Refractive Status of Retinoblastoma Patients in a Tertiary Eye Care Centre of Bangladesh
Purpose: To investigate the refractive status of patients with Retinoblastoma.Methods: A hospital-based cross-sectional study of 30 patients who had unilateral or bilateral retinoblastoma. A total 38 eyes underwent and cycloplegic refraction done with cyclopentolate eye drops in patients under 6 years of age. Statistical analysis was conducted using SPSS V16.Results: The age range was 4 months to 35 years. Most presenting age was 0 to 5 years age group and the most frequent type of refractive error was simple hyperopia (28.90%). Significant numbers of patients had astigmatism, with-the-rule astigmatism being more common (33.6%) than against-the-rule astigmatism. A small number of patients also showed oblique astigmatism.Conclusion: The frequency and nature of ametropia in children with unilateral and bilateral retinoblastoma were analyzed.highlighting the common refractive problems of astigmatism and hyperopia. Proper visual rehabilitation will play a vital role in ensuring a better future for these young people
Roy SR¹*, Biswas SK² and Baidya P³
¹Consultant and Head, Orbit, Oculoplasty and Ocular Oncology, Chittagong Eye Infirmary, Bangladesh ²Consultant and Head, Department of Cornea, Chittagong Eye Infirmary, Bangladesh ³Optometrist, Chittagong Eye Infirmary, Bangladesh Keywords: Retinoblastoma; Hyperopia; Myopia; Astigmatism
Abbreviations
IRB: Institutional Review Board; SH: Simple Hyperopia; SM: Simple Myopia; SMA: Simple Myopic Astigmatism; SHA: Simple Hyperopic Astigmatism; CMA: Compound Myopic Astigmatism; CHA: Compound Hyperopic Astigmatism; RPE: Retinal Pigment Epithelial; TTT: Transpupillary Thermotherapy.
Introduction
Retinoblastoma (Rb) is the commonest primary intraocular tumor of children with a world wide incidence of 1: 16,000 to 18,000 live birth and constitute 3% of childhood cancer [1, 2]. In USA incidence was reported as eleven per million children in under four years of age but a higher incidence was reported in India, Africa and native America [3]. Though this tumor is reported in literature from intrauterine life to older age, 66% are diagnosed before the age of two years and 95% are diagnosed before five years of age [3, 4]. These tumor may present unilaterally or bilaterally, be unifocal or multifocal. The location of tumor affects the vision of the children. The primary visual development of children continue from birth to six years of age and first four years being a critical period [5].
- Once retinoblastoma was a deadly tumor worldwide, but now a days the survival rate is improved to 99 to 91 % in higher and higher middle income countries.
- But in lower and lower middle income countries the survival rate is about 40 to 77% [6]. As overall survival and globe salvage rate is increased than previous due to improved medicine and technology. In such situation it is also important to know about the refractive status of Rb survivors. In literature search, there are paucity of article regarding this and we tried to give some input in this topic.
Methodology
It was a cross- sectional study done in Orbit Oculoplasty and Ocular oncology department of Chittagong Eye Infirmary, Bangladesh from October 2022 to September 2023.The Rb patients presented at that period were included in the study. Total 38 eyes of 30 patients were included. The study was approved by the local institutional review board (IRB) and conducted according to the principles of the 2013 revision of the Declaration of Helsinki. Rb patients, who underwent bilateral enucleation were excluded from the study.
Data regarding demography (age, sex), presenting symptoms, family history and treatment history were taken. Clinically all patients were examined by an ocular oncologist and data related to vision, refractive status, intraocular pressure and dilated fundus examination were taken. Patients under 6 years were examined under general anesthesia. In case of children (below 18 years) data was taken from parents.
