Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
Objective: To present two cases of angioid streaks complicated with macular neovascularization (MNV) and tracking their clinical courses and treatment outcome over 2 years. Methods: Case reports of two patients of angioid streaks complicated with MNV. Best corrected visual acuity (BCVA) using snellen chart ,ophthalmological examination, color photographs, fundus fluorescence angiography (FFA) and optical coherence tomography (OCT) were used to follow the clinical courses and to assess the outcome of the treatment. Results: Two cases (4 eyes) were managed mainly with intravitreal anti vascular endothelial growth factor injections (anti VEGF) for subfoveal macular neovascularization (MNV), and in one eye for juxtrapapillary choroidal neovascularization (CNVM).The follow-up period ranged from 24 to 36 months. At the final visit, visual acuity remained around 6/60, despite of development of submacular scar in both cases. Conclusion: Angioid streaks are frequently complicated by recurrent macular neovascularization, resulting in a poor visual prognosis even with regular treatment. We adopted pro re nata (PRN) regimen of intravitreal anti‑VEGF following an initial loading phase to maintain visual function. This approach was well tolerated and remained effective over a period of two to three years.
Abbreviations
MNV: Macular Neovascularization; BCVA: Best Corrected Visual Acuity; FFA: Fundus Fluorescence Angiography; OCT: Optical Coherence Tomography; VEGF: Vascular Endothelial Growth Factor Injections; CNVM: Choroidal Neovascularization; PRN: Pro Re Nata; AS: Angioid Streaks; GA: Geographic Atrophy; NDPR: Non‑Proliferative Diabetic Retinopathy; RPE: Retinal Pigment Epithelium; PXE: Pseudoxanthoma elasticum; OCT-A: Optical Coherence Tomography Angiography; PDT: Photodynamic Therapy; VA: Visual Acuity.
Introduction
Angioid streaks (AS) are linear breaks of a calcified Bruch membrane, typically of reddish to brownish-gray color and ragged borders of variable width [1, 2, 3]. They are often bilateral and located in the posterior pole, typically radiate from the peripapillary region [1, 4, 5]. Angioid streaks are due to pathological changes in Bruch’s membrane, which were confirmed histologically in the late 1930s. In some diseases, including pseudoxanthoma elasticum, Ehlers-Danlos syndrome, Paget’s disease, and various blood dyscrasias, such as sickle cell disease, thalassaemia. Bruch’s membrane becomes calcified and brittle with subsequent development of cracks [6, 7]. New blood vessels may proliferate in the cracks, generating choroidal neovascularization (CNVM), with subsequent serous and hemorrhagic detachment of the fovea (the most serious complication), choroidal rupture, or foveal involvement by a streak with damage to the retinal pigment epithelium and choriocapillaris [8].
Although many individuals with AS remain asymptomatic, AS may become symptomatic due to hemorrhages, CNVM and geographic atrophy (GA) that may complicate their course, leading to progressive central vision loss [9]. Historically, treatment options have been limited; however, over the last two decades, therapeutic strategies have undergone significant evolution, particularly with the introduction of anti-VEGF agents, which play a central role in the treatment of AS-related CNVM. Emerging treatments, including gene therapy, enzyme replacement and drug delivery systems, represent promising strategies not only for preventing complications of AS but also to hinder its onset and progression [10].
In these case reports, we followed the long term course of this condition, its complications and the treatment responses.
Case Studies
Case Report 1
43 years old male presented with a history of gradual loss of vision over 1 month in the right eye. Visual acuity was 6/36 right eye and 6/9 left eye. The Patient had a known diagnosis of thalassemia and had undergone multiple blood transfusions. He had no other systemic diseases and no history of trauma. He had no signs of Psuedoxanthoma elasticum on skin.
Both eyes anterior segments were unremarkable with normal intraocular pressure of 10 mmHg .Dilated fundus examination revealed an active subfoveal MNV with subretinal hemorrhage, connected to the area of angioid streaks emerging from optic disc on right eye. The left eye showed no evidence of MNV. Diagnosis was further confirmed with FFA and OCT which demonstrated hyperfluorescence streaks arising from optic disc, a classic subfoveal hyper- fluorescencent leak of MNV and the presence of subretinal hyperreflective material with subretinal fluid (SRF) respectively (Figure 1A & 1B).
