The Effectiveness of Intravitreal Aflibercept in the Treatment of Neovascular Age-Related Macular Degeneration
Purpose: To evaluate the effectiveness of intravitreal aflibercept in neovascular age-related macular degeneration (AMD) patients followed in our clinic. Method: The examination file and optical coherence tomography (OCT) datas were investigated retrospectively. Patients divided into two groups according to previous therapies: patients received treatment before aflibercept (Group1) and started treatment with aflibercept (Group2). In Group2, patients were treated with pro-re-nata (PRN) regimen after 3 loading doses monthly. In Group1 patients were treated directly with PRN regimen after switching to aflibercept. Results: 154 eyes of 116 patients were enrolled. Average age of the patients were 75,2. The average follow-up duration was 39,01 months.The differences between the groups were statistically insignificant according to the sex,laterality of the eye and the post-aflibercept therapies (p>0,05). The number of aflibercept injections in Group 2 was significantly higher than Group1 (p0,05). In Group1,central and average macular thickness in post-aflibercept and last visits were significantly thinner than pre-aflibercept visit (p
Introductıon
AMD was firstly described in 1885 by Otto Haab as a disease which was characterized with pigmenter and atrophic changes in macula and progressive central vision loss in the patients over 50 [1]. The other name of the disease is senile macula degeneration. AMD is chronical and progressive disorder and in developed countries it is one of the major reasons of irreversible central vision loss in the population of over 50 [2, 3]. In 2030, it is expected that AMD will be the main reason of blindness by leaving behind diabetic retinopathy (DRP) and glaucoma in developed countries [4]. Clinically, there are two types of the disease: Dry and wet. Dry type is characterized with the loss of choriocapillaris and photoreceptors in addition to progressive RPE atrophy. It is also named as atrophic, nonneovascular or nonexudative type. On the other hand wet AMD is typical with the leakage and/or haemorrages derived from neovascular membranes to RPE and macula. That is why it is also called exudative or neovascular type. Although AMD is most commonly seen as dry form in routine practice, wet form is more relevant with vision loss [5]. On the contrary of dry form’s slow progression, a rapid and sudden vision loss occurs in wet AMD due to the fluid leakage and/or haemorrages from neovascular membranes [6]. It is expected that the prevelance of disease will increase with aging population [7]. Therefore numerous studies have been done on the treatment of wet AMD. Prior to photodynamic therapy (PDT), laser photocoagulation was performed for the treatment of wet AMD chronologically. However it was reported that laser laser photocoagulation wasn’t supposed to be performed anymore because not only it is beneficial in just %15 of patients according to the localisation and subtype of the lesion, but also it has a high iatrogenic central scotoma risk in subfoveal lesions [8]. PDT is the procedure of laser induced destruction of neovascular membranes in macula by reacting with verteporphine given into blood circulation peripherally and the main advantage of PDT is not damaging retina during procedure [9]. After PDT, antiVEGF agents were developed as the ultimate therapy in AMD and these agents were changed the neovascular AMD tretment principles deeply. Superiority of antiVEGF agents to PDT has been proven in AMD treatment [10]. Moreover antiVEGF agents avoid the final outcomes of disease like choroidal neovascularisation and vascular leakage [11]. These are the reasons why antiVEGF agents are currently accepted as “gold standart” modality of neovascular AMD treatment. As an antiVEGF agent, Pegaptanib was the first one produced and approved by American Food and Drug Administration (FDA) (2004) for intravitreal usage. Pegaptanib was followed by Ranibizumab (2006) and finally Aflibercept (2011) respectively. Bevacizumab was approved by FDA in february 2004 in metastatic colorectal cancer for intravenous usage. Although bevacizumab is off-label for intravitreal injection, it has been used quite widely especially in USA. Aflibercept is the ultimate antiVEGF agent and it was approved by FDA in 2011. It was declared as VEGF-Trap firstly because it can catch the circulating VEGF molecules like a trap. It can inhibite whole isoforms of VEGF and PIGF in intravitreal injection.
It is a fusion protein which was formed by the antigen binding parts of VEGF receptor 1, 2 and Fc part of IgG. Molecular formula of aflibercept is C₄₃₁₈H₆₇₈₈N₁₁₆₄O₁₃₀₄S₃₂. In the literature there are many studies about aflibercept showing its clinical and anathomical curative effect in the patients of AMD and PCV [12, 13, 14, 15, 16, 17]. Furthermore the number of these studies are increasing day by day. While some of these studies are including naive patients [12, 13]. some are including the ones received another treatment before [14, 15, 16, 17]. Metaanalysis including resistant cases also shows thatmorphological recovery and vision stabilisation were achieved after switching to aflibercept [18]. Distinctly, aflibercept is licensed to be performed with two-monthed intervals. Because aflibercept is the most recent antiVEGF agent, there has been numerous studies on it. Similarly, the purpose of this study was also determined the activity of aflibercept in the patients of neovascular AMD. In this study we aimed to evaluate the effectivity of aflibercept with VA and OCT outcomes in patients with neovascular AMD followed in our clinic.
