Large Angle Exotropia in a Child: A Case Report
Purpose: To report a case of large angle exotropia in a child.Case Report: A 13 years old male child presented with outward deviation of left eye since 3 years of age. No history ofprematurity, low birth weight and diplopia. His visual acuity was 6/9 in right eye and 6/24 in left eye. On orthoptic evaluation,there was manifest exotropia in left eye with poor control on cover-uncover test. On prism cover test, there was exotropia of 45Prism diopter (PD) in up gaze, primary gaze, down gaze and 40 PD in lateral gaze for distance and exotropia of 45 PD for nearin both eyes. Both binocular single vision (BSV) and stereopsis were absent. He underwent lateral rectus recession of 9mmand medial rectus resection of 6mm in left eye.Conclusion: Post operatively, motor alignment was satisfactory but BSV and stereopsis did not return.
Marazul Islam Bhuiyan¹, Umme Salma Akbar², Shally Biswas³ and Muhammed Raihan Uddin⁴
¹Consultant and Department of Paediatric Ophthalmology, Chittagong Eye Infirmary and Training Complex, Bangladesh ²Consultant, Chittagong Eye Infirmary and Training Complex, Bangladesh ³Associate Consultant, Chittagong Eye Infirmary and Training Complex, Bangladesh ⁴Senior Assistant Surgeon, Chittagong Eye Infirmary and Training Complex, Bangladesh
Abrreviations
PD: Prism Diopter; BSV: Binocular Single Vision; EOM: Extra- Ocular Motility; LR: lateral Rectus; MR: Medial Rectus.
Case Report
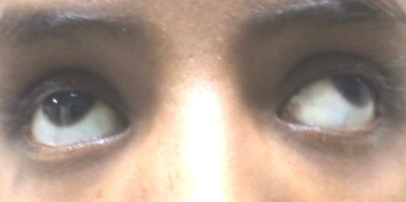
A 13 years old boy (Figure 1) presented with outward deviation of left eye since 3 years of age. No history of prematurity, low birth weight and diplopia. On examination, he had an uncorrected visual acuity of 6/6 in right eye and 6/24 in left eye. Vision in left eye did not improve with pinhole and refraction [1].
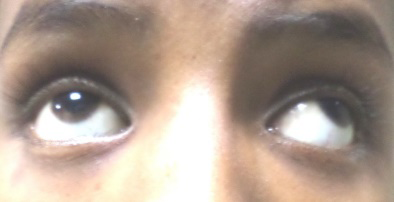
On orthoptic evaluation, there was no anomalous head posture, Hirschberg’s reflex- 25 degree with right eye fixation preference. Ocular motility was full in all gazes (Figure 2).
Cover-uncover test revealed manifest left exotropia with poor control.







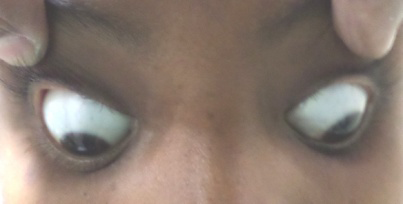
On prism cover test, there was exotropia of 45 PD in up-gaze, primary gaze, downgaze and 40 PD in side gaze for distance and exotropia 45 PD for near in both eyes (Figure 3).
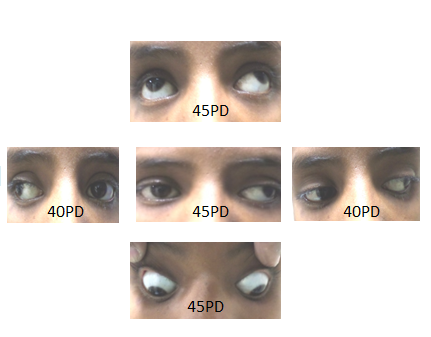
Sensory evaluation showed: left eye suppression on Worth four – dot test and no stereopsis. The rest of the anterior and posterior segment evaluation was unremarkable. He underwent lateral rectus recession of 9mm and medial rectus resection of 6mm in left eye. Post operatively, motor alignment was satisfactory (Figure 4) but BSV and stereopsis did not return.

Discussion
Exodeviation occur less frequently than esodeviation in a ratio of 1:3 and are more common in females. Hereditary plays a significant role in exodeviations. Exotropia developing if one sibling from a multiple birth is affected is increased by 17-fold. No such association is found for siblings from separate births.
Exodeviation is characterized by visual axes that form a divergent angle. It usually begins as an exophoria. Exophoria may later progress to intermittent exotropia and finally to constant exotropia. Burian’s classification of exodeviation are: • Basic Exodeviation: Distance deviation is within 10 PD of near deviation. These patients have a normal accommodative convergence/accommodation (AC/A) ratio. • Convergence Insufficiency: Near deviation measures at least 10PD more than distance deviation. Patients have either low AC/A ratio or fusional convergence insufficiency. • Divergence Excess: True divergence excess- Exodeviation measures at least 10PD more at distance than at near. The AC/A ratio is normal. Measurements do not increase with +3 D lenses nor with prolong occlusion. • Pseudo Divergence Excess: Exodeviation measures at least 10PD more at distance than at near which increases with +3 D lenses and prolong occlusion.
Non-surgical management is indicated in patients with
excellent control as measured by normal distance stereoacuity and in young children who are at risk of developing mono- fixational esotropia from persistent surgical overcorrection. In children, nonsurgical techniques such as minus lenses and base in prisms can prevent or reverse early sensory anomalies by maintaining the potential for equal vision in each eye and preserving binocular fusional status.
Indications for surgery include poor control or deterioration of control of exotropia, deterioration in stereoacuity, development of suppression, severe asthenopia and diplopia. Bilateral lateral rectus (LR) recessions are preferred for patients with divergence excess. The recess- resect procedures involve lateral rectus (LR) recession and medial rectus (MR) resection ideal for basic exotropia and convergence insufficiency. Large angle exotropia of more than 50 PD should probably be managed with bilateral LR recessions combined with resection of one or both MR muscles.
Conclusion
Regular follow-up with vision therapy is necessary to determine progress of vision, BSV and stereoacuity.
References
-
Rosenbaum AL, Santiago A (2000) Clinical strabismus management principles and surgical techniques. American Journal of Ophthalmology 129: 1.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Refractive Status of Retinoblastoma Patients in a Tertiary Eye Care Centre of Bangladesh