Argon Laser as a Treatment of Trichiasis in Alwahda Teaching Hospital-Derna, Libya
Trichiasis is a medical term for abnormally positioned eyelashes that grow back toward the eye, touching the cornea or conjunctiva. Trachoma is the main Couse of Trichiasis which remains an important cause of blindness and the leading preventable cause of visual disability. Data from several surveys have indicated that trachoma is rapidly waning as a highly endemic disease. This prospective study to introduce the argon laser in treatment of Trichiasis in teaching Alwahda hospital in Derna city eastern part of Libya. Were 50 eye lids from 40 Libyan patients, the results were 90% success.
Purpose
Argon laser photocoagulation intervention is also preventable and curable treatment from Trichiasis and improve of visual outcome.
Back Ground
Trichiasis are among the leading causes of visual loss and visual impairment in the eastern Mediterranean countries, this sometimes results in serious ocular squeal such as keratopathy, corneal ulcers, and corneal opacity [1] which can be improved by modulating its treatment. New intervention techniques such as argon laser have been adopted in certain cities in the Middle East. The use of the Argon laser to treat Trichiasis was first reported in the literature in 1979 by Berry [2]. Since then little attention seems to have been paid to the topic until recently when a paper appeared by Awan and the report of an interview on technique by Pannu [3].
Even today Trichiasis remains a therapeutic challenge. Irrespective of etiology, Trichiasis is usually associated with corneal and conjunctival irritation, which if severe enough may lead to corneal ulceration and scarring and eventually result in impairment of vision [4]. Although a number of different modalities of treatment are in wide use today, namely mechanical epilation, electrolysis, cryotherapy and surgery, none is completely effective on its own and all have drawback [5].
Electrolysis is tedious and difficult to perform, requiring infiltration anesthesia and specialized equipment. When large areas are treated it can produce scarring and result in entropion formation [6]. Recurrence following treatment is reported of the order of 30% to 50% [7, 8]. Cryotherapy is currently considered the most effective method of treatment in widespread use, especially where large numbers of lashes are involved [8, 9]. Cure rates of 71% to 90% are reported in the literature but this procedure is also associated with a high complication rate, reported as being 26% by Wood and Anderson. Complications of cryotherapy include severe lid edema, lid depigmentation, lid notching, corneal ulceration, preseptal cellulitis, and induction of Trichiasis, acceleration of symblepharon formation, reactivation of herpes zoster, xerosis and visual lOSS [10]. Surgical techniques in use include wedge resection; these procedures can be difficult to perform, time consuming and can result in further scarring and impairment of lid function [5, 9]. If the lashes do recur, the options include repeated removal at the slit lamp every 4-6 weeks or permanent lash removal. There are several methods for permanent lash removal, and the best method is determined for each individual patient based on the location and number of misdirected lashes. Untreated, it can potentially become a serious problem. However, with prompt diagnosis and proper treatment, Trichiasis can be effectively managed without any permanent damage to the eye or to the vision.
Methods
Planning was discussed eligible population manpower logistics requirement was taken into consideration, Including eligible patients, ethical issues and time frame was discussed and the agreement was obtained after detailed discussion with the patients about the aim, objectives and methodology of the study. Detail history for every patient taken include paste medical and surgical history, the etiology of Trichiasis was determined whenever possible. Examine of 40 patients we found 50 eyelids with Trichiasis. The standard technique for laser therapy was performed under clean but not sterile conditions, every patient was followed up monthly during the for 5 months, any patient had recurrent one or more eye lashes had retreated by argon laser and this repeated for three session. And those Recurrences one or more eye lashes after 3ed session after treatment by same laser parameter considered failed. The laser parameters were 1 watt power, for 0.20 seconds, with 100 micrometer beam diameter, this low dose was just for remarkable the area or the site of origin the eye lash exactly then increase the power to 1.2 watt power, for 0.20 seconds, with 200 micrometer beam diameter to go deep to reach and destroy the follicle of eye lashes. An antibiotic-corticoid ointment was used t.i.d. for a week after each laser treatment session.
