Giant Kissing Naevus: An Oculoplastic Challenge
A kissing naevus is usually congenital and found in approximately 1–3% of neonates. These lesions are present at birth and gradually affect both upper and lower eyelids and extend to the eyelid margin. There is a risk of developing malignant melanoma, which ranges from 5–40%. The larger the size of the naevus, the higher the chance of developing malignant change. We present a case of a congenital melanocytic giant kissing nevus involving the entire upper and lower eyelids in a fourteenyear- old male boy who was surgically correcting the lesion. Surgical correction is always challenging to reconstruct; the eyelid looks normal. Multiple sessions are required to get the optimum result.
Kadir SMU¹* and Haider MG²
¹Department of Oculoplasty, National Institute of Ophthalmology and Hospital, Bangladesh ²Professor and Director-Medical Education, Bangladesh Eye Hospital and Institute, Bangladesh Keywords: Giant; Melanocytic; Naevus; Eyelid; Reconstruction
Introduction
A kissing nevus is a compound variety of congenital pigmented naevus that affects both the upper and lower eyelids equally and involves the eyelid margins [1, 2]. Congenital naevus is a rare melanocytic lesion and has a risk of developing malignant melanoma that is proportional to the size of the lesion, specifically giant congenital naevus, if it involves over 5% of the body surface or the lesion size is more than 20 cm in adolescents [3, 4]. Here, we attempt a case report on a giant melanocytic naevus of the eyelids which is challenging to manage in surgical aspect.
Case Report
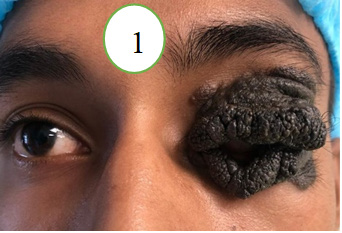
A 14-year-old male boy presented with a diffuse, large painless enlarging pigmented lesion, involving both upper and lower eyelids of the left eye (Figure 1) which is starting from his birth which is increasing in size over the time. The upper lid lesion was a soft tissue lesion about (Wide*height)
3 cm × 2 cm, which is extend horizontally from lateral to medial canthus, and vertically up to eyebrow in lateral aspect. The upper eyelid crease could not be demarcated. The skin over the lesion was, coarse, multiple small lobulated, and pigmented with fine hair present over the lesion, large hairs are present in few areas. The lower eyelid mass was about 3 cm × 2 cm which was dark black colored pigmentation and hair bearing. Lateral aspect was pale dark pigmented lesion with large hair bearing. The visual axis was covered due the lesion which caused the mechanical ptosis of the left upper eyelid. The other variety of the ptosis could not be evaluated due to giant melanocytic lesion. The best corrected visual acuity (VA) in the right eye was 6/6 and left eye was counting fingers due to visual occluded amblyopia. Fundus of the right eye was normal. Slit lamp evaluation and fundus examination could not be performed preoperatively due to diffuse giant variety of melanocytic lesion. CT scan of the eye and adnexa revealed a heterogenous mass in the upper and lower eyelid in the left eye with extension to the median canthus and lateral canthus but not extending the lesion to the left orbit. The complete excision of the entire full thickness lesions of the both eyelids from the medial to lateral canthus was performed, and the excised tissue was sent for histopathological analysis, which revealed a compound melanocytic nevus involving both lids. The anterior lamella of each eyelid was reconstructed by the full thickness skin graft (Figure 2) which was harvested from antero-medial aspect of the right arm.
Haemostasis was secured through the surgery. We used 6–0 vicryl suture throughout the reconstructive surgery and 4-0 silk suture was used for tarsorrhaphy. The tarsorrhaphy was released after 6 weeks of the primary surgery. The surgery removed the obstruction of the visual axis and improved the aesthetic appearance of the patient (Figure 3). Eyelash reconstruction is still challenging for this patient and may need more session of the reconstructive surgery.


Discussion
Congenital melanocytic naevus usually appears at birth and is reported in about 1% of all newly born babies. Based on their architecture, benign melanocytic nevi are divided into three categories: junctional, compound, and intradermal [1, 4, 5].
Eyelid nevi can be flat, elevated, dome-shaped, or pedunculated. Flat lesions are often junctional nevi, dome- shaped lesions are often intradermal or compound nevi, and pedunculated lesions are usually intradermal nevi. Nevi are typically tan with deep brown pigmentation and are well- circumscribed, not associated with ulceration [1, 2, 4, 5].
Fuchs A [3] described the eyelids’ congenital divided or kissing nevus in 1919 [3]. Collenza D [6] published a case report on two patients with kissing nevi in 1937 [6]. Subsequently, a study by Callahan A [7], another study by Harrison A, et al. [8] are reported additional cases in various literature [7, 8]. In 1969, Ehlers N [9] reported a case series on 10 cases of the melanocytic kissing nevus [9].