Refraction Procedure
Objective refraction was performed to determine the total refractive status of the eye. After dry objective retinoscopy, refractive power was obtained, and finally, cycloplegia was carried out for all children. Cycloplegic refraction was performed under cyclopentolate eye drops. In the case of all children, cyclopentolate 1% was used three times, one drop in each eye, at an interval of 5 minutes. Cycloplegia was considered complete if the pupil diameter was 6mm or greater and the light reflex was absent. Cycloplegic refraction was carried out by streak retinoscopy in a semi-dark room at a distance of 50 cm. The magnitude of refractive error was determined by subtracting the working distance. Data Analysis We used Microsoft Excel version 2020 and SPSS (16.0 for Windows, SPSS Ine, Chicago, IL, USA). All data were entered into a Microsoft Excel database and converted to SPSS for analysis. According to the normality test, all parameters were nonparametric. A descriptive statistic was used to evaluate the frequency of the age group, gender, and refractive error. Frequency data were used to evaluate the percentages of age, gender, history, refractive error, diagnosis, and management.
Result
Age and Sex Distribution of the Study
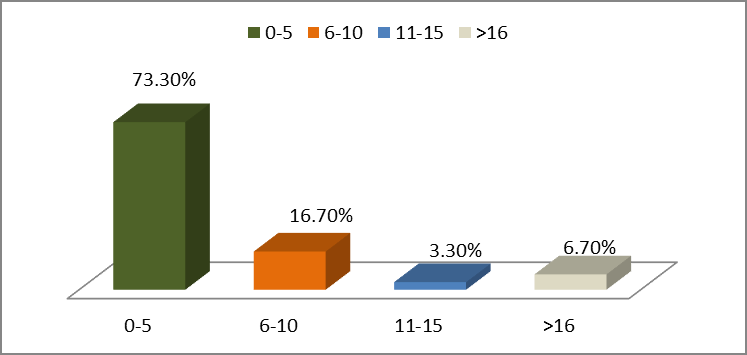
Out of 30 patients in the study, the highest age group was 0-5 years (n=22,73%) followed by 16.7%(n=5), 3.3%(n=1) and 6.7%(n=2) (Figure 1). The youngest one was 4 months old and oldest was 35 years old. About 47% were male and 53 % were female with a male: female was 1:1.1 (Table 1).
| Age in months | Number of the children (Total=22) |
|---|---|
| 0-12 | 18.1%(n=04) |
| 13-24 | 45.4%(n=10) |
| 25-36 | 13.6%(n=03) |
| 37-48 | 13.6%(n=03) |
| 49-60 | 09%(n=02) |
Table 1: Age distribution in months of 0 to 5 years aged children.
Chief Complaints of the Study
The main complaints of patients were white pupillary reflex in 22 individuals (73.3%). Others were decreased vision, redness, watering. One patient came for a routine examination due to a family history (Table 2).
| Presenting symptoms | Number of patients |
|---|---|
| White pupillary reflex | 73.3%(n=22) |
| Watering and redness | 23.3%(n=07) |
| Visual problem | 30.0%(n=09) |
| Regular check up | 3.30%(n=01) |
Table 2: ** Presenting symptoms of the responded.
Note: More than one symptom was present in a single patient. Table 2: Presenting symptoms of the responded.
Types of Refractive Status of the Patients
Refractive error diagnosed on basis of cycloplegic refraction. Most frequent type of refractive error was simple hyperopia in 28.90%(n=11) patients followed by CMA 18.40%(n=7)) (Figure 2).
