Pearls for Refractive Cataract Surgery
The cataract surgery has gone leaps and bounds from the days of intracapsular to extracapsular and then phacoemulsification and now a new Era of refractive cataract surgery.
Mini Review
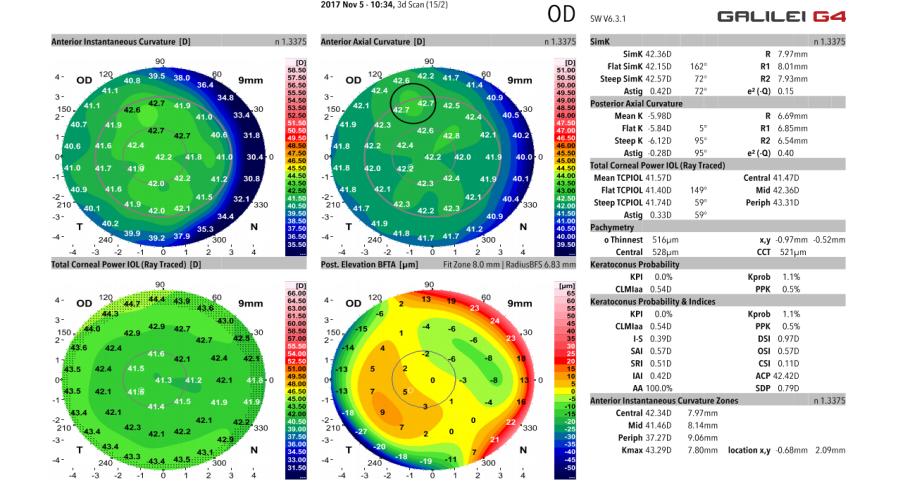
The cataract surgery has gone leaps and bounds from the days of intracapsular to extracapsular and then phacoemulsification and now a new Era of refractive cataract surgery [1]. The technology has evolved and similarly the expectations of our patients has increased tremendously they not only demand an improvement in vision but also relatively spectacle free vision postoperatively. The role of topography in planning a refractive cataract surgery is immense. It tells us about the astigmatism whether it’s regular or irregular [2, 3]. A sphericity of the cornea positive or negative there by planning a negative or a positive aspheric IOL [4, 5]. Gives information about the posterior curvature of the cornea. Irregular posterior corneal surface will likely to lead to suboptimal refractive outcomes after diffractive multifocal or trifocal IOL implantation. Galilee topographer has 4 refractive maps the best fit toric map has AAI index which takes the difference of the most elevated point and the most depressed point if the value is more than 21 it tells us that the cornea is very irregular which becomes a relative contraindication to implantation of premium IOL especially a trifocal or multifocal’s. It’s important to look out for the higher-order aberrations especially the values of vertical and horizontal coma. If the values are more than 0.35 indefinitely tells us that the patient is going to be less happy after multifocal IOL implantation even though the vision may be 20/20.
Similarly if the astigmatism is irregular toric IOLs are not a solution for it. The posterior corneal astigmatism has to be taken into account while calculating toric IOL power calculation. There are various on line software like Barrett’s toric IOL calculator which takes into account posterior corneal astigmatism thereby predicting a better refractive outcome and the precise spherical equivalent. Sometimes we come across irregular astigmatism with different keratometry readings on topographer auto keratometer and IOL master [6, 7, 8]. If there is mild irregular astigmatism it can be dealt by taking the readings which agree most with each other and fed into equalant K program of Barrett’s toric IOL calculator this will give the best suited toric model. In spite of this be prepared for some surprises because the keratometry readings are not accurate what we are feeding into the software. Be a blessed to have the luxury of laser vision correction in case of any postoperative surprises. Allow the refractive error to settle postoperatively for 2-3 months rule out any causes of secondary refractive error like dry eyes lookout for a stable refraction and then proceed with surface laser or laser in situ keratomileusis. Piggyback IOLs is another option when there is a refractive surprise beyond the range of laser vision correction of air laser vision correction might cause more aberrations. Morsher’s extra focus IOL is an exciting option for focal corneal scar not in visual axis causing irregular astigmatism and if there is an iris loss especially posttraumatic cases who improve with pinhole (Figure).
References
-
Anderson D, Kojima R, Aurora I (2007) Topography: A clinical pearl. Optom Manag 42(2): 35.
-
McKay T (1998) A Clinical Guide to the Humphrey Corneal Topography System. Dublin, CA: Humphrey.
-
Mack C, Merchea M (2006) Advanced Corneal Imaging and Interpretation in the Diagnosis and Treatment of Corneal Disease. AAO lecture Denver.
-
Roberts C (1998) A Practical Guide to the Interpretation of Corneal Topography. CL Spectrum 13(3): 25-33.
-
Caroline P, Andre M (2001) Elevating our Knowledge of the Corneal Surface. CL Spectrum 16(4): 56.
-
Mountford J, Noack D (2002) Corneal Topography and Orthokeratology: Post-Fit Assessment.
-
Tang M, Shekhar R, Miranda D, Huang D (2005) Characteristics of keratoconus and pellucid marginal degeneration in mean curvature maps. Am J Ophthalmol 140(6): 993-1001.
-
Shovlin JP (2005) Do I see Keratoconus or PMD? Rev Optom 142(4): 91.
-
Mountford J, Caroline P, Noack D (2002) Corneal Topography and Orthokeratology: Pre- Fitting Evaluation.
-
Medmont (2006) International Pty Ltd. Medmont E300 Corneal Topographer User Manual. Australia: Medmont Intl 43.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report