Future Perspectives about Genetics of Congenital Glaucoma
As everybody knows, glaucoma is the leading cause of irreversible blindness worldwide. Most of glaucoma patients are elderly but congenital glaucoma (CG) and glaucomas of childhood are important causes of visual disability. Congenital glaucoma is isolated, non-syndromic glaucoma that occurs in the first three years of life and is one of the major causes of childhood blindness.
Editorial
As everybody knows, glaucoma is the leading cause of irreversible blindness worldwide. Most of glaucoma patients are elderly but congenital glaucoma (CG) and glaucomas of childhood are important causes of visual disability. Congenital glaucoma is isolated, non-syndromic glaucoma that occurs in the first three years of life and is one of the major causes of childhood blindness. Early- onset glaucomas may arise secondary to developmental abnormalities, such as glaucomas with aniridia or as part of Axenfeld-Rieger syndrome a/or Peters’ anomaly. Congenital glaucomas have strong genetic bases and disease-causing mutations have been discovered in several genes since Sarfarazi 1995 [1]. Mutations in three genes (CYP1B1, LTBP2, TEK) have been reported in congenital glaucoma patients (Figure 1).
![Figure 1: CYP1B1. Axenfeld-Rieger syndrome is caused by mutations in PITX2 or FOXC1 and aniridia and Peters’ anomaly are caused by PAX6 mutations [2] (Figure 2).](/fulltextimages/1242/fig_1.jpeg)
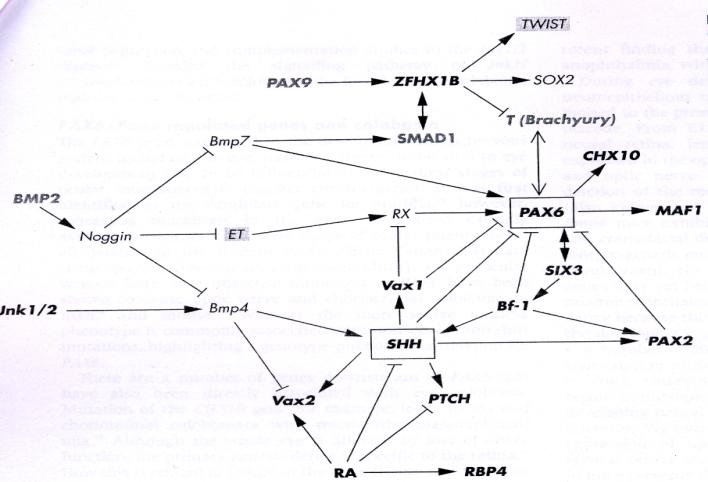
Figure 2: Coloboma gene network (CGN) model. Mutations in genes or signalling molecules that are associated with coloboma are depicted in bold black text. Mutations in genes that are associated anophthalmia/microphthalmia are in normal text. Mutations in genes that are associated with other eye defects are shaded grey. Genes in bold grey text have not been associated with developmental eye defects, but are directly involved in regulation/interaction of downstream coloboma target genes. SHH and PAX6 are boxed as they regulate many genes associated with coloboma. Human genes are in uppercase, and mouse genes are in lowercase. Clinically, congenital glaucoma is characterized by high intraocular pressure (IOP), epiphora, corneal oedema, photophobia, blepharospasm and ocular enlargement. The disease is bilateral in approximately 75% of patients. CG incidence varies substantially among countries: it is estimated to occur in about 1/10000 births in Europe, in
1/2500 in Saudi Arabia and 1/1250 in the gipsy population in Slovakia (Online Mendelian Inheritance in in Man, OMIM 231300). From a pathophysiological point of view, an increase in IOP, untreated either with surgery or pharmacological therapy, results in ocular enlargement (buphthalmos) and rapidly progressive cupping of the optic nerve with severe and irreversible damage of the visual field. Early recognition and therapy can significantly improve the child’s visual function. Onset of an aggressive form of glaucoma occurs between birth and 3 years of age. The disease has higher prevalence in males (2:1; M/F). Most cases of CG are sporadic and recessive inheritance of CG is common, with almost complete penetrance in populations with high consanguinity rate. Reduced penetrance (40% in some populations) and various phenotypic forms suggest a polygenic inheritance pattern or multi factorial aetiologies. In a paper published in Ophthalmic Genetics in 2011 we confirmed the major role of CYP1B1 gene in congenital glaucoma and we suggested an autosomic recessive role of MYOC/TIGR in a digenic inheritance model [3]. Treatment of diseases with gene therapy is advancing rapidly and is the future of the therapy of glaucoma. Genes offer numerous advantages over conventional drugs. The gene therapy use both viral and nonviral vectors. The eye is an ideal organ for gene therapy. It is easily accessible and it is an immune-privileged site. Currently, there are clinical trials for diseases affecting practically every tissue of the eye, mostly trying to restore vision in patients affected by Leber congenital amaurosis. The number of eye trials compared with those for systemic diseases is quite low (1.8%). One area for eye gene therapy is glaucoma, where a long-term gene drug would eliminate daily applications and compliance issues. The future of glaucoma therapy is the possibility for treating the trabecular meshwork to lower intraocular pressure (IOP) and the retinal ganglion cells (RGC) to protect them from neurodegeneration [4].
References
-
Sarfarazi M, Akarsu AN, Hossain A, Turacli ME, Aktan SG, et al. (1995) Assignment of a locus (GLC3A) for primary congenital glaucoma (Buphthalmos) to 2p21 and evidence for genetic heterogeneity. Genomics 30(2): 171-177.
-
Lewis CJ, Hedberg-Buenz A, De Luca AP, Stone EM, Alward WLM, et al. (2017) Primary congenital and developmental glaucomas. Hum Mol Genet 26(R1): R28-R36.
-
Giuffre I (2011) Molecular analysis of patients affected by congenital glaucoma. Ophthalmic genetics 2011-08-04 e pub ahead of print.
-
Borras T (2017) The pathway from genes to gene therapy in glaucoma: a review of possibilities for using genes as glaucoma drugs. Asia Pac J Ophthalmol 2017 6(1): 80-93.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report