Methods
The eyes received at least 1 intravitreal aflibercept injection due to neovascular AMD were enrolled to the study. There were no treshold value for VA and follow-up duration as an including criteria. Similarly phacic status of the patients were ignored. Neovascular AMD patients received no intravitreal aflibercept injection and non- neovascular AMD patients reveived intravitreal aflibercept injection were excluded. Polipoidal choroidal vasculopaty (PCV) patients and suspects were not seperated as a special subgroup. The study was realized retrospectively based on examination notes in patients’ files and OCT analyses. In every visit VA, full anterior and posterior segment examination and macula OCT were performed to all patients. If needed, FFA was used. VA was evaluated by optometrists or ophthalmologists and measured from 4 meters –and 2 meters or 1 meter in case- with Early Treatment Diabetic Retinopaty Study (ETDRS) chart.
VA values were converted into logMAR. TOPCON 3D 2000 was used for OCT and FFA imagination. While deciding the activity of disease; haemoragge next to the lesion in biomicroscopy, 5 letters or more loss of VA and existance subretinal or intraretinal fluid in OCT were regarded. Patients were divided into 2 groups according to their previous treatment history: The ones received any kind of treatment for exudative AMD (PDT, pegaptanib, bevacizumab, ranibizumab, triamcinolone) before aflibercept (Group 1)and the ones started treatment with aflibercept (naive patients) (Group 2). In group 2, patients were followed with pro-re-nata (PRN) regimen after 3 loading injections. In group 1, patients were followed directly with PRN regimen after switching to aflibercept. 2 mg of aflibercept were performed in whole intravitreal injections. Patients were followed up monthly or maximum bimonthly depending on clinical congestion. Demographic values of patients, previous therapies (type and number), VA before aflibercept, central and average macular thickness values befaore aflibercept, VA after aflibercept, central and average macular thickness values after aflibercept, VA in last visit, central and average macular thickness values in last visit and other therapies after aflibercept were noted carefully.
As the values of VA, central and average macular thickness after aflibercept, the values after 3 loading doses in group 2 and the values in first visit after aflibercept injection in group 1 were included. During follow up cataract surgery were recommended if clinically significant. Cataract surgery and aflibercept injection were performed at the same time in some cases. In definitive statistics of data; average, standart deviation, median, minimum value, maximum value, frequency and proportion value were used. Distribution of variable factors were measured with Kolmogorov-Simirnov test. Mann-Whitney U test as used for quantitative data. SPSS 22.0 programme was used for statistical analyze. Statistically significance value was p=0,05. This study was approved by ethical comittee.
Results
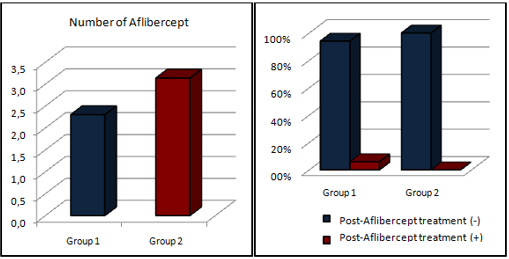
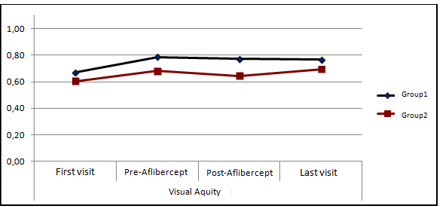
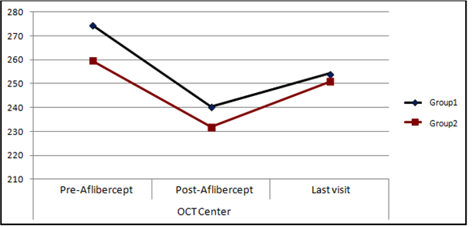
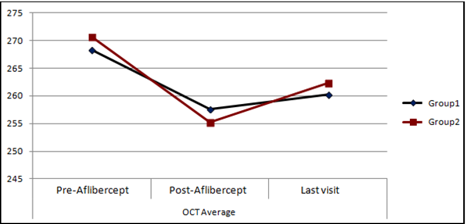
