Prevalence and Types of Amblyopia among Primary School Children in Gondar town, Northwest Ethiopia
Background: Amblyopia is a unilateral or bilateral condition which results in visual reduction whilst the eye seems to be healthy. The main purpose of this study was to determine the magnitude and identify the types of amblyopia among primary school children in Gondar town, Northwest Ethiopia. Materials and Methods: A descriptive cross-sectional study was conducted among 1287 school children age between 6 - 15 years from January to February 2015 in Gondar. Complete ocular examination was carried by qualified optometrists and structured check list was used to collection socio – demographic data. Children with presenting vision less than 6/9 were fully examined for case confirmation and best corrected visual acuity was used to determine the type of amblyopia. Data were entered and analyzed using the Statistical Package for Social Sciences PSS 16 software computer package. Results: The prevalence of amblyopia was 4.7% (60). Anisometropic amblyopia and ametropic amblyopia each account 38.3%, while strabismic amblyopia, visual deprivation amblyopia and posterior segment abnormality contribute 6.7%% 8.3% and 8.3% respectively. Bilateral amblyopia was the most frequent 55% (33) and females account 56.7% (34). Conclusion: The magnitude of amblyopia was high in the study area. School screening programme for early detection and treatment is recommended to minimize the burden of visual loss due to amblyopia among primary school children in Gondar town.
Introduction
Vision development is a continuous dynamic process that occurs due to changes within visual system and it retains its plasticity within first decade of life. Amblyopia occur when inadequate stimulus in either one or both eyes during the critical period of development even after best corrections ended reduced visual acuity provide that no pathology detected [1]. Amblyopia is clinically defined as a reduction of Snell’s visual acuity of greater than two lines between the two eyes or an absolute reduction in acuity below 6/9 in either eye after best possible correction, without obvious pathology [1]. Amblyopia occurs as a result of defect from central visual pathways of the brain due to insufficient exposure to sharply focused images and different quality images from the two eyes [2, 3]. When there is mismatch between the images to each eye while eye itself looks normal, one eye is favored while the information from the other eye is suppressed [1, 3, 4, 5, 6, 7]. Amblyopia leads to unilateral or bilateral reduction of visual function, caused by form vision deprivation and or abnormal binocular interaction. The reduction in acuity persists despite correction of refractive error and other factors at late age [8]. Although reduced acuity is its most obvious defect, amblyopia is a complex functional anomaly affecting many aspects of visual performance which cannot be reversed in late age. Typically amblyopia ended reduced visual acuity accompanied by one or more known amblyogenic factors [6]. Hence, amblyopia can be classified as strabismic, anisometropic, derivational and ametropic. Among 625 million children under the age of 5 years worldwide, more than 15 million may have amblyopia, and more than half of them will not be identified before they reach school age in developed countries [1, 6, 7, 8]. The situation is far worse in developing nations even though irreversible vision loss could be prevented by performing early vision screening. The consequences of not early identifying and treating amblyopia include permanent visual impairment, adverse effects on school performance, poor fine motor skills, weak social interactions, and blurred self-image [7, 9]. More Importantly permanent monocular visual impairment due to amblyopia is a risk factor for total blindness, if there is injury on better eye in afterward life. School screening interventions are likely to be considered cost-effective relative to many other potential public health programs [7, 10]. Amblyopia has an Impact on health related quality of life, though treatment is likely to be very cost effective [11, 12, 13]. Hence improvement of visual acuity in young children is often dramatic after initiation of therapy in early life age. Gondar town is a home for tertiary eye care and training center with all categories of eye care specialists serving the community [4, 14]. However, school screening program is not yet established in Gondar primary schools as part of school eye health. This therefore leads to undetected vision problem which in turn results in irreversible vision loss. The magnitude of amblyopia in Gondar, Ethiopia has not been previously determined. Rather it has been left undiagnosed in school children. Therefore, this study determined the prevalence and the type of amblyopia which is hoped to be an evidence for school administrators, eye health professionals and organizations to support and to conduct regular vision screening programs in Gondar primary schools thereby to assure early identification and treatment of amblyopia. There were population based studies aimed to determine the prevalence of amblyopia. Accordingly, it was found out that amblyopia was responsible for more unilaterally vision reduced of childhood onset than all other causes combined. The overall prevalence of amblyopia in school- aged children on a multi-country refractive error study was 0.74% (0.64%-0.83%) [15]. In Germany, the prevalence