Results
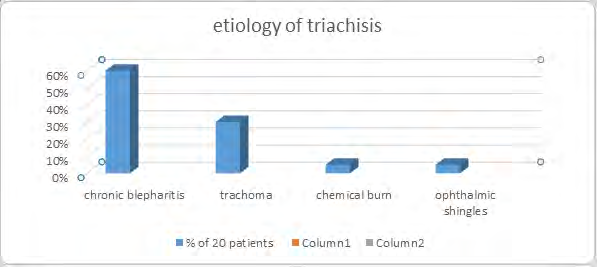
Forty patients, a total of 50 eyelids, were treated with the argon laser. 40% of the patients were females. The average age was 50 years old. The etiological factor is found in 20 of our patients (50%), {(chronic blepharitis (60 %), trachoma (30%), chemical burns (5%), and ophthalmic shingles (5%))). 20 patients (50%) no cause was found (Figure 1).
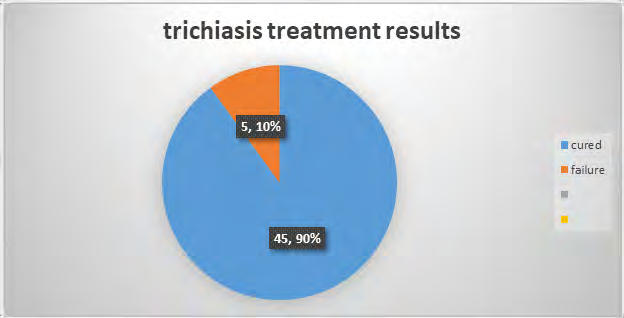
The patients were seen in the clinic and the presence or absence and number of lashes was noted. A total of 45 eyelids, the overall success rate for abolition of aberrant lashes were 90% the recurrence rate was 10%, there were two patients who developed aberrant eyelashes in areas that had not previously been treated. These were not considered to be either recurrences or complications (Figure 2).
Recurrence or failure was 5 eyelids after a maximum of 3 sessions of Laser treatment. The treatment has been repeated with the same protocol for the recurrence cases.
Discussion
Eye diseases affecting the cornea are major causes of blindness worldwide. In some area of Africa as much as 90% of all blindness is a direct result of corneal pathology. The message is clear that early preventive medical and surgical intervention urgent needed to eliminating corneal blindness in developing country. Treatment of trichiasis has always been a difficult therapeutic problem. Many modalities of therapy have been tried with variable rates of success. These include epilation after which rubbing lashes invariably recur; electrolysis which has not been fully successful in the past [11].
If left untreated it can lead to corneal ulceration, vascularisation, hypoethesia and can predispose to infectious keratitis. For temporary relief, the eyelashes can be plucked out (called epilation), but they usually grow back. For more severe cases and for recurrent disease, may recommend permanent removal of only the affected eyelash follicles using a special device. The optimal management of minor trichiasis (<6 trichiatic lashes) is controversial. The WHO advises lid rotation surgery for all trachomatus trichiasis patients irrespective of severity, even if only 1 peripheral lash touches the eye [12].
Epilation, cryotherapy, and eyelash hair follicle removal are all utilized in the treatment of trichiasis .However, many ophthalmologists and some trachoma control programs advise epilation for minor trichiasis. There are no reported trials comparing surgery and epilation, argon laser therapy, and a randomized, controlled trial addressing this question would be useful .The results of our study were encouraging and demonstrated the successful use of the Argon laser to treat selected cases of trichiasis. The most recent paper on this topic by Awan KJ, et al. [13]. Reported a 90.3% cure rate treating 31 patients who were followed up from three months to two years. Various results have been reported for the treatment of trichiasis with the argon laser. Compbell reported 33% success rate after the first session, and 80% after three LASER sessions [14]. Argon laser treatment of trichiasis is a safe, effective procedure which allows more precise placement and control of the treatment with minimal cicatrization. Thus repeated laser treatment can be performed with little fear of inducing significant scarring. Accordingly Argon laser ablation of maldirrcted eyelashes is preferred in trichiasis associated with cicatrizing conditions. Moreover, Argon laser treatment is found to be efftxtive especially when few fine cilia are involved but repeated treatment is required for more and thicker cilia. The major drawback of Argon laser treatment is that it is costly. As the initial results of Argon laser treatment for trichiasis are promising, so more studies with a larger number of patients are needed for proper evaluations of the procedure. Moreover, other types of laser may be tried which may prove to be more effective .While Sharif et al reported 67.9% success for 21 patients after approximately two consecutive laser sessions and stated that the number of aberrant lashes per lid dictated the number of treatment sessions required [15]. The Argon laser seems to be a suitable alternative to treat small numbers of trichiatic lashes whether they are isolated, located in a cluster or recurrent following treatment with other