154 eyes of 116 patients were included to the study. In group 1 and 2 there were 118 eyes 93 patients and 36 eyes of 31 patients respectively. Average follow up period was 36,01 months (46,69 months[2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148, 149, 150, 151, 152]. in group 1 and 13,8 months [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77]. in group 2). In both groups there were no statistical significant difference in age, sex, laterality of the eye and treatment ratio after aflibercept injection (p>0,05). Average age in this study was 75,2 and 79 eyes were women’s, 75 eyes were men’s. Aflibercept injection number was significantly higher in group 2 than group 1 (p<0,05) (Table 1 & Figure 1). The most probable reason is loading dose factor of group 2. In Group 1 and 2, VA change weren’t significant in first, pre-aflibercept, post-aflibercept and the last visits (p>0,05) (Table 2 & Figure 2). In Group 1, VA values of pre-aflibercept, post-aflibercept and last visits didn’t change significantly in comparison with the VA values of first visit (p>0,05) (Table 2). In Group 2, VA values of pre-aflibercept, post-aflibercept and last visits didn’t change significantly in comparison with the VA values of first visit (p>0,05) (Table 2). In comparison with the first visit, changes of VA values in pre-aflibercept, post-aflibercept and last visits weren’t significant between two groups (p>0,05) (Table 2). In Group 1 and 2, central macular thickness values in pre- aflibercept, post-aflibercept and last visits weren’t significantly different (p>0,05) (Table 3 & Figure 3). In Group 1, central macular thickness values in post- aflibercept and last visits were significantly lower than pre-aflibercept visit (p<0,05) (Table 3). In Group 2, central macular thickness in post-aflibercept visit was significantly lower than pre-aflibercept visit (p<0,05). However the difference between the last visit and pre-aflibercept was not (p>0,05) (Table 3). In comparison with first visit, central macular thickness values in post-aflibercept and last visits didn’t significantly change between two groups (p>0,05) (Table 3). In Group 1 and 2, difference of average macular thickness values in pre-aflibercept, post-aflibercept and last visits weren’t significant (p>0,05) (Table 4 & Figure 4). In Group 1, average macular thickness values in post- aflibercept and last visits were significantly lower than pre-aflibercept visit (p<0,05) (Table 4). In Group 2, average macular thickness values in post- aflibercept and last visits were significantly lower than pre-aflibercept visit (p<0,05) (Table 4).
visits weren’t significant between two groups (p>0,05) (Table 4).
| Group 1 | Group 2 | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ave ± s.d./n-% | Me | d | Min-Maxi | Ave ± s.d./n-% | Me | d | Min-Maxi | p | |||||||||||||||
| Age | 75.2 ± 8.1 | 76 | 53 - 92 | 75.2 ± 7.8 | 77 | 54 - 89 | 0.819 m | ||||||||||||||||
| Sex | Female | 58 | 49.20% | 21 | 58.30% | 0335X2 | |||||||||||||||||
| Male | 60 | 50.80% | 15 | 41.70% | |||||||||||||||||||
| laterality | Right | 55 | 46.60% | 21 | 58.30% | 0.218X2 | |||||||||||||||||
| Left | 63 | 53.40% | 15 | 41.70% | |||||||||||||||||||
| Number of Aflibercept | 2 ± 1.3 | 2 | 1-7 | 3 ± 1.3 | 3 | 1-5 | 0.000m | ||||||||||||||||
| Post-Aflibercept (-) | 11 | 94.10% | 36 | 100% | 0.135x2 | ||||||||||||||||||
| Treatment (+) | 7 | 5.90% | 0 | 0.00% |
Table 1: Comparison of groups in terms of demographic data, number of aflibercept injections, treatments after aflibercept inject
| Group 1 | Group 2 | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | ||||||||||||||||||||
| Ave. ± s.d. | Med | Min-Maxi | Ave. ± s.d. | Med | Min-Maxi | |||||||||||||||
| Visual Aquity | ||||||||||||||||||||
| First visit | 0.67 ± 0.5 | 0.61 | -0.1 - 1.7 | 0.61 ± 0.5 | 0.48 | 0.1 - 1.7 | 0.53m | |||||||||||||
| Pre-Aflibercept | 0.79 ± 0.4 | 0.84 | 0.0 - 1.7 | 0.68 ± 0.5 | 0.50 | 0.1 - 1.7 | 0.212m | |||||||||||||
| Post-Aflibercept | 0.77 ± 0.4 | 0.82 | -0.2 - 1.7 | 0.64 ± 0.5 | 0.52 | 0.1 - 1.7 | 0.081m | |||||||||||||
| Last visit | 0.77 ± 0.4 | 0.74 | -0.1- 1.7 | 0.70 ± 0.4 | 0.65 | 0.1 - 1.7 | 0.381m | |||||||||||||
