FAF in DME
FAF (Fundus auto Fluorescence) changes in DME (Diabetic macular edema) can range from normal FAF and increased FAF to decrease FAF. Increased FAF can be due to oxidative products accumulation such as lipofuscin while decreased FAF exudate accumulation and the death of photoreceptors. In DME there are four types of FAF patterns Normal, Cystoid, Spot and decreased FAF may be useful tool to compare the micro structure of the macula to BCVA.
Introduction
Diabetic macular edema (DME) causes early visual loss in diabetic patients and there are many tools for to diagnosis it, such as fluorescein angiography, and OCT but funds autofluorescence (FAF) is non invasive technology that may give us some useful data for DME using confocal laser scanning ophthalmoscopy.
Clinical Uses of FAF
Lipofuscin in RPE cell has fluorescent property which may provide us with useful data about pathophysiology mechanisms, diagnosis and monitoring disease progression that cannot be revealed using fluorescein angiography or OCT. The Technology is available for 40 years but it became more popular due to advances in digital imaging tech. FAF is already used to check RPE function and toxicity status in several diseases such as age related macular degeneration, retinal artery occlusion and hydroxychloroquine toxicity [1].
Findings of Funds Autofluorescence in DME
Studies have shown that FAF in diabetic macular edema (DME) may show damage to the retina and a correlation between visual acuity and the microstructure changes of the retina such as photoreceptor integrity. FAF changes in DME can range from normal FAF and increased FAF (iFAF) to decrease FAF (dFAF). There are two hypothesis explain the iFAF in DME the first is oxidative products accumulation due to activated microglia and thus lipofuscin maybe a product of oxidation; The second hypothesis is a window defect due to mechanically relocating the luteal pigment (that usually block the fluorescence) due to formation of intraretinal cysts in the out plexiform layer but studies showed even after resolving of cysts the iFAF has remained and thus maybe due to activated microglia.
dFAF is explained by FAF absorption by hard exudate accumulation and the death of photoreceptors and thus will reduce the production of lipofuscin.
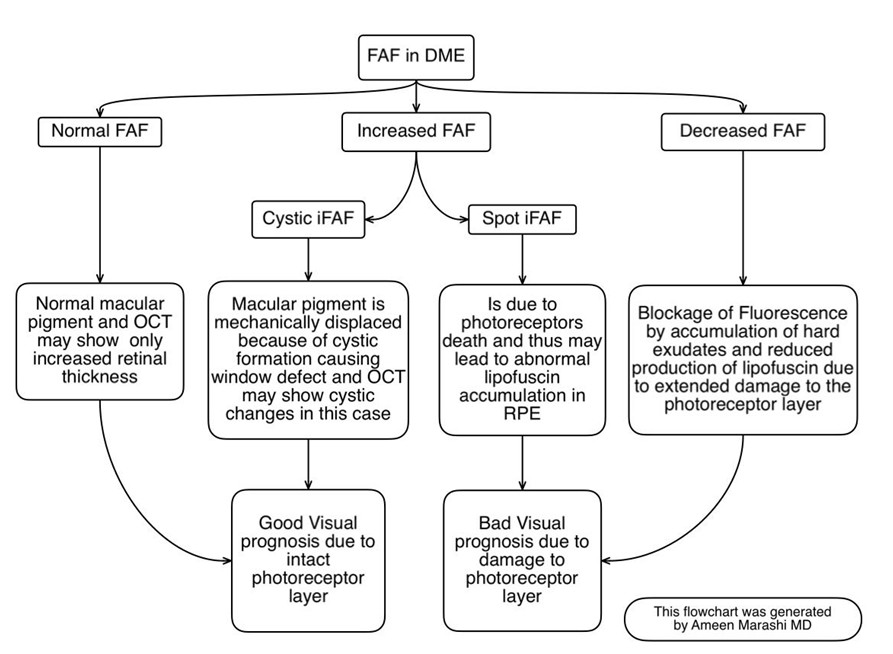
There are Four Main Patterns of FAF in DME
Normal FAF: Which may reflect a normal macular pigment and OCT may show no cystic changes only increased retinal thickness. Cystoid iFAF: Reflects autofluorescence due to macular pigment is mechanically displaced because of cystic formation causing window defect and OCT may show cystic changes in this case. Spot iFAF: Autofluorescence is due to photoreceptors death and may not be due to macular pigment displacement and thus may lead to abnormal lipofuscin accumulation in RPE. Decreased FAF: Is explained by blockage of Fluorescence by accumulation of hard exudates and reduced production of lipofuscin due to extended damage to the photoreceptor layer [2]. Visual function is better in the normal FAF and cystic iFAF and worse in spot iFAF and dFAF because of the status of photoreceptor layer integrity, where in the first two patterns the photoreceptor layer is intact where in the second two patterns the photoreceptor layer is damaged [3].
Conclusions
FAF can be useful tool to compare the micro structure of the macula to BCVA and as noted above where the spot iFAF and dFAF maybe a indicator of starting a chronic DME which may be an indicator to shift treatment from AntiVEGF to steroids as it may save the patient a multiple ANT VEGF injections and make us choose steroid as 1st line therapy especially in pseudophakic patients that are suspicious of chronic DME. More research is needed in comparing FAF in chronic and non chronic DME as studies showed that FAF can study the microstructure changes in diabetic macular edema and can be an indicator of IS/OS cell death which can interim indicate chronicity.
References
-
(2015) A novel way to use an old technology Clinicians, researchers look at early clinical implications of DME using fundus autofluorescence. By Vanessa Caceres, Contributing Editor.
-
Shen Y, Xu X, Liu K (2014) Fundus autofluorescence characteristics in patients with diabetic macular edema. Chin Med J (Engl) 127(8): 1423-1428.
-
Vujosevic S, Casciano M, Pilotto E, Boccassini B, Varano M, et al. (2011) Diabetic macular edema: fundus autofluorescence and functional correlations. Invest Ophthalmol Vis Sci 52(1): 442-448.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report