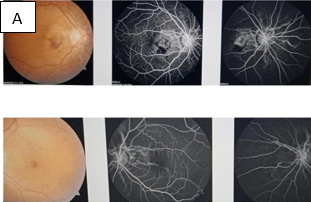
Figure 1A: Right active subretinal hemorrhage connected to area of angioid streaks.FFA showed classic subfoveal MNV with leakage.
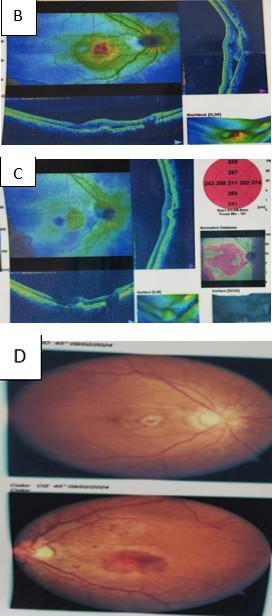
Figure 1B: Right sub retinal hyper reflectivity with SRF.
The patient was treated with 6, monthly doses of intravitreal ranibizumab injection (0.5mg/0.05ml) in the right eye. After 6 months, vision improved to 6/9 (Figure 1C).
Patient was regular to follow up for next 2 months after that he missed.
Figure 1C: Resolved SRF.
9 months later, the patient returned with complaints of sudden blurry vision in the left eye for 10 days. Visual acuity on right eye was 6/24 and 1/60 on left eye. Dilated fundus examination showed an active subfoveal MNV with
Figure 1D: Active subfoveal MNV of left eye.
subretinal hemorrhage in the left eye, confirmed by OCT which displays subretinal fluid. The right eye also showed signs of MNV reactivation (Figure 1D & 1E).
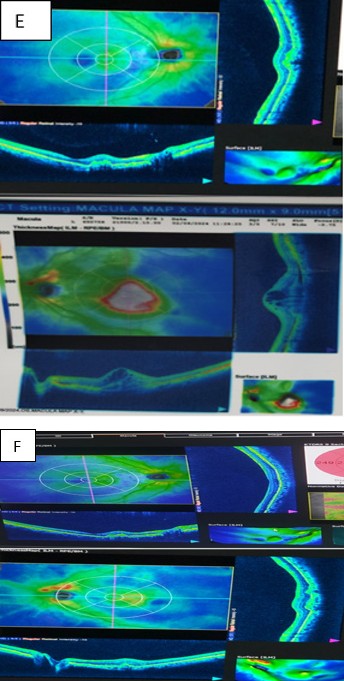
Figure 1E: Active subfoveal MNV of left eye.
The patient underwent monthly doses of 3 intravitreal ranibizumab on right eye and 6 doses on left eye. After 6 months, visual acuity improved to 6/9 in the right eye and 6/36 in the left eye. Clinical evaluation and OCT of the right eye showed regression of MNV but the left eye still had residual subretinal fluid. The patient was advised to continue the injection for the left eye but missed follow-up again.
6 months later he presented again with metamorphopsia and decreased vision in the left eye. This time vision was
6/18 in the right eye and 6/60 on left eye. OCT of both eyes showed the presence of subretinal fluid. The patient was advised to restart intravitreal antiVEGF therapy in both eyes. Although brolucizumab were recommended, due to financial constraints he opted for bevacizumab.
After 6 doses of bevacizumab, (1.25mg/0.05ml) in both eyes, visual acuity was 6/18 in the right eye and 6/24 in the left eye. MNV healed with leaving a subfoveal scar, prominently in left eye (Figure 1F).
Figure 1F: Healed MNV in both eyes.