| Change in comparison with first visit | ||||||||||||||||||||
| Pre-Aflibercept | 0.11 ± 0.4 | 0.0 | -0.8 -1.3 | 0.08 ± 0.3 | 0.0 | 0.2 -1.5 | 0.789m | |||||||||||||
| Change p | 0.051 w | 0.061 w | ||||||||||||||||||
| Post-Aflibercept | 0.10 ± 0.4 | -1.2 - 1.2 | 0.04 ± 0.3 | 0.4 -1.5 | 0.314m | |||||||||||||||
| Change p | 0.051 w | 0.746 w | ||||||||||||||||||
| Last visa | 0.10 ± OA | -1.1 -1.5 | 0.09 ± 0.4 | 0.6-1.5 | 0.905m | |||||||||||||||
| Change p | 0.088 w | 0.321 w |
Table 2: VA changes in each group on table. m-Mann-whitney u Test; w-Wilcoxon test
| Group 1 | Group 2 | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | |||||||||||||||||||||||
| Ave. ± s.d. | Med | (Min-Max) | Ave. ± s.d. | Med | ( | Min-Max | ) | ||||||||||||||||
| OCT Center | |||||||||||||||||||||||
| Pre-Aflibercept | 274.5 ± 107.2 | 257 | 90 - 839 | 259.7 ± 87.1 | 250 | 119-487 | 0.443m | ||||||||||||||||
| Post-Aflibercept | 240.4 ± 105.7 | 227 | 49 - 719 | 231.8 ± 78.0 | 213 | 12 -522 | 0.843m | ||||||||||||||||
| Last visit | 254.2 ± 121.8 | 227 | 69 - 795 | 250.9 ± 99.2 | 219 | 97-522 | 0.952m | ||||||||||||||||
| Change in comparison with pre-aflibercept | |||||||||||||||||||||||
| Post-Aflibercept | -34.1 ± 110.2 | -21 | -676 | -25 | -281-315 | 0.717m | |||||||||||||||||
| Change p | 0.000 W | 0.048 | |||||||||||||||||||||
| Last visit | -20.2 ± 125.3 | 35 | -304 -484 | 8.8 ± 105 1 | -3 | -278 - 315 | 0.367m | ||||||||||||||||
| Change p | 0.017 w | 0.451 w |
Table 3: Changes of central macular thickness in each group on table. m-Mann-whitney u Test; w-Wilcoxon test
| Group 1 | Group 2 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P | |||||||||||||||||||||
| Ave. ± s.d. | M | e | d | Min-Max | ) | Ave. ± s.d. | Med | ( | Min-Max | ) | |||||||||||
| OCT Average | |||||||||||||||||||||
| Pre-Aflibercept | 268.3 ± 39.3 | 259 | 207 - 390 | 270.7 ± 35.0 | 269 | 189 - 354 | 0.379 | ||||||||||||||
| Post-Aflibercept | 257.6 ± 41.3 | 250 | 206 - 463 | 255.2 ± 29.4 | 252 | 213 - 338 | 0.866 | ||||||||||||||
| Last visit | 260.3 ± 45.9 | 249 | 187 - 536 | 262.3 ± 39.5 | 255 | 194 - 355 | 0.554 | ||||||||||||||
| Change in comparison with pre-aflibercept | |||||||||||||||||||||
| Post-Aflibercept | -10.7 ± 30.2 | -7 | -105-150 | -15.4 ± 28.3 | -13 | -98 - 84 | 0.166m | ||||||||||||||
| Change p | 0.00 w | 0.00 w | |||||||||||||||||||
| Last visit' | -8.0 ± 47.2 | -6 | -202 - 244 | -8.3 ± 41.7 | -13 | -104 - 158 | 0.452m | ||||||||||||||
| Change p | 0.00 w | 0.017 w |
Table 4: Changes of average macular thickness in each group on table. m-Mann-whitney u Test; w-Wilcoxon test
Dıscussıon
AMD is one of the main reasons of central vision loss and it is expected that AMD will be the most common reason of blindness in near future by excelling DRP and glaucoma [2, 3, 4]. Recetly, our knowledge in medicine has advanced prominently due to technological developments and many unknown points have been clarified. Thus average duration of human life has elongated and senility- related disorders have been seen world widely. Senility and senility-related disorders are the most important economical burden all around the world today and therefore they give direction to the health politics. AMD is one of the leading senility-related disorders and its incidance increses by age. According to a study, the prevelance of disease is %20 over 75 age [19]. Currently the population of over 75 age is more crowded than before owing to the technological developments. Therefore AMD is much more common clinical disorder in comparison with past. And it is obvious that it will affect much more people in the future than today.