of amblyopia among school children was 1.9% [16]. A cross-sectional study in Indian school children showed 4.8% prevalence of amblyopia, which was higher than general population [17, 18]. Using similar method among rural school children population of Kurnool District, India showed 0.66% prevalence of amblyopia. Again another study in Southern India school children showed 1.1% prevalence of amblyopia [19]. In Vietnam, cross-sectional study determined prevalence of amblyopia among school children to be 2.2% [20]. Similarly, in Jhapa, Nepal, the prevalence of amblyopia among school children was 2% [21]. Prevalence of amblyopia among children attending primary schools in Africa was 0.28%(16), while that of Minia county, Egypt was 1.49% [22, 23]. Similar study on Abha City, Saudi Arabia, school boys showed 1.85% [24] and 3.9 % in Qassim province school children. Similarly, in Oman the prevalence of amblyopia was 0.92% [25]. In sub-Saharan Africa, very few literatures focused on amblyopia [26]. However, there are studies concerning on refractive error and visual impairment in different parts of this region. The prevalence of amblyopia among school children in Ghana, Cameroon, Botswana and Nigeria were 9.9%, 8.9% 31% and 0.3% respectively. In the entire above studies, the major amblyogenic factor was refractive error. Similarly, in Ethiopia there were few empirical works aimed to determine the prevalence of refractive error and visual impairment and to depict about amblyopia [27, 28, 29, 30]. These studies describe amblyopia as a factor for visual reduction. In central Ethiopia rural school children, amblyopia accounts for 9.6% of vision reduction. Similarly, in central Ethiopia hospital-based study on ocular morbidity, amblyopia contributes for 14.3% of bilateral visual impairment [31]. Refractive error is among top causes of amblyopia according to studies in Africa and Ethiopia [32]. Prevalence of refractive error in the study area was 4.9% which was greater in females [33]. Similarly, prevalence of refractive error in central Ethiopia was 6.3%, 11.4% and 10.2. [31, 32, 34] Besides myopia followed by astigmatism was very common among males and females [31, 32, 33].
Materials and Methods
Study Design and Setting
A cross-sectional study design was employed to determine the prevalence and types of amblyopia among primary school children aged from 6 -15 in Gondar town from January to February, 2015.
Source and Study Population
One thousand two hundred eighty seven primary school children were randomly selected among 58 primary schools using multistage sampling technique. Twelve (12) schools out of 58 were included from grades 1-8 class. Students who attend their class on the date of data collection were included. All the sampled students were well-looking and hence they were not reported to have general health problem.
Data Collection Tools and Methods
Complete ocular examination was carried out for each child by qualified clinical optometrists. Socio - demographic data were also collected using a structured questionnaire before ocular examination. Anterior segment evaluation was assessed at class room prepared for the purpose of the study using direct ophthalmoscope and handheld slit lamp bio-microscope. Visual acuity was assessed in a well lit room using log MAR acuity chart. Refractive error was objectively assessed using retinoscope refined subjectively using both sphere and cylindrical lenses. Students with visual acuity less than 6/9 had undergone further examination using dry and wet retinoscopy for objective and subjective determination of refractive error at hospital based eye care unit at Gondar University tertiary eye care and training center . Visual acuity after best possible correction was considered to categorize in to amblyopia.
Definitions Used for the Study
Amblyopia was defined as best corrected visual acuity in one or both eyes ≤ 6/12 and or visual acuity (VA) of difference between the two eyes ≥2 lines without obvious pathology. Anisometropia was defined as refractive anomaly with power difference between the two eyes ≥1.00 D and strabismus was a manifest deviation of the visual axis of either or both eyes. Myopia was defined as a refractive error of ≤ -0.50 D on subjective refraction while hypermetropia was considered a refractive error of ≥+0.75D on subjective refraction. Astigmatism was considered a power difference between the two meridians of ≥ 0.50D. All the definition of refractive errors was based on the spherical equivalent of the refined subjective refraction.
Data Management and Analysis
After coding data were entered, cleaned and analyzed using SPSS version 16 software computer package. Data were presented descriptively using tables and figures.
Ethical Considerations
The study was approved by the research ethical review committee of University of Gondar. Permission was also obtained from each school head master, class room teachers. Students and parents were informed about the purpose of the study in their local language with a written consent form. Further examination of children with ocular conditions was treated at Gondar University hospital tertiary eye care and training center.
Results
Scio Demographic Characteristics of Study Population
One thousand two hundred eighty seven children were participated in the study with a participation rate of 97.5 %. The mean age of the participants was 10.78± 2.43 years. Seven hundred five (54.8%) were females. Eight hundred two (62.3 %) were 10 years and above.