Case Report 2
A 38‑year‑old male presented with a 3‑month history of metamorphopsia in right eye. He had previously received six doses of intravitreal bevacizumab in the right eye at another center, 6 months earlier. His visual acuity was 3/60 in the right eye and 6/6 in the left eye. The patient was diabetic and hypertensive.Examination of the neck and axilla revealed coalescent yellow papules and skin thickening with a peau d’orange appearance, suggestive of pseudoxanthoma elasticum. There was no history of trauma.
Both eyes anterior segments were unremarkable with normal intraocular pressure of 12 mmHg. Dilated fundus examination of the right eye showed blurring and irregular margins of the optic nerve head due to optic disc drusen, with faint angioid streaks emerging from the disc margin. The macula demonstrated a macular neovascular membrane with a small hemorrhagic spot. The background retina showed multiple microaneurysms and dot‑blot hemorrhages, consistent with non‑proliferative diabetic retinopathy (NPDR) (Figure 2A).
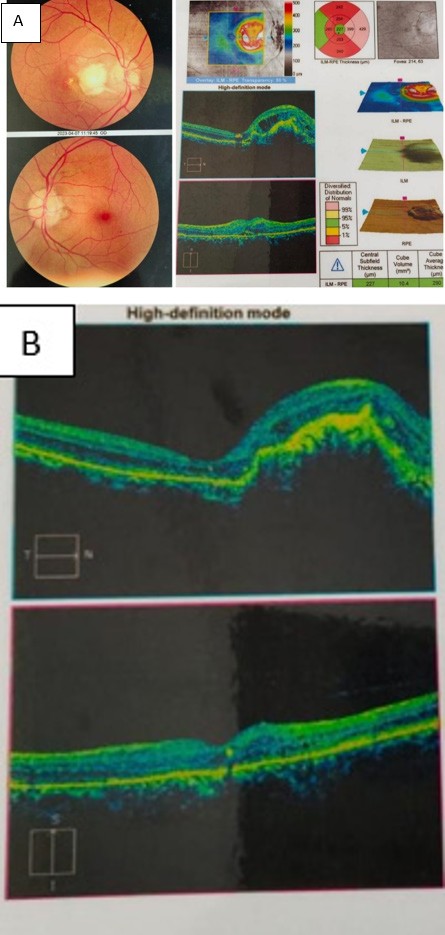
Figure 2A: Right active MNV.OCT showed sub retinal fluid.
In the left eye, blurred and irregular optic disc margins due to optic disc drusen was present with angioid streaks starting from the disc margin but no associated MNV. Back ground retina had multiple microanuerysm and dot blot haemorrhage due to NPDR (Figure 2A). To confirm the findings, B‑scan ultrasonography (Figure 2F) and macular OCT were performed for both eyes. The right eye OCT showed
Figure 2B: Status after 6 doses of brolucizumab on right eye.
prominent subretinal fluid (Figure 2A). So, the patient was advised to start intravitreal brolucizumab, (6mg/0.05ml) monthly doses in the right eye. After 6 doses, the visual acuity improved to 6/60, and resolution of subretinal fluid is seen (Figure 2B). For next 3 months patient was regular to follow-up with no recurrence of subretinal fluid. Then, he missed the follow up.
6 months later, the patient returned with complaints of dimness of vision in the left eye for 1 month. Visual acuity was 6/9 in the left eye and 6/60 in the right eye. Dilated fundus examination revealed an MNV scar in the right eye and a juxtapapillary CNVM in the left eye. OCT of both eyes showed the presence of subretinal fluid (Figure 2C). The patient was advised to restart intravitreal anti‑VEGF therapy in both eyes. This time, he chose bevacizumab due to affordability.