Although AMD is more common in dry type in clinical practice, wet type is more related with vision loss. There is no current certain treatment for dry type. Because wet type is more responsible for vision loss, treatment modalities are more focused on characteristical lesion CNVM.
Vision loss in AMD is related with neovascularisation component of disease. Pathophysiologically, this is a kind of abnormal angiogenesis and the main point of angiogenesis is the imbalance between angiogenic and antiangiogenic factors. As neovascular AMD, DRP and retinopathy of premature are also angiogenesis-based disorders and abnormal vessel formation is prognostic in such disorders [20]. VEGF which is one of the strongest factor in angiogenesis is released from the cells in hypoxic-ischemic conditions, shows vigorous mitogenic activity on endothelial cells and increases vascular permeability [21]. It was showed that VEGF levels are high in blood circulation in AMD [22]. Therefore treatment of neovascular AMD is based on inhibition of VEGF today [23, 24]. For this purpose antiVEGF agents marked an era in treatment of wet AMD. Nowadays antiVEGF agents are golden standart in treatment. Not only the target molecule is known today but also it is showed that short-term activity of PDT is not valid in long-term, antiVEGF agents are indispensable for wet AMD. Similarly PDT is not recommended for treatment of AMD as monotherapy anymore. Clinical trials has stated that PDT is more convenient for combination with antiVEGF agents or in case of resistance to these agents [25, 26, 27, 28].
In a prospective study organized in Japan, it is reported that aflibercept recovered both VA and morphology at the end of 12 months in neovascular AMD and PCV [12]. In this study, aflibercept injections performed bimonthly after 3 loading doses. In another study using OCT angiography to evaluate the effect of aflibercept on macular anathomy in naive neovascular AMD patients, it is reported that aflibercept was related with significant changes in retinal-choroidal vascularity and decreased choroidal neovascularisation mostly [13]. In our study, Group 2 included naive patients and after 3 loading doses PRN regimen was performed to these patients instead of bimonthly constant intervals. Morphological recovery was seen with PRN regimen either. In comparison with pre- aflibercept visit, both in post- aflibercept and final visits average macular thickness was significantly thinner. On the other hand central macular thickness was significantly thinner in post- aflibercept visit than pre- aflibercept, however the difference wasn’t significant in final visit. We thought that the recurrens in final visit might be the reason of it. In naive patients VA was preserved but didn’t increase significantly. VA increase reported in the studies mentioned above might be due to fixed injection regimen. This method is taugh to perform because of its financial burden and ocular risks especially in congested clinics as ours.
There are clinical trials reporting the activity of aflibercept in not only naive patients but also resistant ones to other antiVEGF agents: It is reported in a study that a rapid morphological recovery and VA increase depending on the subtype of AMD after switching to aflibercept in neovascular AMD patients resistant to ranibizumab [14]. Another study evaluated the 12 monthed results of neovascular AMD patients resistant to 3 loading ranibizumab injections by dividing patients into PRN and fixed regimen groups. They reported that by the end of 12 months BCVA was steable in PRN group and significantly increased in fixed regimen group in comparison with first visit. However despite stabilised morphological parameters with both regimens, fixed regimen was emphisized as more effective with its significant BCVA increase. They also reported that pigment epithel detechment (PED) morphology had no significant change during 12 months in each group. Yet, they underlined the height of PEDs decreased some in comparison with beginning [15]. On the other hand, another study showed better morphological outcomes than functional outcomes in neovascular AMD patients switching to aflibercept.