Our study patient, a 14-year-old male boy, presented with a diffuse, large, painless, enlarging pigmented kissing naevus involving both upper and lower eyelids, including the left eye’s lid margin.
The risk of small melanocytic nevi to transforming malignant condition is still not clear, but the larger lesions of more than 4 cm have a chance of 4.6% for malignant transformation over a long time [1, 10, 11].
Fuchs A [3] managed two patients through simple excision; two required full-thickness skin grafts to repair the defect, two were treated with cryotherapy, and the remainder received no treatment [3].
It is always better to excision the lesion as early as possible because a large lesion requires more extensive excision and a difficult reconstructive procedure [12]. If the melanocytic naevus involving the subcutaneous tissue and deep dermis, the treatment consists of full-thickness excision followed by repair with a skin graft [12, 13, 14].
Jacob SM, et al. described the management of congenital melanocytic nevus or panda naevus or kissing naevus of the eyelid of a 25-year-old female patient who underwent surgical excision with a full-thickness skin graft for the residual defect [14]. In our study, we found that the traditional approach to treating a large kissing nevus on both the upper and lower eyelids involves completely removing the lesion in a vertical and horizontal direction until reaching the normal tissue depth. To reconstruct the front layer of the eyelids, a full-thickness skin graft is used. Additionally, we repair the levator muscle and adjust the upper eyelid crease during the surgery.
Current treatment options for Giant congenital naevus include surgical resection of the lesion, but there is no effective medical management for this type of lesion. Trametinib was recently used for a case of a school-going child with a giant congenital melanocytic naevus who was shown an AKAP9- BRAF fusion, which resulted in a good outcome as well as a dramatic improvement in the extent of the melanocytic naevus [15].
Conclusion
Complete surgical excision is the main modality for managing the congenital compound melanocytic kissing naevus. Multiple session of the reconstructive surgery is needed to get better functional and cosmetic results.
References
-
Rajput GC, Mahajan D, Chaudhary KP, Deewana V (2015) Kissing naevus arising from neural crest cells presenting as upper and the lower lid mass. J Neurosci Rural Pract 6(3): 417-419.
-
Westfall CT, Shore JW, Rubin PA, Jakobiec FA (1991) Kissing nevus masquerading as a viral papilloma. Ophthalmic Surg 22: 614-615.
-
Fuchs A (1919) Shared nevi of the eyelids. Clinical Monatsblatter ophthalmology 63: 678.
-
Chauhan DS, Guruprasad Y (2011) Congenital melanocytic nevus of upper eyelid. J Cutan Aesthet Surg 4(1): 61-64.
-
Becher OJ, Souweidane M, Lavi E, Kramer K, Lis E, et al. (2009) Large congenital melanotic nevi in an extremity with neurocutaneous melanocytosis. Pediatr Dermatol 26: 79-82.
-
Collenza D (1937) Nevi divisi pigmentari delle palpebre. Boll Oculist 16: 435-460.
-
Callahan A (1946) The removal of adjacent nevi of the eyelids. Am J Ophthalmol 29: 563-565.
-
Harrison R, Okun M (1960) Divided nevus. A clue to the intrauterine development of melanocytic nevi. Arch Dermatol 82: 235-236.
-
Ehlers N (1969) Divided nevus. Acta Ophthalmol (Copenh) 47(4): 1004-1011.
-
Lorentzen M, Pers M, Bretteville-Jensen G (1977) The incidence of malignant transformation in giant pigmented nevi. Scand J Plast Reconstr Surg 11: 163-167.
-
Tannous ZS, Mihm MC Jr, Sober AJ, Duncan LM (2005) Congenital melanocytic nevi: Clinical and histopathologic features, risk of melanoma, and clinical management. J Am Acad Dermatol 52: 197-203.
-
Huemer GM (2008) The value of full-thickness skin grafts in reconstruction of the periorbital region. Plast Reconstr Surg 121: 1857-1858.
-
Rolland S, Kokta V, Marcoux D (2009) Meyerson phenomenon in children: observation in five cases of congenital melanocytic nevi. Pediatr Dermatol 26(3): 292-297.
-
Jacobs SM, Couch SM, Custer PL (2013) Divided eyelid nevus: a lid-sparing, staged surgical approach. Am J Ophthalmol 156(4): 813-818.e1.
-
Mir A, Agim NG, Kane AA, Josephs SC, Park JY, et al. (2019) Giant Congenital Melanocytic Nevus Treated with Trametinib. Pediatrics 143: 3.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report
- Refractive Status of Retinoblastoma Patients in a Tertiary Eye Care Centre of Bangladesh