Ultrasound Biomicroscopy in Ophthalmology; An Updated Mini –Review
Ultrasonic biomicroscopy (UBM) is an imaging technique that utilizes 50-80MHz high-frequency sound waves to produce a high-resolution image with penetration depth of about 5 mm. It has multiple applications in ophthalmology to evaluate anterior segment structures; cornea, angle, iris, peripheral choroid, as well as foreign bodies localization. The present article is an updated mini-review regarding the use of UBM as one of anterior segment imaging devices, and its clinical applications.
Introduction
Ultrasound biomicroscopy (UBM) was first developed by Pavlin’s group in Canada. UBM has frequencies in the 50 to 100 MHz range, so it is useful in imaging of conjunctiva, sclera, cornea, anterior chamber, iris, ciliary body and anterior choroid [1]. The principal components of UBM are a hand piece with transducer, a computer console with the required hardware and specific software, a monitor, a printer and a foot switch. The UBM software provides a quantitative and qualitative assessment for the anterior segment. Sonographic data are generated along 512 lines; the signal is amplified, processed, converted from analog to digital format and transferred to a high speed scan converter, and eventually displayed on a video computer. According to the principles of ultrasound, high frequency and short focal length are associated with high image resolution and poor penetration. The patient is examined in a supine position with instillation of topical anesthesia. An eyecup is used to separate the eyelids and it is filled with a viscous, sono- lucent coupling fluid such as methylcellulose (1-2.5%) or normal saline. To detect a maximum reflected signal, the probe should be held in such way ultrasound beam strikes the target surface perpendicularly [1]. Probe orientation: The white line (or dot) on the side of the probe body indicates the direction of linear movement of the probe. For examining angles, the line should always point toward the cornea regardless of clock hour. When performing a Sulcus-to-Sulcus measurement the probe line will face the nose for the right eye and the ear for the left eye (Figures 1a & 1b).
![Figure 1: The probe orientation is marked by blue arrows. Figure 1a: the axial view of this case show the angle to angle width with shallow anterior chamber , closed angle and increased iridolenticular contact area. Figure 1b: The angle view with the structure of the normal angle; schwalb’s line (white arrow ) and scleral spur (the red arrow ). The most significant disadvantages of UBM are the need for immersion, the necessity of the supine position, and the need for patient cooperation during image acquisition. Recently, a disposable ultrasound probe covers eliminate the need for the supine position and insertion of a plastic shell during image acquisition [2]. Also, the Penetration depth of only 4-5 mm with Image quality that depends on plane of section, orientation of the probe, room illumination, fixation and accommodative effort, all may present minor inconveniences. In the normal eye, the cornea, anterior chamber, posterior chamber, iris, ciliary body, and anterior lens surface can be recognized easily (Figure 1b). The scleral spur is a landmark located where the trabecular meshwork meets the interface line between the sclera and ciliary body. The](/fulltextimages/2085/fig_1.jpeg)
Figure 1: The probe orientation is marked by blue arrows. Figure 1a: the axial view of this case show the angle to angle width with shallow anterior chamber , closed angle and increased iridolenticular contact area. Figure 1b: The angle view with the structure of the normal angle; schwalb’s line (white arrow ) and scleral spur (the red arrow ). The most significant disadvantages of UBM are the need for immersion, the necessity of the supine position, and the need for patient cooperation during image acquisition. Recently, a disposable ultrasound probe covers eliminate the need for the supine position and insertion of a plastic shell during image acquisition [2]. Also, the Penetration depth of only 4-5 mm with Image quality that depends on plane of section, orientation of the probe, room illumination, fixation and accommodative effort, all may present minor inconveniences. In the normal eye, the cornea, anterior chamber, posterior chamber, iris, ciliary body, and anterior lens surface can be recognized easily (Figure 1b). The scleral spur is a landmark located where the trabecular meshwork meets the interface line between the sclera and ciliary body. The