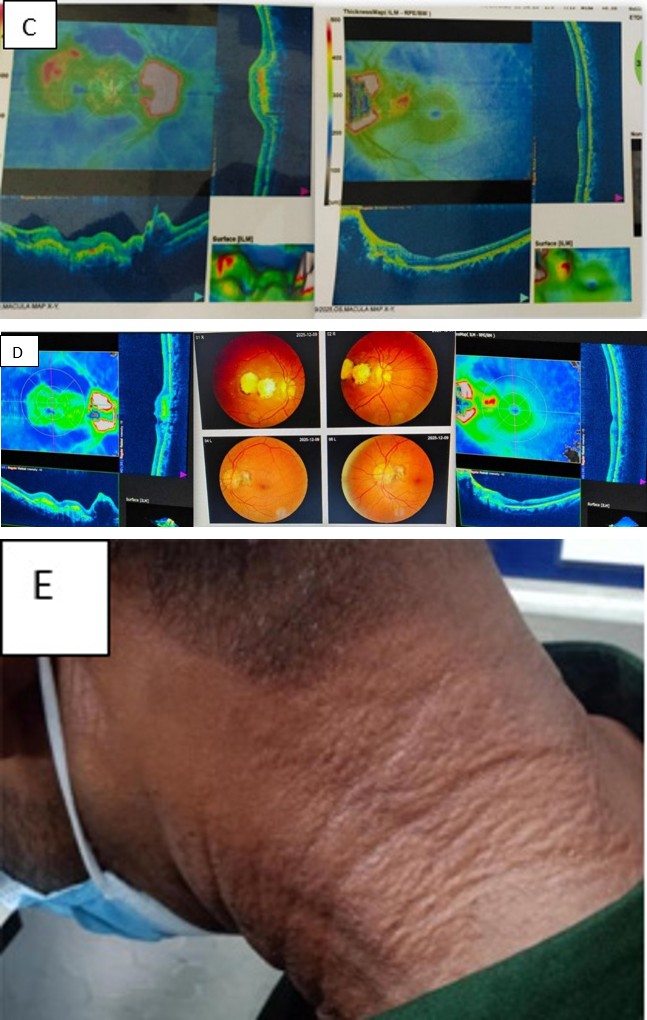
Figure 2C: Recurrence of SRF in both eyes.
After 6 doses, the visual acuity remained 6/60 in the right eye and improved to 6/6 in the left eye. He came after 3 months for follow‑up, the right eye showed a fibrotic macular scar, while the left eye had an inactive CNVM (Figure 2D & 2E). Throughout this period, the background diabetic retinopathy remained stable.
Figure 2D: Macular scar in right eye.
Figure 2E: Psuedoxanthoma elasticum on neck skin.
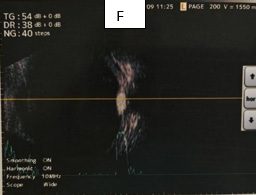
Figure 2F: Left B-scan USG shows optic disc drusen.
Discussion
Angioid streaks are distinct crack-like line can be observed during fundoscopy that represent a dehiscence in the Bruch membrane, a thin connective tissue layer that separate the retinal pigment epithelium (RPE), the cellular mono layered barrier directly adjacent to the photoreceptors, from the underlying choriocapillaris. A mottled, yellowish speckling of the RPE, commonly referred to as “peau d’orange” (orange peel appearance) or “leopard skin,” is also a feature frequently associated with AS [11].
Pseudoxanthoma elasticum (PXE) is a genetic metabolic disease with autosomal recessive inheritance caused by mutations in the ABCC6 gene [12]. This disease is characterized by a progressive mineralization and degeneration of components within the extracellular matrix, affecting multiple organ systems, including the skin, eyes, and cardiovascular system. PXE typically causes skin changes, due to dermal calcifications, that manifests as a “cobblestone” or “chicken skin” appearance. Its association is with AS, also known as Grönblad-Strandberg syndrome [11].
Careful fundoscopy usually reveals the presence of AS. When clinical suspicion persists fundus color photography and fundus autofluorescence are useful adjuncts. Fundus fluorescein angiography and optical coherence tomography angiography (OCT-A) are usually performed to rule out extent of MNV. Though due to unavailability of OCT-A at our centre we used OCT.