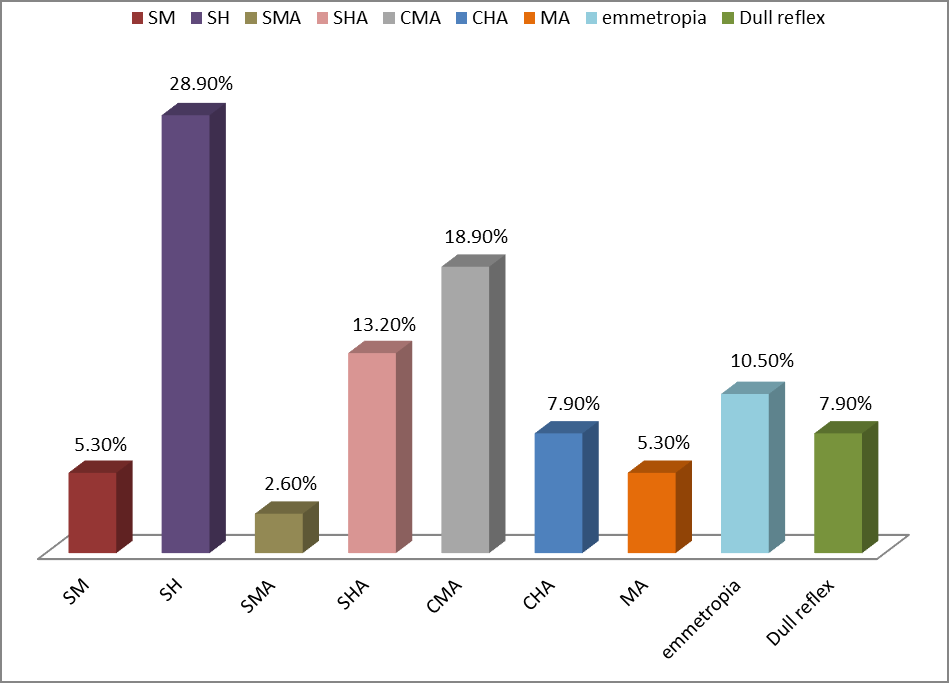
Note: SH=simple hyperopia, SM=simple myopia, SMA= simple myopic astigmatism, SHA= simple hyperopic astigmatism, CMA=Compound myopic astigmatism, CHA= Compound hyperopic astigmatism. Figure 2: Percentage of refractive error in the study.
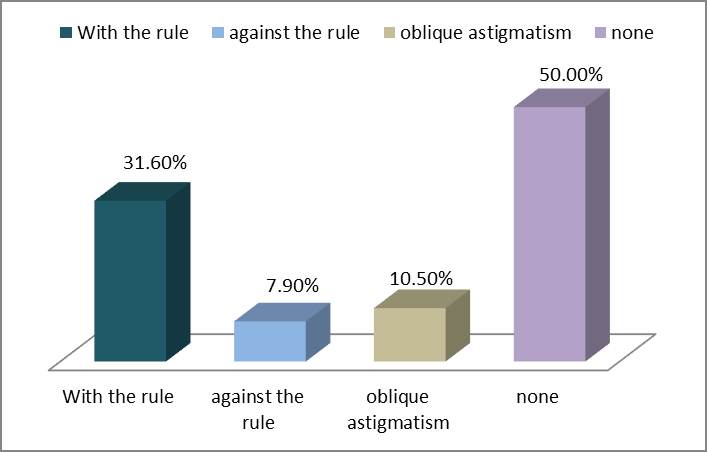
Distribution of pattern of astigmatism: The study found, most patients (n=19,50%) did not have any astigmatism and about 32%(n=12) had with the rule astigmatism (Figure 3).
| IIRC (n=30) | Number of patients |
|---|---|
| Group A | 03.3%(n=01) |
| Group B | 36%(n=11) |
| Group C | 30%(n=09) |
| Group D | 26.7%(n=08) |
| Group E | 70%(n=21) |
Table 3: ** Grouping of tumors according to International Intraocular Classification of Retinoblastoma.
Note: In bilateral cases both eyes diagnosis was included. Table 3: Grouping of tumors according to International Intraocular Classification of Retinoblastoma.
Management of the patients: About 43%(n=13) received a combination of chemotherapy and focal therapy (laser, cryo therapy), 10% (n=03) received both systemic, intravitreal chemotherapy and focal therapy, 63.3%(n=19) received a combined treatment regimen of chemotherapy, laser, and enucleation and 33.3%(n=10) patients underwent solely enucleation.
Family history of the study: Only 4 (13%) cases had family history of retinoblastoma. In two cases father had retinoblastoma and other cases sibling were affected.
