Biomechanical Impact of Femto-Second Laser Arcuate Keratotomy
It has long been assumed, and since some years is known that refractive surgical treatments have an impact on the biomechanics of the cornea. Therefore, it is even more important to understand the underlying biomechanical mechanism of such procedures.
Mini Review
It has long been assumed, and since some years is known that refractive surgical treatments have an impact on the biomechanics of the cornea. Therefore, it is even more important to understand the underlying biomechanical mechanism of such procedures. One such surgical technique, exploiting biomechanical effects to treat corneal astigmatism, is femto-second laser arcuate keratotomy (AK). Manual AK incisions were being used for years in clinical practice, but were abandoned by many because of too poor outcome predictability. Now with the femto-second (FS) laser getting more and more popular, the technique sees a comeback in clinics. FS Laser manufacturers such as Alcon, Bausch+Lomb, Johnson+Johnson Vision, or Ziemer are already providing the ability to cut arcuates into corneal tissue. In this context, it is interesting to note, that two recent (2016) consecutive publications by the same authors of the Moorfields Eye Hospital in London focused on efficacy, predictability, sensitivity, and the effect of multiple parameters in the femto-second laser intrastromal arcuate keratotomy. Printed one after another, in the same issue of the Journal of Cataract and Refractive Surgery (Issue 42, 2016), the first study by Alexander C Day, et al. describes the effects and results of intrastromal femto-second astigmatic keratotomy (AK) [1]. Due to the minimal data about the efficacy of intrastromal AK, it aims to determine the astigmatic changes happening in this intervention.196 eyes were used, and the operation was planned with nomograms. The corneas all underwent an astigmatic correction additionally to a cataract surgery. They then were analyzed with three vectors of the Alpins method: the target induced astigmatism (set at 0, to facilitate calculations), surgically induced astigmatism, and the difference vector. Additional parameters were the correction index, the coefficient of adjustment, the magnitude and angle of error, and the index of success. The results are summarized in Table 1.
- Vector analysis parameter values (N = 196 eyes)
- Parameter
- Mean (SD)
- Range
- Target induced astigmatism [D]
- 1.21±0.42
- 0.75, 2.64
- Surgically induced astigmatism
- [D]
- 0.74±0.40
- 0.00, 2.86
- Difference vector [D]
- 0.74±0.38
- 0.00, 2.25
Table 1: Target- and surgically induced astigmatism for
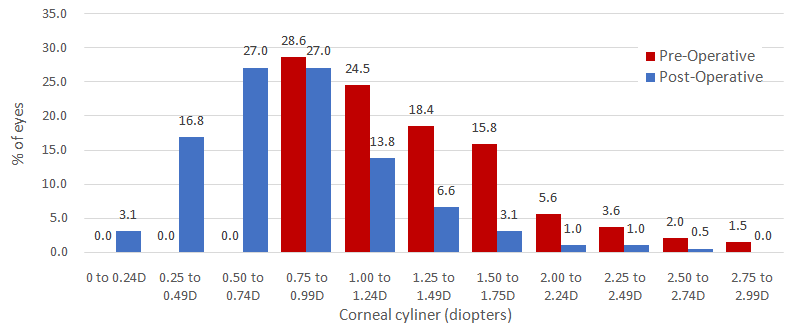
astigmatism, and that the between-eye variance in the astigmatism vector must be further analyzed see Figure 1.
additionally want to analyze the effects of corneal biomechanical parameters on the efficacy of the operation [2]. The selected preoperative parameters were axial length, anterior chamber depth, central corneal thickness, corneal hysteresis, corneal resistance factor and some more, as can be seen in Table 2.
| Multiple variable regression model of dependent variable SIA induced by femto-second AK | |||||||||||
| Variable | B Value | B 95% CI | P Value | ||||||||
| Femto-second arc length [°] | 0.005 | 0.001, 0.008 | 0.006 | ||||||||
| Preoperative cylinder [D] | 0.347 | 0.220, 0.474 | <0.001 | ||||||||
| Age [years] | 0.005 | 0.000, 0.009 | 0.044 | ||||||||
| Astigmatism type (oblique/WTR/ATR) | -0.067 | -0.131, -0.004 | 0.038 | ||||||||
| Corneal hysteresis | -0.063 | -0.099, -0.027 | 0.001 | ||||||||
| Corneal resistance fractor | 0.044 | 0.080, 0.800 | 0.018 |
Table 2: Multi-variat regression modeling of surgical outcome of 319 eyes, receiving intrastromal arcuate keratotomy Table 2: Mul
Table 2: Multi-variat regression modeling of surgical outcome of 319 eyes, receiving intrastromal arcuate keratotomy Table 2: Multi-variat regression modeling of surgical outcome of 319 eyes, receiving intrastromal arcuate keratotomy surgery, operated with a femto-second surgical laser. The study included 319 eyes which underwent an astigmatism reduction in addition to the normal cataract surgery. Results primarily showed that long and deep incisions as well as high preoperative cylinder correlate with higher astigmatic correction. Regression analysis indicated that increasing patient age was associated with the SIA magnitude. In a second step, the authors considered biomechanical parameters, and correlated them to astigmatic effects.Results showed that surgically induced astigmatism is meridian-dependent and its magnitude is greater when corneal hysteresis (CH) is lower, but its corneal resistance factor (CRF) is higher. It also appeared that WTR (with the rule) astigmatism induces a 0.13 higher SIA than ATR (against the rule). Finally, the authors state that out of all parameters they looked at, only preoperative corneal cylinder magnitude, AK depth, and the steep astigmatism meridian were independent predictors for surgically induced astigmatism. Moreover, the correlation between incision length and the induced astigmatic correction was found to be poor. It is interesting to see, that a surgical technique abandoned by many, sees a revival thanks to femto- second laser technology. Even though clinical results are promising, it appears that there is room for improvement, and that more studies and improved surgery planning technologies are needed.
References
-
Alex Day, Lau NM, Stevens JD (2016) Nonpenetrating femtosecond laser intrastromal astigmatic keratotomy in eyes having cataract surgery. Journal of Cataract and Refractive Surgery 42(1): 102-109.
-
Alex Day, Stevens JD (2016) Predictors of femtosecond laser intrastromal astigmatic keratotomy efficacy for astigmatism management in cataract surgery; Journal of Cataract and Refractive Surgery 42(2): 251-257.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report