The advent of anti-VEGF therapies has dramatically improved the management of MNV in AS. Drugs such as ranibizumab, aflibercept, and off-label bevacizumab inhibit VEGF, a key mediator in angiogenesis and vascular permeability [13]. Numerous case reports and small series have demonstrated that these agents can stabilize and even improve visual acuity in patients with AS-related CNV [14]. Before the anti-VEGF era, Photodynamic Therapy (PDT) with verteporfin was commonly used to treat CNV. Though initially promising, PDT’s efficacy was modest and often short-lived [9].
Bhatnagar reported short-term improvements or stabilization of visual acuity (VA) with bevacizumab in PXE patients with AS-associated CNV; however, 50% of patients required multiple injections, with a mean of 1.8 injections over just 6 months [14].
We also have observed immediate improvement of vision and stable anatomical outcome after intravitreal bavacizumab in both cases.
In a separate study, Finger RP, et al. [14] evaluated bevacizumab in 16 eyes with CNV secondary to PXE over a 28-month period, observing both functional and anatomical improvements, with an average of 6.5 injections during that time [14].
The PIXEL study demonstrated VA stabilization over 4 years with a lower average of 4.1 injections of ranibizumab 0.5 mg, suggesting a reduced treatment burden compared to the previous study. Moreover, in the PIXEL study the percentage of eyes affected by CNV decreased by more than half over 4 years, while the occurrence of retinal hemorrhage dropped to nearly one-quarter within 2 years and then remained stable through the 4-year follow-up [15].
In first case, we have seen that, after initial doses of 6 injection ranibizumab patient’s vision was stable for at least 2 months with no recurrence. But due to long 9 months of missed follow up, we could not confirm the exact time of recurrence and sustainability of ranibizumab.
Over a 36 -month period this patient received total 15 intravitreal injections in the right eye and 12 in the left eye. Each episodes of recurrent SRF was accompanied by a measurable decline in visual acuity, prompting continuation of anti‑VEGF therapy on a PRN basis. Resolution of SRF produced meaningful visual improvement, though recurrence could not be prevented. This clinical course is a noteworthy feature of MNV associated with angioid streaks (AS), reflecting the underlying fragility of Bruch’s membrane. In this case both ranibizumab and bevacizumab effectively reduced SRF with a good safety profile.
In our second case along with angioid streak patient had a distinguished feature of optic disc drusen in both eyes. This patient was treated previously with 6 doses of injection bavacizumab in another centre. At presentation to our clinic, he had a marked decline in visual acuity, so we chose newer generation injection brolucizumab. Smaller molecules, such as brolucizumab, have exhibited superior target-tissue penetration, resulting in longer durability, better efficacy, and reduced systemic exposure. These molecular properties of brolucizumab can be advantageous in a condition such as AS which has thickened and calcified Bruch’s membrane and an abnormal retinal pigment epithelium [16]. We have found one single case report of a case with MNV secondary to AS that was treated successfully with intravitreal brolucizumab [16].
In our patient, six injections of brolucizumab produced substantial reduction of SRF at least for next 3 months. Although long‑term stability remained elusive due to repeated missed follow-up.
In both cases bilateral involvement happened within one year of the first eye being affected. Ultimately, one eye in each patient progressed to macular scarring.
Across both cases, multiple anti‑VEGF injections did not yield the degree of visual improvement typically observed in other etiologies of MNV.
Several recurrence of MNV on the same site or other site makes the treatment challenging. Some emerging strategies including gene therapy, proton pump inhibitor modulation and sustained drug delivery represent promising avenues that may target the underlying disease mechanism [9].
Conclusion
The clinical course and long‑term treatment outcomes of angioid streaks are highly variable and often unpredictable. Extended monitoring and strong patient adherence are essential for achieving the best possible results. Although anti‑VEGF agents remain the cornerstone of therapy for AS‑related MNV, challenges persist regarding treatment sustainability and prevention of recurrence. Given the rarity of this condition and its frequent systemic associations, early diagnosis and management of complication is crucial. Continued research and exploration of emerging therapeutic modalities are needed to improve long‑term visual prognosis in these patients.
Disclosure
The authors report no conflicts of interest in this work.