In this study 96 eyes with neovascular AMD previously treated with ranibizumab and/or bevacizumab enrolled and 12 monthed outcomes of those eyes after switching to aflibercept were evaluated retrospectively. During follow- up it was seen that central macular thickness and axial PED lenght decreased significantly, the interval between injections increased, number of injections lessened and BCVA was steable [16]. In another study including ranibizumab resistant AMD patients, morphological and functional short-term changes after switching to aflibercept were evaluated prospectively . Significant BCVA incline, retinal thickness decline, shrinkage of the lesion regardless of subtype and dry macula in %64 of eyes were reported after monthly 3 loading doses in this study [17]. A meta-analyses about resistant neovascular AMD proved similarly retinal thickness decline and VA preservation after switching to aflibercept [18]. In our study Group 1 was comprising resistant cases especially to ranibizumab, and our results were also similar to these studies above morphologically. In Group 1, both central and average macular thickness values of post- aflibercept and final visits were significantly smaller than pre- aflibercept values. Differently, we did not investigate PEDs. On the other hand VA of these patients didn’t increase significantly but preserved in our study. Not only the injection regimen (PRN) but also permenant damage on retina due to chronical disease might be responsible of it. This morphological recovery of aflibercept can be explained with its high affinity for binding VEGF molecules more than other antiVEGF agents and its inhibitor effect on PIGF in addition to VEGF or antibodies against other previous antiVEGF agents.
The largest clinical trials about the activity of aflibercept in neovascular AMD are VEGF Trap-Eye Investigation of Efficacy and Safety in Wet AMD (VIEW) studies. VIEW1 and VIEW2 are similarly designed phase 3 studies. The efficacy of monthly and bimonthly intravitreal aflibercept injections were compared with monthly intravitreal ranibizumab injections in neovascular AMD. 2419 patients with CNVM secondary to AMD were enrolled to the study. Main outcome of the study was sustainability of VA (less than 15 letters loss) at 52nd week. In results, there were no significant difference between aflibercept and ranibizumab groups. According to BCVA change, morphological recovery and adverse events the results were similar between the groups. After 3 loading doses, outcomes of each group were similar, which means aflibercept was effective in treatment of neovascular AMD with no doubt even performed bimonthly [29]. It is remarkable that main superiority of aflibercept is its therapeutic vigorwith fewer injections. Because each injection brings not only financial burden but also ocular and systemical risks as haemmorage into vitreus, detechment of retina, elevated intraocular pressure, endophthalmitis, stroke and myocardial infarction.
In the study showing clinical results of aflibercept after 1 year in routine practice with VIEW protocole (3 loading doses and continueing bimonthly), the records of 16 centers were investigated retrospectively. 1840 naive eyes of 1682 patients were enrolled. Average number of injections and visits were 8 in 12 months. VA raised up to 58,8 letters from average 53,7 letters. The most important outcomes of the study were preserving VA increase in short term during whole year and reflecting real life results with an average 5,1 letters gain which was better than previous studies [30]. In the study showing the outcomes of 92 weeks of VIEW studies, the activity of aflibercept in exudative AMD after changing regimen in second year following a year with constant injection regimen was investigated. 2457 patients were enrolled to this study. Until 52nd week, after 3 loading injections monthly ranibizumab, monthly aflibercept and bimonthly aflibercept were performed. Between 52nd and 96th weeks original doses were performed with PRN regimen. At the end of this study it was reported that BCVA was preserved and VA of patients received 2 mg aflibercept bimonthly was similar to ranibizumab with 5 fewer injections [31]. The major outcome of this study is aflibercept can present VA loss with fewer injections in long term.
One of the handicaps of our study is that no further discrimination was performed in terms of phacic condition of the patients which could cause low VA in some patients with cataracts. If needed, combined cataracts surgery and intravitreal injection were performed together. Another handicap of the study was VA evaluation. Due to clinical congestion VA values were not BCVA. Therefore if patient had high refractive defect, his VA value could have been recorded smaller than real one. Again, due to congestion it took almost 1 month after injection decision to injection day. Hence some planned injections could have been disorganised. In some naive patients loading doses could not been completed because of patient-related reasons. Financial burden could also be another reason of it. Nevertheless in Group 2 number of injections were significantly higher than Group 1. On the other hand inequality of the groups was another handicap in the study. If the number of patients in each group were equal, the results would have let us comment more confidently in terms of statistics. Moreover the groups were not homogenous themselves because no further division was applied to the groups according to AMD subtypes. However when we checked the literature we realized that most of the studies about this issue had been organized also regarless of subtypes of AMD and the heterogenity had been ignored. For instance PCV patients which is also a subtype of exudative AMD, were not excluded in our study. Subtype analysis was not performed either, due to few number of patients. When we separetely investigated these PCV patients we saw that most of these patients showed temporary morphological recovery in short term. However after approximately 2 months, the basic disease relapsed. In terms of follow up period, there was a large range (2-152 months) in our study. Short follow up period affects the interval between post-aflibercept and final visits. Which means, in some patients’ final visit dates were a long time later than post- aflibercept visit while others’ were short.