modalities. The main advantages of the laser are precision and selectivity of application, apparent lack of complications, non-requirement for infiltrative anesthesia and the relative ease with which the technique can be performed. These days Argon lasers are readily available in most ophthalmology centres in Libya. The main disadvantages are that repeat treatment may be required in order to obtain a successful result. The follicles of cilia are normally located 1.5 to 2.5 mm below the surface [16]. In order for treatment to be successful the lash follicle needs to be completely destroyed and for Thermo ablation treatment for trichiasis using the argon laser 429 that reason the depth and direction of the crater are important. It was noted that in some patients a few lashes regrew but were no longer misdirected and all were attenuated. This suggested that partial destruction of the follicle had occurred and that scarring around the follicle may have caused it to reorientate. Therefore care needs to be taken when treating aberrant cilia close to normal follicles to avoid excess tissue destruction which could induce trichiasis. In the future, the Argon laser may become an important alternative modality to treat Trichiasis in selected patients, but other research still needs to be done into the technique to determine the ideal laser factors (i.e. exposure time, spot size, wavelength and power) and the optimum amount of treatment. In extreme cases, may be the only option if abnormal eyelash growth and eye infections become recurrent or involve a multitude of eyelashes, leaving a constant discomfort. Surgical rotates the eyelid around to its normal alignment and uses strategically placed stitches to keep it in its proper place. This is another expensive treatment option, although it is a permanent cure for ingrown eyelashes.
Conclusion
The result of this study was expected to be positive, but we did not expect it to reach a rate of 90%, this good result is an indicator that encourages to give superiority to treatment of trichiasis with argon laser Al-Wehda Teaching Hospital Derna. Not just factor of the result take in consideration but also due to the ease of procedure and the side effects were very mild comparing to such as other treatment methods. There are several factors that will be proposed for research that may interfere and affect the outcome of the treatment, such as the dose of laser , number of sessions and power of each session, the patient’s age, and also the main underlying couses of the trachiasis, all that needs to be studying in detail in the near future.
References
-
Choo P (2002) Distichiasis, Trichiasis, and Entropion: Advances in Management. Int Ophthalmol Clin 42(2): 75-87.
-
Berry J (1979) Recurrent trichiasis: treatment with laser photocoagulation. Ophthalmic Surg 10(7): 36-38.
-
(1988) Argon laser treatment for trichiasis. Ocular Surgery News 6(22): 22.
-
Hartzler J, Neldner KH, Forstot LS (1984) X-ray epilation for the treatment of trichiasis. Arch Dermatol 120(5): 620-624.
-
Collin JRO, Coster DJ, Sullivan JH (1978) Cryosurgery for trichiasis. Trans Ophthalmol SOC UK 98(1): 81-83.
-
Sullivan JH, Beard C, Bullock JD (1976) Cryosurgery for treatment oftrichiasis. Am J Ophthalmol 82(1): 117-121.
-
Sullivan JH, Beard C, Bullock ID (1976) Cryosurgery for treatment of trichiasis. Trans Am Ophthalmol SOC 74: 189-202.
-
Hecht SD (1977) Cryosurgery of trichiasis with use of the retinal cryoprobe. Am J Ophthalmol 9(12): 1501-1503.
-
Johnson RL, Collin JR (1985) Treatment of trichiasis with a lid cryoprobe. Br J Ophthalmol 69(4): 267-270.
-
Wood JR, Anderson RL (1981) Complications of Cryosurgery. Arch Ophthalmol 99(3): 460-463.
-
Fox I (1970) SA: Ophthalmic surgery, 4th (Edn.), New York, Grun Stratton pp: 330-335.
-
(2011) Trachoma control: a guide for programme managers. World Health Organization.
-
Awan KJ (1988) Laser photocoagulation-vaporization therapy of trichiasis. Ophthalmic laser therapy 3: 3-9.
-
Campbell DC (1990) Thermoablation treatment for trichiasis using the argon laser. Aust NZ J Ophthalmol 18(4): 427-430.
-
Sharif KW, Arafat AFA, Wykes WC (1991) The treatment of recurrent trichiasis with argon laser photocoagulation. Eye 5: 591-595.
-
Duke ES, Wybar KC (1961) Anatomy of the Eye-In: System of Ophthalmology. St Louis 2.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report