References
-
Gliem M, Finger RP, Fimmers R, Brinkmann CK, Holz FG, et al. (2013) Treatment of choroidal neovascularization due to angioid streaks: a comprehensive review. Retina 33(7): 1300-1314.
-
Georgalas I, Tservakis I, Papaconstaninou D, Kardara M, Koutsandrea C, et al. (2011) _Pseudoxanthoma elasticum_, ocular manifestations, complications and treatment. Clin Exp Optom 94(2): 169-180.
-
Ozkaya A, Alkin Z, Faiz M, Yazici AT, Demirok A (2014) _Intravitreal_ bevacizumab for choroidal neovascularization secondary to angioid streaks: a report of two patients. Saudi J Ophthalmol 28(4): 316- 318.
-
Finger RP, Charbel IP, Schmitz-Valckenberg S, Holz FG, Scholl HN (2011) Long-term effectiveness of intravitreal bevacizumab for choroidal neovascularization secondary to angioid streaks in _pseudoxanthoma elasticum_. Retina 31(7): 1268-1278.
-
Finger RP, Charbel PI, Ladewig M, Holz FG, Scholl HP (2008) _Intravitreal_ bevacizumab for choroidal neovascularisation associated with _pseudoxanthoma_ _elasticum_. Br J Ophthalmol 92(4): 483-487.
-
Gelisken O, Hendrikse F, Deutman AF (1988) A long- term follow-up study of laser coagulation of neovascular membranes in angioid streaks. Am J Ophthalmol 105(3): 299-303.
-
Piro PA, Scherga D, Fine SL (1983) Angioid streaks: natural history and visual prognosis. In: Fine SL, Owens SL (Eds.), Management of Retinal Vascular and Macular Disorders, Williams & Wilkins, US, pp: 136-139.
-
Al-Rashaed S, Arevalo JF (2012) Long-term follow- up of choroidal neovascularization secondary to angioid streaks: case series and literature review. Clin Ophthalmol 6: 1029-1034.
-
Rissotto F, Querques G (2025) An update on emerging treatments for patients with angioid streaks. Future Rare Diseases 5: 1.
-
Pfau K, Lengyel I, Ossewaarde-van NJ, Van Leeuwen R, Risseeuw S, et al. (2024) _Pseudoxanthoma elasticum_ – genetics, pathophysiology, and clinical presentation. Prog Retin eye Res 102: 101274.
-
Almeida S, Filgueira SCL, Makarckyk LSQ, Castanho RFP (2025) Multimodal ophthalmological evaluation in a case of angioid streaks, with comet tail lesions and extensive traumatic lesions, in a patient with _pseudoxanthoma_ _elasticum_. Brazilian Journal of Health Review 8: 1.
-
Germain DP (2017) _Pseudoxanthoma elasticum_. Orphanet J Rare Dis 12(1): 85.
-
Kandasamy S, Shaikh N, Surve A, Kumari S, Bhayana AA, et al. (2025) Comprehensive review of angioid streaks. Indian J Ophthalmol 73(Suppl 1): S47-S54.
-
Finger RP, Charbel PI, Schmitz-Valckenberg S, Holz FG, Scholl HN, et al. (2011) Long-term effectiveness of intravitreal bevacizumab for choroidal neovascularization secondary to angioid streaks in _pseudoxanthoma elasticum_. Retina 31(7): 1268-1278.
-
Mimoun G, Ebran JM, Grenet T, Donati A, Cohen SY, et al. (2017) Ranibizumab for choroidal neovascularization secondary to _pseudoxanthoma elasticum_: 4-year results from the PIXEL study in France. Graefes Arch Clin Exp Ophthalmol 255(8): 1651-1660.
-
Chakraborty S, Sheth JU (2022) Case Report _Intravitreal_ _Brolucizumab_ for Choroidal Neovascularization Associated to Angioid Streaks. Case Reports in Ophthalmological Medicine pp: 1-4.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report
- Refractive Status of Retinoblastoma Patients in a Tertiary Eye Care Centre of Bangladesh