Foster Kennedy Syndrome: About 2 Cases
We relate 2 patients cases whose age are 32 and 35 years affected by Foster Kennedy’s syndrom during a 10 years period in Brazzaville (Congo) Teaching Hospital. These two patients had progressive bilateral low visual acuity, papillary edema in one eye and optic atrophia in another one, in link with pituitary tumor. For all cases, betamethazone-based treatment associated to acetazolamid in bolus by intravenous infusion and per os route has been set up.15 days later we have observed a decline of the papillary edema and the stability of vision acuity. The syndrom of Foster Kennedy is scarcely revealed into the african’s literature, the etiological diagnosis refers to computed tomography scan and especially brain magnetic imaging resonance. The etiological treatment remains essential and the prognosis depends onto it.
Introduction
The syndrom of Foster Kennedy is a symptom of expansive and compressive process of the anterior cranial fossa which induce a mass effect on tissus and surrounding neurosensory tracts [1]. It is typically characterized by bilateral papillaries anomalies as a papillary atrophia homolateral to the lesion and stasis papillary in the contrary side of the lesion in inconstant association with anosmia. It has been described by numerous of authors such as: William Gower in 1893, Schultz-Zehden in 1905, Foster Kennedy in 1911 in USA then later the depiction done by Willehm Uhthoff in 1915.Regarding the importance of this syndrome caused by cerebral tumor, we relate 2 clinical cases found during a period of 10 years in Brazzaville(Congo) Teaching Hospital.
Goal
Underlining the interest of cerebral imaging accessibility in the diagnosis and neurosurgical treatment of brain tumors.
Observation
First Case
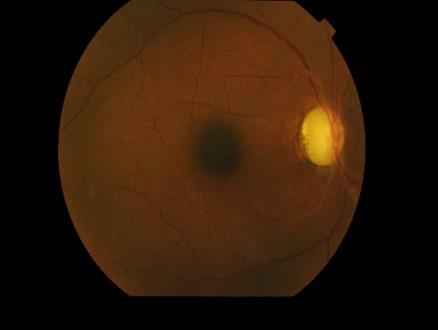
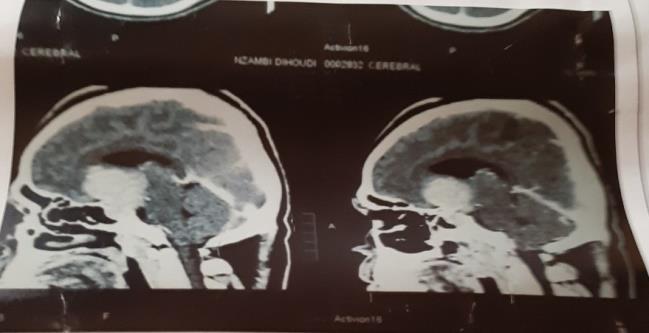
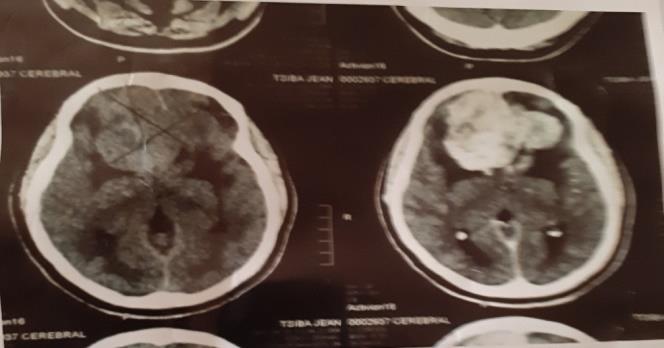
KL, 32 years old, female, visited for the very first time the ophtalmologist. The onset of the illness comes back up about 4 years, by a progressive bilateral low visual acuity, relapsing cephalagias despite taking some antalgic pills of the first stage, and amenorrhea. During sight exam, we notice on the right eye a low visual acuity quoted 1/10 testifying a papillary edema Stage III, and on the left one, low light reception showing an optic atrophia (Figure 1). Neurologic exam is normal. We notice in gynecologic exam an amenorrhea without galactorrhea. The cerebral scan objectified a giant sellar tumor with agressive appearance, extensive through the left temporal lobe with bone lysis (Figures 2&3).