Prevalence of Amblyopia
The prevalence of amblyopia was 4.7% (60 / 1287) (CI, 4.687%-4.713%). From the total of children with amblyopia, females contribute 56.7 % (34 / 60). Amblyopia was more common (41 out of 802) in the relatively older age group (10 to 15 years) compared to the younger age group (6 to 9 years old) school children. However, this difference was not statistically significant (p=0.84).
| Age category (years) | ||||
|---|---|---|---|---|
| 9-Jun | 15-Oct | Total | ||
| Amblyopia | Yes | 19 | 41 | 60 |
| No | 466 | 761 | 1227 | |
| Total | 485 (37.7%) | 802 (62.3%) | 1287 (100%) |
Table 1: Amblyopia distribution in terms of age group among Gondar town primary school children, 2015.
Types of Amblyopia
Bilateral amblyopia 55% (33) was encountered more frequently than unilateral amblyopia cases which account 45% (27). The common types of amblyopia were anisometropic amblyopia 38.3% (23), ametropic 38.3% (23), strabismic amblyopia 6.7% (4), derivational amblyopia 8.3% (5) and posterior segment abnormality 8.3% (5).
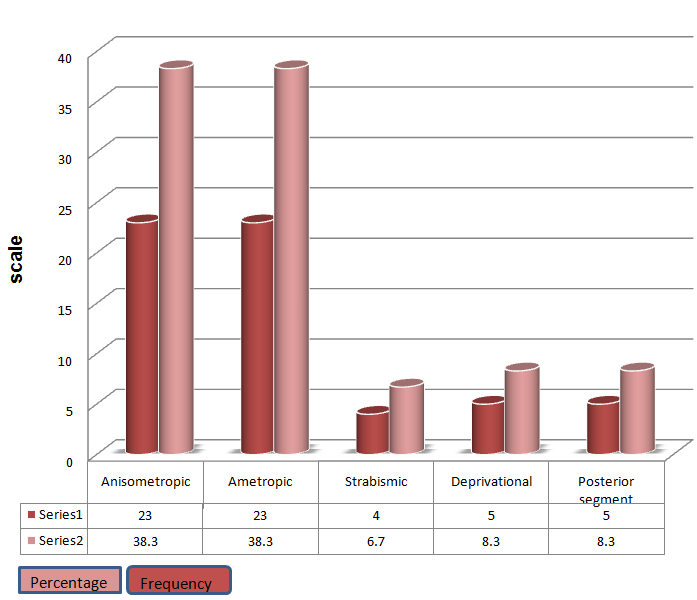
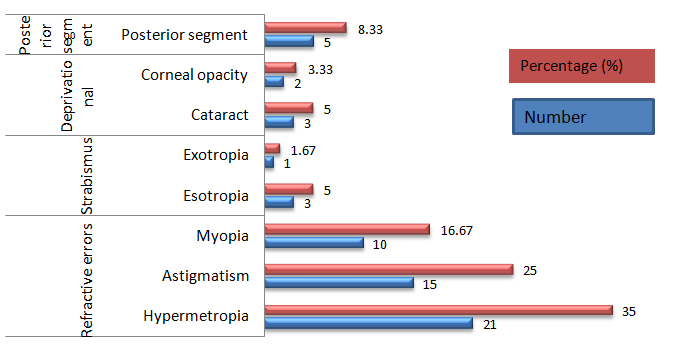
Refractive error contribute lion share for amblyopia occurrence. Hence, according to this study hypermetropia was found common amblyogenic factor followed by astigmatism and myopia.