It was unclear how much this situation affected the average. During the follow up it was decided that some patients had no benefit with aflibercept and therefore their antiVEGF therapy was altered to another agent. The number of these patients were few. Nevertheless these patients were not excluded. Hence this situation was another heterogenity factor in the study. Particularly in Group 1 the resistance to previous treatments, duration of disease and variable follow up were confounding factors and could have affected the results. Prior to aflibercept it was seen that treatment modalities had varied. For instance Group 1 was including both the patients received only 1 PDT and also the ones received numerous intravitreal injections in addition to PDT. We don’t know whether this heterogenity affected the results. VIEW studies showed that aflibercept is effective even bimonthly injections. However in VIEW studies original doses were performed at most 3 months even with PRN regimen [31]. Because of the congestion in our clinic antiVEGF therapy is performed with PRN regimen either. However there were some patients to whom intravitreal injections weren’t performed as late as 3 months. Furthermore it is hard to follow patients closely and it causes delay in antiVEGF therapy. All of these factors could have affected the results of our study. Because there is no consensus about the application of antiVEGF treatment regimen all around the world, it is stil unclear whether this situation affects the outcomes of present studies. It is a hard question to answer what “the most correct way” is, especially after aflibercept obtained good results even injected bimonthly.On the other hand our study is reflecting real life outcomes of long-term follow up in wet AMD and this is the most valuable side of this study.
Conclusion
Both central and average macular thickness values were smaller significantly after aflibercept in comparison with pre-aflibercept visit in previously treated patients. And in final visit this difference was maintaining. Both central and average macular thickness were lessened significantly after aflibercept in naive patients either and VA was preserved not only in short-term but also in long- term regardless of previous treatments. VA loss was avoided with aflibercept. So in treatment of exudative AMD aflibercept is an effective agent.
References
-
Haab O (1985) Erkrankungen der Macula Lutea. Centralbhat Augenheilkd 9: 384-391.
-
Wong TY, Chakravarthy U, Klein R, Mitchell P, Zlateva G, et al. (2008) The natural history and prognosis of neovascular age-related macular degeneration: a systematic review of the literature and meta-analysis. Ophthalmology 115(1): 116-126.
-
Klein R, Klein BE, Jensen SC, Meuer SM (1997) The 5 year incidence and progression of age related maculopathy: the Beaver Dam Eye Study. Ophthalmology 104(1): 7-21.
-
Rosenfeld PJ, Brown DM, Heier JS, David SB, Peter KK, et al. (2006) Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 355: 1419-1431.
-
Ferris FL 3rd, Fine SL, Hyman L (1984) Age-related macular degeneration and blindness due to neovascular maculopathy. Arch Ophthalmol 102(11): 1640-1642.
-
Kokotas H, Grigoriadou M, Petersen MB (2011) Age- related macular degeneration: genetic and clinical findings. Clin Chem Lab Med 49(4): 601-616.
-
Lindekleiv H, Erke MG (2013) Projected prevalence of age-related macular degeneration in Scandinavia 2012-2040. Acta Ophthalmol 91(4): 307-311.
-
Macular Photocoagulation Study Group (1993) Laser photocoagulation of subfoveal neovascular lesions of age-related macular degeneration: updated findings from two clinical trials. Arch Ophthalmol 111(9): 1200-1209.
-
Meyer CH, Lapolice DJ, Fekrat S (2005) Functions changes after photodynamic therapy with verteporfin. Am J Ophtalmol 139(1): 214-215.
-
Bressler NM, Chang TS, Fine JT, Dolan CM, Ward J, et al. (2009) Improved vision-related function after ranibizumab vs photodynamic therapy: a randomized clinical trial. Arch Ophthalmol 127(1): 13-21.
-
Brijesh T, Shorya A (2016) Macular Atrophy Progression and 7-Year Vision Outcomes in Subjects From the ANCHOR, MARINA, and HORIZON Studies: The SEVEN-UP Study. Am J Ophthalmol 162: 200.
-
Saito M, Kano M, Itagaki K, Sekiryu T (2017) Efficacy of intravitreal aflibercept in Japanese patients with exudative age-related macular degeneration. Jpn J Ophthalmol 61(1): 74-83.
-
Mastropasqua L, Toto L, Borrelli E, Carpineto P, Di Antonio L, et al. (2017) Optıcal Coherence Tomography Angıography Assessment of Vascular Effects Occurrıng after Aflıbercept Intravıtreal Injectıons in Treatment-Naıve Patıents wıth Wet Age- Related Macular Degeneratıon. Retina 37(2): 247- 256.