Second Case
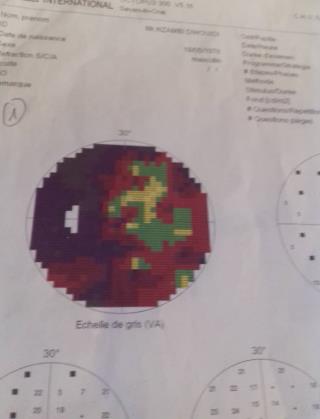
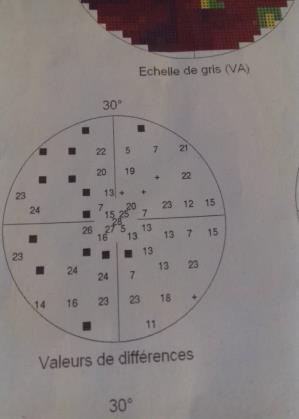
ND, 35 years old, male, with no particular ophtalmologic past record, consults for progressive bilateral low visual acuity during 12 months preceded by a bilateral amaurosis. During the sight exam, we notice on the right eye a low visual to the light perception in keeping with an optic atrophia, on the left eye, a low visual acuity quoted 4/10 in link with a papillary edema stage II (Figure 4). The visual field is off on the right, and it was existing a left nasal heminanopsia (Figure 5). An anosmia has been revealed and neurologic exam was normal. The Scanner showed a hypophyseal tumor which avokes a giant hypophyseal adenoma (Figure 6).

For these both cases betamethazone-based medical treatment in bolus associated to acetazolamid intravenous infusion and per os route, has been set up while we wait for the intervation of the neurosurgical and anatomopathologist results. 15 days later we have observed decline of the papillary edema and stability of vision acuity. Patients have been lost touch for social and economic reasons.
Discussion
Foster Kennedy’s syndrom is scarcely brought in the african’s literature. It prevalence in relation with hypophyseal adenoma is estimated from 0.02 up to 0.1% according to some authors [2]. If the clinical examination is evocative of an endocranial process, the etiological diagnosis refers to computed tomography scan (CT-scan) and espacially the brain magnetic imaging resonance (MRI) that provides the best details and constitutes a privilege study [3], a test to determine homone rate and anatomopathology. The contrast administration within imaging is intemately linked to the level of the endothelio- capillary hyperplasia. The diversity of causes shows that in the 45% of cases we find gliomas, from 10 to 15% we find adenomas, in 15% we have meningiomas and also 15% of neurinomas. The treatment refers precociously to corticoids and carbonic anhydride which proving effecient for intracranial high pressure and papillary edema as noted by Liang and Co [4]. However the etiological treatment remains essential and the prognosis depends on it. Precisely with appropriate drugs when the tumor is chemosensitive or by a total surgical extraction or partial one, coupled with radiotherapy or radiotherapy itself. The medical imaging is compulsory for treatement control.
Conclusion
The syndrom of Foster Kennedy is a complex desease. The availability of diagnosis measures, treatement and they accessibility are worrying for the Congolese people and most black African countries.
References
-
Kennedy F (1911) Retrobulbar neuritis as an exact diagnostic sign of certain tumors and abscesses in the frontal lobes. Am j Med Sci 142: 355-368.
-
Ezzat S, Asa SL, Couldwell WT, Barr CE, Dodge WE, et al. (2004) The prevalence of pituitary adenomas: a systematic review. Cancer 101(3): 613-619.
-
Jarus GD, Feldon SE (1982) Clinical results and tomography in Foster Kennedy’s syndrom. Am Ophthalmol 93(3): 317-322.
-
Liang F, Offret H (2007) Foster Kennedy’s syndrome: about one case. Jfo 30(2): 2S318.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report