Discussion
Prospective cross sectional study was done from January to February, 2015 among school children between ages 6 -15 years old. Out of the 1287 children examined, 4.7 % (60) of them were found to have amblyopia. It was comparable to a similar study done in India [4.8%]. However, this result was higher than other studies conducted in developed nations, for example in United States and Germany [18]. This might be due to the fact that, school children with eye problem in this study area may not have an opportunity for early case detection and treatment [7, 15, 17]. Similarly, prevalence of amblyopia in the study area was found to be higher than a multinational study in the world and Africa. This might be because of low economic development and lower eye health awareness by parents to have regular check up [16]. The prevalence is higher not only in similar studies conducted in developed world, but also much higher in developing countries like India, Vietnam, Nepal, Egypt, Saudi Arabia and Oman. The possible reason could be school children in Gondar town might have high prevalence of uncorrected refractive error according to the study done in 2008 in the same population [8, 19, 20, 21, 22, 23, 25, 26, 33]. Furthermore, the population of the study area has low access to preschool and school vision screening programs compared to other countries with lower economic status and poor awareness to vision check at existing tertiary hospitals. In the present study, the most commonly encountered types of amblyopia among primary school children were anisometropic, ametropic, strabismic and derivational amblyopia. Such a finding was in line with the various studies done in different countries [2, 19, 20, 23, 25, 26]. Regarding type of amblyopia, anisometropic amblyopia (38.3%) and ametropic amblyopia (38.3%) contributed the majority. This might be due to the high prevalence of uncorrected refractive error in similar study population. This was supported by refractive error studies done in a study area. And across Ethiopia wind up myopia was a common type of refractive error followed by astigmatism and hypermetropia [33]. Among the types, prevalence of anisometropic amblyopia (38.3%) was higher compared to strabismic amblyopia (6.7%) and derivational amblyopia (5%) [33, 34]. It was in line with other studies conducted in different nations [2, 23, 25]. Ametropic amblyopia was a common type of amblyopia compared to strabismic and derivational amblyopia. The result was similar to other studies conducted so far (20). This might be attributed to the high prevalence of uncorrected refractive error. According to this study, the prevalence of amblyopia was higher in females (56.7%) than in males (43.7%). This was in line with a similar study in India. However it also contradicts with other studies in India [19, 2, 20]. For example there was no statistically significant difference between males and females (P=0.76). Such a finding was similar to a study conducted in Saudi Arabia [25] and Africa [16]. Binocular amblyopia was frequently encountered 33 (55%) than monocular amblyopia 27 (45%) despite the fact that it is not statistically significant (p=0.99). Thus it does not conform to results from various studies in different nations across the world. This might be because of higher proportion of amblyopia caused by uncorrected refractive cases like anisometropia and ametropia since refractive error prevalence was high in the study area in which myopia stood first followed by astigmatism and hypermetropia [16, 18, 19, 25]. According to this study, leading type amblyogenic refractive error was hypermetropia followed by astigmatism and myopia [33]. As a result it contradict from overall prevalence of refractive error types done in study area [33].
Conclusion
Prevalence of amblyopia in the study area was found to be high compared to other studies while binocular amblyopia was found common. Besides anisometropic and ametropic amblyopia were common types. Early diagnosis and treatment of amblyogenic factors for school children can minimize permanent vision loss. Therefore, frequent eye screening program has to be established and performed regularly in the study area.
References
-
William H, Bernarad G (2004) Pediatric optometry. Spain: Butterworth Heinemann.
-
Janti SS, Raja AM, Matheen A, Charanya C, Pandurangan R (2014) A cross sectional study on Prevalence of amblyopia in school going children. J of Evolution of Med and Dent Sci 3(30): 8561-8565.
-
Myron Y, Jay D (2004) Ophthalmology. 2nd (Edn.), Spain: Mosby.
-
Mai K El Mallah, Usha Chakravarthy, Hart PM (2000) Amblyopia: is visual loss permanent? Br J Ophthalmol 84(9): 952-956.
-
Theodore G (2007) Primary care optometry. 5th (Edn.), China: Butterworth Heinemann.
-
Terry B (1993) Visual problems in children. Great Britain: Butterworth Heinemann.
-
Eileen EB (2013) Amblyopia and Binocular Vision. Prog Retin Eye Res 33: 67-84.
-
Pradeep S (1999) Strabismus. India: CBS.
-
Wu C, Hunter DG (2006) Amblyopia: diagnostic and therapeutic options. Am J Ophthalmol 141(1): 175- 184.
-
Harrad R, Williams C (2003) Risk, causes and outcomes of visual impairment after loss of vision in the non-amblyopic eye, a population-based study. Surv Ophthalmol 48(2): 235-236.
-
David B Rein, John S Wittenborn, Xinzhi Zhang, Michael Song, Saaddine JB (2012) The Potential Cost- Effectiveness of Amblyopia Screening Programs. J Pediatr Ophthalmol Strabismus 49(3): 146-155.
-
Maharaja YI, Naidooa KS, Dabideena R, Ramsona P (2011) The KwaZulu-Natal Child Eye Care Programme: Delivering refractive error services to primary school learners. S Afr Optom 70(2): 61-68.