-
Hirakata T, Fujinami K, Watanabe K, Sasaki M, Noda T, et al. (2016) One-year outcome of intravitreal aflibercept injection for age-related macular degeneration resistant to ranibizumab: rapid morphologic recovery and subsequent visual improvement. Clin Ophthalmol 10: 969-977.
-
Ricci F, Parravano M, Regine F, Sciamanna M, Tedeschi M, et al. (2016) Aflibercept in persistent neovascular AMD: comparison of different treatment strategies in switching therapy. Eye (Lond) 30(8): 1077-1083.
-
Pfau M, Fassnacht-Riederle HM, Freiberg FJ, Wons JB, Wirth M, et al (2016) [Switching Therapy from Ranibizumab and/or Bevacizumab to Aflibercept in Neovascular Age-Related Macular Degeneration (AMD): One-Year Results]. Klin Monbl Augenheilkd 233(8): 945-950.
-
Abri Aghdam K, Seidensticker F, Pielen A, Framme C, Junker B (2016) The short-term effects of aflibercept on the size of choroidal neovascularization lesion in treatment-resistant neovascular age-related macular degeneration as determined by spectral-domain optical coherence tomography. Lasers Surg Med 48(7): 668-677.
-
Seguin-Greenstein S, Lightman S, Tomkins-Netzer O (2016) A Meta-Analysis of Studies Evaluating Visual and Anatomical Outcomes in Patients with Treatment Resistant Neovascular Age-Related Macular Degeneration following Switching to Treatment with Aflibercept. J Ophthalmol pp: 1-8.
-
Sperduto RD, Hiller R (1986) Systemic hypertension and age-related maculopathy in the Framingham Study. Arch Ophthalmol 104(2): 216-219.
-
Jampol LM, Ebroon DA, Goldbaum MH (1994) Peripheral proliferative retinopathies: An update on angiogenesis, etiologies and management. Surv Ophthalmol 38(6): 519-540.
-
Distler O, Neidhart M, Gay RE, Gay S (2002) The molecular control of angiogenesis. Int Rev Immunol 21(1): 33-49.
-
Sharma K, Sharma NK, Singh R, Anand A (2015) Exploring the role of VEGF in Indian Age related macular degeneration. Ann Neurosci 22(4): 232-237.
-
Oester A, Baffi J, Ambati BK (2008) Pharmacotherapy targeting ocular neovascularization. Focal Points XXVI: 1-10.
-
Yalçınbayır O, Firozvi A, Akduman L (2005) Makula dejeneransı tedavisinde yeni bir dönem başlıyor. Ret- Vit 13: 1-7
-
Silva-Garcia R, McLellan C, Shaya FS, Small KW (2014) Long-lasting effects of anti-VEGF/photodynamic combination therapy in the treatment of exudative age-related macular degeneration: a retrospective chart review. Clin Ophthalmol 8: 2529-2532.
-
Kaiser PK, Boyer DS, Cruess AF, Slakter JS, Pilz S, et al. (2012) Verteporfin plus ranibizumab for choroidal neovascularization in age-related macular degeneration: twelve-month results of the DENALI study. Ophthalmology 119(5): 1001-1010.
-
Larsen M, Schmidt-Erfurth U, Lanzetta P, Wolf S, Simader C, et al. (2012) Verteporfin plus ranibizumab for choroidal neovascularization in age-related macular degeneration: twelve-month MONT BLANC study results. Ophthalmology 119(5): 992-1000.
-
Costa RA, Jorge R, Calucci D, Melo LA Jr, Cardillo JA, et al. (2007) Intravitreal bevacizumab (Avastin) in combination with verteporfin photodynamic therapy for choroidal neovascularization associated with age- related macular degeneration (IBeVe Study). Graefes Arch Clin Exp Ophthalmol 245(9): 1273-1280.
-
Heier JS, Brown DM, Chong V, Korobelnik JF, Kaiser PK, et al. (2012) VIEW 1 and VIEW 2 Study Groups. Intravitreal aflibercept (VEGF trap-eye) in wet age- related macular degeneration. Ophthalmology 119(12): 2537-2548.
-
Talks JS, Lotery AJ, Ghanchi F, Sivaprasad S, Johnston RL, et al. (2016) First-Year Visual Acuity Outcomes of Providing Aflibercept According to the VIEW Study Protocol for Age-Related Macular Degeneration. Ophthalmology 123(2): 337-343.
-
Schmidt-Erfurth U, Kaiser PK, Korobelnik JF, Brown DM, Chong V, et al. (2014) Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology 121(1): 193-201.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report