Discussion
Each year about 9000 new cases of retinoblastoma is added to the existing list of retinoblastoma and about two- third are from Asia [7]. Due to improvement of treatment facilities and awareness the survival rate of retinoblastoma is increasing. In India the pooled 5 years overall survival rate is 78.7% [8]. One single center study from Bangladesh showed the overall survival rate in primary enucleated patients is 68% [6]. To live a better normal life all the Rb survivor need visual and psychosocial rehabilitation. The visual outcome depends on early presentation, location of tumor, treatment modalities and acceptance of treatment by parents. In case of macular tumor, patient’s central vision is diminished but with proper refraction eccentric vision may improve. Peripheral tumor usually presents at delay and usually presents with huge tumor which may lead to sacrifice the globe. Regarding treatment modalities, it depends on which types of treatment is necessary to treat the tumor ad availability of treatment modalities. Intravenous and intra- arterial chemotherapy quickly reduce exudative retinal detachment and improve vision. Sometimes anticancer medication causes retinal pigment epithelial (RPE) toxicity and change of other retinal cells causing long term effect on vision. One study demonstrated 100% central RPE changes near cell nucleus, RPE proliferation in about 18% cases formation of drusen in 47% cases in a series of post chemotherapy patients [9]. Radiotherapy also causes delayed effect in vision. Transpupillary thermotherapy (TTT) is better than argon laser but TTT is not available in all Rb centers specially lower and lower middle- income countries. The literature stated that, extensive local therapy (Cryo and Laser therapy) may affect the normal development of the eye [10]. The visual and good treatment outcome mainly depends on time of occurrence of tumor; early presentation; knowledge and understanding of parents.
A child after birth gradually meets to visual maturation up to late teen. The primary visual development occurs from birth to six years and first 4 years are thought to be critical period. There are some key milestones like development of binocular vision by four months, color vision by five months, depth perception by five to eight months and refined visual – motor coordination with acuity of vision later on. So if there is an interruption in any period of visual development, the vision will be affected.
According to different studies the main presenting symptom is white pupillary reflex and about 73% of the study children had the same presentation. Our 70% children were diagnosed as group E retinoblastoma followed by group B. Regarding treatment about 67% patients received chemotherapy and focal treatment (except solely enucleation).
In the current study the most affected age group was 0 to 5 years and among them about 45% were between 13 to 24 months old. Two different studies related to refraction with Rb children stated the age range of 3.8 to 18 years and 1 month to 72 months respectively [11, 12]. In our study, the age range was 4 months to 35 years. Both studies showed little bit female predominance like ours.
Different types of refractive error were found along with emmetropia and dull reflex. Most children (28.9%) had simple hyperopia. One study from Russia also showed increased frequency of hyperopia over 3 diopters in more than 25% cases of retinoblastoma patients [13]. The number of myopias in the similar study was 3.3% and in the present study it was 5.3%. It may be due to increase axial length. Eyes treated with laser for several time supposed to had greater refractive changes overtime [14]. Extensive focal therapies in retinoblastoma hamper the normal development of the anterior segment of eye.
Children who have refractive defects, including anisometropia and hyperopia, are at risk for developing amblyopia [15]. One large study with 3- to 5-year-old subjects (n = 3,869) found that unilateral amblyopia is present in 12.9% of subjects with hyperopia (3–4 D) and 33.1% of subjects with anisometropia (1-2 D) [16].
In this study, astigmatism was present in a significant proportion of patients, with a higher prevalence of with-the- rule astigmatism compared to against-the-rule astigmatism. Oblique astigmatism was also observed in a subset of patients. Unequal refraction at different meridians of results in astigmatism and may divided into corneal, lenticular and retinal astigmatism. Among them corneal astigmatism is more prevalent [17]. Study by Abdallah HA, et al. [12] and Saakyan SV, et al. [13] showed Rb children had more astigmatism in eyes with tumor than fellow and control eye. In tumor filled eye the reason for more astigmatism may due to location of tumor causing retinal astigmatism and excessive focal therapy causing corneal astigmatism. In 2018, Consejo et al. proved that astigmatism is highly related to corneal and scleral asymmetries by using corneoscleral topographer [18].
This study’s focus on refractive status and its sequelae adds to the corpus of knowledge by providing information on the potential ocular problems and visual outcomes of retinoblastoma patients post-treatment. The similarity of our findings with those of previous studies highlights the general necessity of continuous ocular monitoring for these patients.
Moreover, anisometropia and astigmatism patterns identified in this study align with other investigations, emphasizing the necessity of addressing these optical challenges to optimize visual rehabilitation. The presence of hyperopia and myopia also warrants careful management to ensure the best possible vision outcomes.