iris has a planar configuration with slight anterior bowing, and the anterior chamber angle is wide and clear. The present article is an updated mini-review regarding the use of UBM as one of anterior segment imaging devices, and also I report few selected cases to elucidate its usefulness Cornea: When there is corneal edema, the descmet’s detachment can be ruled out by UBM. Also, in opaque corneas the assessment of anterior chamber can be done prior to keratoplasty [3]. UBM can assess the depth of limbal tumor and helps to study the amount of infiltration of the cornea and sclera. (Figures 2a & 2b)
Glaucoma
Although gonioscopy remains the clinical gold standard for the diagnosis of narrow angles, UBM can assist in proper evaluation of glaucoma mechanisms such as pupillary block, plateau iris, phacomorphic glaucoma, and malignant glaucoma Differentiating these mechanisms is the key to provide effective treatment [4]. Common biometric parameters that are used in describing the anterior chamber such as angle opening distance, angle recess area, trabecular -iris space area, and trabecular- ciliary process area, iris thickness, iridolenticular contact distance . These values aid in the establishment of reproducible values for classifying the various subtypes of glaucoma [4, 5]. Pupillary Block with increased iridolenticular contact, resistance to aqueous flow from the posterior to the anterior chamber occurs , causing anterior iris bowing, angle narrowing, and acute or chronic angle-closure glaucoma [5] (Figure 3). A plateau iris configuration occurs owing to a large or anteriorly positioned ciliary processes which pushes the iris root mechanically up against the trabecular
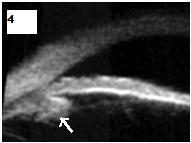
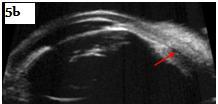
Figure 3: Mechanism of papillary pblock glaucoma with angle closure and anterior bowing of iris. Figure 4: Plateau iris with anterior insertion of iris into ciliary body and prominent ciliary process (white arrow). Phacomorphic glaucoma anterior subluxation of the lens may lead to angle-closure glaucoma. Because of the lens pushing the iris and ciliary body toward the trabecular meshwork (Figure 5a). Malignant Glaucoma: UBM clearly shows that iris lens diaphragm is displaced anteriorly with or without fluid in the supraciliary space (Figure 5b). In a recent study by Wang et al., the ciliary bodies were found to be thinner
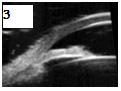
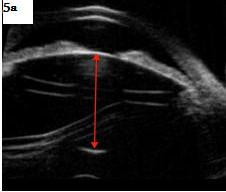
Figure 5a: Phacomorphic glaucoma with increased lens thickness (red arrow). Figure 5b: Malignant glaucoma after trabeculectomy with shallow anterior chamber, iris-lens diaphragm pushed anteriorly, thin ciliary body and supraciliary fluid (red arrow). Figure 5c: Secondary iris cyst after cataract extraction related to limbal wound causing displacement of the intraocular lens and occluding the angle with secondary glaucoma.
meshwork (Figure 4). With indentation gonioscopy, the “double hump” sign is observed [1]. In a study done by Mandell et al., they found that the AC depth was shallower than that of normal eyes and shallower than that of eyes with papillary block [6].
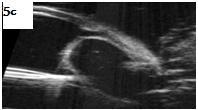
and more anteriorly rotated in the eyes with malignant glaucoma after trabeculectomy as compared to normal eyes [7]. Iridociliary Body Cysts: UBM can differentiate cystic from solid lesions of the iris and ciliary body. As well as, their size and posterior invasion of can be evaluated [3] (Figure 5c).
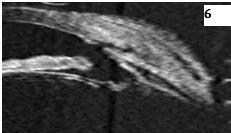
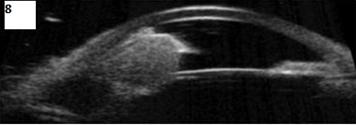
![Figure 8: Typical UBM findings in a pigment dispersion syndrome are a widely opened angle, posteriorly inserted iris with posterior bowing, and increased iridolenticular contact. Pseudo exfoliation syndrome is associated with a thick anterior lens capsule and disintegrated zonules with nodules. After Trabeculectomy, fluid-filled spaces can be identified in the subconjunctival and sub-Tenon's spaces above the level of the episclera denoting a functioning bleb [3] (Figure 6). **Uvietis:** UBM can assess the retrolenticular and retroiridal space and detect ciliary membranes in cases of chronic hypotony [8] (Figure 7).](/fulltextimages/2085/fig_8.jpeg)
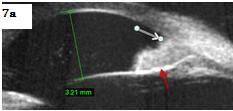
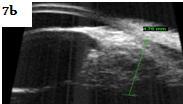
Figure 7: shows UBM findings in cases of uveitis. Figure 7a: Uveitis induced glaucoma with peripheral anterior synechiae (white arrow) and intact iris posterior pigmented epithelium (red arrow). Figure 7b: Ciliary body deposits and anterior vitreous deposits. Figure 7c: Numerous cells, peripheral anterior synechiae closed angle and iris granuloma with intact iris posterior pigmented epithelium. Marked oedema in the iris⁄ciliary body and numerous adjacent exu-dates. Marked oedema in the iris⁄ciliary body and numerous adjacent exu-dates.