-
Williams C, Northstone K, Harrad RA, Sparrow JM, Harvey I (2003) Amblyopia treatment outcomes after preschool screening v school entry screening: observational data from a prospective cohort study. Br J Ophthalmol 87(8): 988-993.
-
Konig HH, Barry JC (2004) Cost effectiveness of treatment for amblyopia. Br J Ophthalmol 88(5): 606- 612.
-
Ophthalmology AAO (2011) Pediatric Ophthalmology and Strabismus. Singapore: The Eye M.D Association.
-
Xiao O, Morgan IG, Ellwein L, He M (2014) Prevalence of amblyopia in school-aged children and variations by ethnicity: a multi-country refractive error study in children. Ophthalmol Vis Sci 55(13).
-
Haase W, Mühlig HP (1979) The incidence of squinting in school beginners in Hamburg Klin Monbl Augenheilkd 174(2).
-
Janti SS, Adnan Matheen AMR, Charanya C, Pandurangan R (2014) A cross sectional study on prevalence of amblyopia in school going children. Journal of Evolution of Medical and Dental Sciences 3(30): 8561-8565.
-
Anjaneyulu K, Reddy GN (2015) Prevalence of Amblyopia in Children Aged from 5-15 Years in Rural Population Kurnool Dist. Andhra Pradesh, India. International Journal of Science and Research 4(2): 99-100.
-
Sunil Ganekal, Vishal Jhanji, Yuanbo Liang, Dorairaj S (2013) Prevalence and etiology of amblyopia in Southern India: results from screening of school children aged 5-15 years. Ophthalmic Epidemiol 20(4): 228-231.
-
Prakash Paudel, Prasidh Ramson, Thomas Naduvilath, David Wilson, Ha Thanh Phuong et al. (2014) Prevalence of vision impairment and refractive error in school children in Ba Ria – Vung Tau province, Vietnam. Clin Experiment Ophthalmol 42(3): 217- 226.
-
Gauri Shankar Shrestha, Digen Sujakhu, Joshib P (2011) Refractive error among school children in Jhapa, Nepal. J Optom 4(2): 49-55.
-
Sahar T Abdelrazik, Khalil MF (2014) Prevalence of amblyopia among children attending primary schools during the amblyogenic period in Minia county. J Egypt Ophthalmol Soc 107 (4): 220-225.
-
Abolfotouh MA Badawi I, Faheem Y (1994) Prevalence of amblyopia among schoolboys in Abha city, Asir Region, Saudi Arabia. J Egypt Public Health Assoc 69(1-2): 19-30.
-
Aldebasi YH (2015) Prevalence of amblyopia in primary school children in Qassim province, Kingdom of Saudi Arabia. Middle East Afr J Ophthalmol 22(1): 86-91.
-
Lithander J (1998) Prevalence of amblyopia with anisometropia or strabismus among schoolchildren in the Sultanate of Oman. Acta Ophthalmol Scand 76(6): 658-662.
-
Kumah BD EA, Abdul-Kabir M, Ahmed AS, Koomson NY, Aikins S, et al. (2013) Refractive error and visual impairment in private school children in Ghana. Optom Vis Sci 90(12): 1456-1461.
-
Noche CD, Kagmeni G, Bella AL Epee E (2011) Prevalence and etiology of amblyopia of children in Yaoundé (Cameroon), aged 5-15 years. Sante 21(3): 159-164.
-
Nallasamy S, Anninger WV, Quinn GE, Kroener B, Zetola NM et al. (2011) Survey of childhood blindness and visual impairment in Botswana. Br J Ophthalmol 95(10): 1365-1370.
-
Megbelayin EO (2012) Prevalence of amblyopia among secondary school students in Calabar, south- south Nigeria. Niger J Med 21(4): 407-411.
-
Mehari ZA, Yimer AW (2013) Prevalence of refractive errors among schoolchildren in rural central Ethiopia. Clin Exp Optom 96(1): 65-69.
-
Mehari ZA (2014) Pattern of childhood ocular morbidity in rural eye hospital, Central Ethiopia. BMC Ophthalmol 14(50).
-
Yared AW, Belaynew W, Destaye S, Ayanaw T, Zelalem E (2012) Prevalence of refractive errors among school children in gondar town, northwest ethiopia. Middle East Afr J Ophthalmol 19(4): 372- 376.
-
Sewunet SA, Aredo KK, Gedefew M (2014) Uncorrected refractive error and associated factors among primary school children in Debre Markos District, Northwest Ethiopia. BMC Ophthalmol 14(95).
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report