic approach integrating clinical examination, optic disc evaluation, DM/DD ratio measurement, visual field testing, OCT analysis, and neuroimaging.
Recognizing the congenital nature of ONH allows for appropriate management, prognosis assessment, and avoidance of overtreatment.
Not all large cups indicate glaucoma congenital anomalies such as ONH should remain on the differential particularly in young adults with asymmetric optic disc.
References
-
Brodsky D (2013) Optic nerve hypoplasia: Clinical significance and association. J Neuroophthalmol 33(1): 1-7.
-
Hoyt AL (1976) Congenital anomalies of the optic disc. Am J Ophthalmol 81(5): 606-618.
-
Hellström J, Aronsson M (1999) Optic nerve hypoplasia prevalence and clinical spectrum. Acta Ophthalmol Scand 77(1): 78-82.
-
Borchert MA (2012) Reappraisal of the optic nerve hypoplasia syndrome. J Neuroophthalmol 32(1): 58-67.
-
Borchert MA, Garcia-Filion JE (2013) The syndrome of optic nerve hypoplasia. Curr Neurol Neurosci Rep 13(1): 1-9.
-
Frisén AM, Holmegaard L (1992) Visual field in optic nerve hypoplasia: The DM/DD ratio revisited. Acta Ophthalmol Scand 70(4): 495-500.
-
Morales ME (2015) Distinguishing optic nerve hypoplasia from glaucoma using OCT and clinical examination. Ophthalmology 122(5): 1138-1146.
-
Anderson DM (2014) Optic nerve anomalies mimicking glaucoma. Curr Opin Ophthalmol 25(2): 115-120.
-
Lee JK, Park KS (2020) Differentiating congenital optic nerve anomalies from glaucomatous cupping. Br J Ophthalmol 104(3): 325-331.
-
Yoo SH (2019) Optical coherence tomography findings in optic nerve hypoplasia and their diagnostic significance. Eye 33(4): 623-630.
-
Patel BA (2021) Neuroimaging in optic neuropathies: Clinical utility and diagnostic role. Surv Ophthalmol 66(6): 869-885.
-
Quigley H (2020) Glaucoma: Macro and microstructural considerations of optic nerve damage. Prog Retin Eye Res 76.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Large Angle Exotropia in a Child: A Case Report
- Refractive Status of Retinoblastoma Patients in a Tertiary Eye Care Centre of Bangladesh