Ocular Trauma: A retrospective study by Deramo et al. demonstrated that UBM could detect small intraocular foreign bodies <1 mm in size missed by CT and B scan. In addition, UBM has been shown to be an excellent method for identifying zonular damage, angle recession, iridodialysis, and rupture of the anterior lens capsule, lens displacement, lens subluxation, ciliary body detachment, hyphema, and traumatic cataract [9]. Ocular Tumors: Great advantage of UBM is assessing the intraocular invasion and metastasis although it cannot distinguish between melanocytic and metastatic lesion, so biopsy is always mandatory [10] Figure 8.
Typical UBM findings in a pigment dispersion syndrome are a widely opened angle, posteriorly inserted iris with posterior bowing, and increased iridolenticular contact. Pseudo exfoliation syndrome is associated with a thick anterior lens capsule and disintegrated zonules with nodules. After Trabeculectomy, fluid-filled spaces can be identified in the subconjunctival and sub-Tenon's spaces above the level of the episclera denoting a functioning bleb [3] (Figure 6). Uvietis: UBM can assess the retrolenticular and retroiridal space and detect ciliary membranes in cases of chronic hypotony [8] (Figure 7).
Finally, in this mini-review I present few cases to illustrate application of UBM as an anterior segment imaging device. Its technology has become an indispensable tool in qualitative and quantitative assessment of the anterior segment and beneficial in glaucoma, cornea, refractive, and even oculoplastic subspecialists. As it becomes more affordable, the examination becomes increasingly comfortable for patients, and practitioners gain greater familiarity with its potential applications, UBM will likely become more and more popular in comprehensive ophthalmology offices
References
-
Pavlin CJ, Harasiewicz K, Foster FS (1992) Ultrasound biomicroscopy of anterior segment structures in normal and glaucomatous eyes. Am J Ophthalmol 113(4): 381-389.
-
Bell NP, Feldman RM, Zou Y, Prager TC (2008) A New Technology for Examining the Anterior Segment by Ultrasonic Biomicroscopy. J Cataract Refract Surg 34(1): 121-125.
-
Deepak C Bhatt (2014) Ultrasound biomicroscopy: an overview. Journal of Clinical Ophthalmology and Research 2(2): 115-123.
-
Mannino G, Abdolrahimzadeh B, Calafiore S, Anselmi G, Mannino C, et al. (2016) A review of the role of ultrasound biomicroscopy in glaucoma associated with rare diseases of the anterior segment. Clin Ophthalmol 29(10): 1453-1459.
-
Chansangpetch S, Rojanapogpun P, Lin SC (2018) Anterior Segment Imaging for Angle Closure. Am J Ophthalmol 188: 16-29.
-
Mandell MA, Pavlin CJ, Weisbrod DJ, Simpson ER (2003) Anterior chamber depth in plateau iris syndrome and pupillary block as measured by ultrasound biomicroscopy. Am J Ophthalmol 136(5): 900‑903.
-
Wang Z, Huang J, Lin J, Liang X, Cai X, et al. (2014) Quantitative measurements of the ciliary body in eyes with malignant glaucoma after trabeculectomy using ultrasound biomicroscopy. Ophthalmology 121(4): 862‑869.
-
Ahmed AS, Biswas J (2013) Uveitis A search for a cause. Taiwan Journal of Ophthalmology 3(4):134- 140.
-
Deramo VA, Shah GK, Baumal CR, Fineman MS, Correa ZM, et al. (1998) The role of ultrasound biomicroscopy in ocular trauma. Trans Am Ophthalmol Soc 96: 355-365.
-
Bianciotto C, Shields CL, Guzman JM, Romanelli-Gobbi M, Mazzuca D, et al. (2011) Assessment of anterior segment tumors with ultrasound biomicroscopy versus anterior segment optical coherence tomography in 200 cases. Ophthalmology 118(7): 1297-1302.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report