Limitation
This study was done who were attending the oncology department and was in different stages of treatment which may affect the result of refraction. Tumor size, tumor growth pattern, visual acuity, and clinical changes were not evaluated.
Conclusion
Hyperopia emerged as a common refractive issue, with astigmatism patterns providing valuable insights in retinoblastoma patients. Sustained ocular monitoring in these patients, especially addressing anisometropia and optimizing visual rehabilitation is needed for a brighter future.
Conflict of Interest
All authors declared no conflict of interest. References
1. Roy SR, Kaliki S (2021) Retinoblastoma: A Major Review. Mymensingh Med J 30(3): 881-895.
2. Rodriguez-Galindo C, Orbach DB, Veen DV (2015) Retinoblastoma. Pediatr Clin North Am 62(1): 201-223.
3. Gupta N, Pandey A, Dimri K, Prinja S (2020) Epidemiological profile of retinoblastoma in North India: Implications for primary care and family physicians. J Family Med Prim Care 9(6): 2843-2848.
4. Salim A, Wiknjosastro GH, Danukusumo D, Barnas B, Zalud I (1998) Fetal retinoblastoma. J Ultrasound Med
17: 717-720.
5. Zimmermann A, Carvalho KMM, Atihe C, Zimmermann SMV, Ribeiro VLM (2019) Visual development in children aged 0 to 6 years. Arq Bras Oftalmol 82(3): 173-175.
6. Roy S, Anjum R, Biswas S (2024) A 12-year analysis of presentation, histopathological features, high- risk factors, and survival in retinoblastoma patients undergoing primary enucleation at a tertiary eye care center in Bangladesh. Tumor Discovery 3: 4336.
7. Zhang Y, Wang Y, Zhi T, Jin M, Huang D, et al. (2023) Clinical characteristics, treatment and prognosis of infants with retinoblastoma: A multicenter, 10-year retrospective analysis. BMC Pediatr 23(1): 229.
8. Das S, Mahajan A, Das S, Honavar SG (2025) Survival outcomes and globe salvage rates of retinoblastoma in India - A systematic review. Indian J Ophthalmol 73(8): 1116-1123.
9. Das D, Rehman O, Bhattacharjee K, Barman MJ, Bhattacharjee H, et al. (2024) Post-chemotherapy changes in retinal pigment epithelium in retinoblastoma eyes. Can J Ophthalmol 59(6): e758-e762.
10. Whitmore WG, Curtin BJ, Fox D (1993) The modulation of ocular growth in rabbits with peripheral retinal ablation. Ophthalmology 100(7): 1003-1008.
11. Villegas VM, Wu SC, Murray TG, Cavuoto KM, Capo H,
et al. (2019) Prevalence of refractive errors in children with retinoblastoma. Clin Ophthalmol 13: 431-435.
12. Abdallah HA, Hamdi MM, Abdel Rahman SH, Mohamed NS, Abdel Aziz NAS (2025) The Refractive Parameters of Treated Retinoblastoma Eyes. Ocul Oncol Pathol 11: 1.
13. Saakyan SV, Tsygankov AI, Tadevosyan SS, Makarova AA, Kogoleva LV, et al. (2020) Refractive Errors in Children with Retinoblastoma. Ophthalmology in Russia 17(1): 76-80.
14. Hwang ES, Kassem IS, Allozi R, Kravets S, AlKirwi KY, et al. (2022) Association between myopia progression and quantity of laser treatment for retinopathy of prematurity. PLoS One 17(12): e0279898.
15. Villegas VM, Wu SC, Murray TG, Cavuoto KM, Capo H, et al. (2019) Prevalence of refractive errors in children with retinoblastoma. Clin Ophthalmol 13: 431-435.
16. Pascual M, Huang J, Maguire MG, Kulp MT, Quinn GE, et al. (2014) Risk Factors for Amblyopia in the Vision in Preschoolers Study. Ophthalmology 121(3): 622-629.
17. Abrams D (1993) Duke-Elder’s practice of refraction. In: 10th (Edn.), London: Churchill Livingstone, pp: 6.
18. Consejo A, Rozema JJ (2018) Scleral shape and its correlations with corneal astigmatism. Cornea 37(8): 1047-1052.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report