Evisceration Decision as a Primary Surgical Intervention: Why and When?
Purpose: To evaluate indications of patients to whom evisceration was performed as a primary surgical intervention in a tertiary eye center. Methods: Patients who underwent evisceration as a primary surgical intervention between years 2016-2021 were retrospectively analyzed. The patients were classified into 2 groups in terms of corneal perforation presence and these groups were divided into 4 subgroups according to presence of trauma and infection: Traumatic infectious or non-infectious and nontraumatic infectious or non-infectious causes. Results: A total of 20 eyes of 20 patients who underwent evisceration as a primary surgical intervention were recorded. The mean age was 70.45±3.99 (36-90) with a female/male ratio of 9/11. Light perception was absent in most of the eyes (14 patients). Standard surgical procedure was performed under general anesthesia and orbital implants were placed in 6 of 20 patients, who had no infectious situation. Primary evisceration was performed predominantly to patients with corneal perforation (15/20). Subgroups of these cases included penetrating injuries (2/20), microbial keratitis with corneal perforation (7/20), and non-infectious corneal perforation (6/20). In 5 of 20 cases without corneal perforation owing to uncontrolled infectious pathologies [endophthalmitis (2/20), microbial keratitis (3/20)] primary evisceration was performed. Post-operatively, standard medical treatment was ordered, and no surgical complications were observed. Conclusion: Ophthalmic surgeons tend to postpone evisceration surgery due to its brutal nature. Clinicians may perform the procedure as a primary surgical intervention in selected cases. In conclusion, surgeons should think wisely and consider the benefit and damage balance when deciding to perform evisceration surgery as a primary intervention.
Introduction
Evisceration surgery is one of the most frequently performed destructive ocular surgeries [1]. Main indications of globe evisceration include a severely traumatized globe, painful blind eye, phthisis bulbi, secondary glaucoma, refractory infections (e.g., endophthalmitis and keratitis) that do not respond to medical treatment, and other miscellaneous causes [2, 3]. Due to its brutal nature, ophthalmic surgeons do not prefer to perform primary evisceration unless there is a devastating situation. Nevertheless, there are some situations, such as elderly debile patients with infectious or traumatic corneal perforations, that clinicians should evaluate the potential benefit of reconstructive surgeries and might decide on evisceration surgery as a primary surgical intervention [4]. In the present study, it was aimed to determine the indications of evisceration as a primary surgical intervention in a tertiary eye center.
Materials and Methods
Patients who underwent evisceration as a primary surgical intervention between years 2016-2021 were retrospectively evaluated. Medical data including demographic information, clinical history, and primary clinical diagnosis, detailed ophthalmological findings at presentation, initial best corrected visual acuity (BCVA), the main cause of surgery, surgical and medical treatments before surgery, and post-operative complications were reviewed. The patients were classified into 2 groups in terms of corneal perforation presence, and these groups were also divided into 4 subgroups according to the presence of trauma history and infection: traumatic infectious or non-infectious and non-traumatic infectious or non-infectious causes. The study was approved by the Institutional Ethics Review Board of Ege University and was conducted in agreement with the tenets of the Helsinki Declaration. Statistical analysis was performed by using the IBM SPSS Statistics 25.0 package program (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). Results were reported as mean standard deviation (SD) for quantitative variables and number and percentage for categorical variables.
Results
A total of 20 eyes of 20 patients who underwent evisceration as a primary surgical intervention were recorded. The mean age was 70.45±13.99 (36-90) with a female/male ratio of 9/11. Light perception was absent in most of the eyes (14 patients). Visual acuity could not be measured in one unconscious patient with corneal perforation with extrusion of intraocular contents who was hospitalized in intensive care unit. Light perception (4 patients), and hand motion (1 patients) were present in the rest of the eyes. Standard surgical procedure was performed in all patients under general anesthesia and orbital implants were placed in 6 of 20 patients, who had no infectious situation. Indications for evisceration as a primary surgical intervention were summarized in (Table 1). Primary evisceration was performed predominantly in patients with corneal perforation (75.0%). The most common subgroup among these patients was recorded as the non-traumatic infectious group (7, 35.0%).
| Age; mean ± SD (range) | 70.45± 13.99 (36-90) | |
|---|---|---|
| Gender (male / female ratio) | 9/11 | |
| Patients with Corneal Perforation | Penetrating /Perforating Injury | 2 (10.0%) |
| (15;75%) | Non-Traumatic Infectious Group | 7 (35.0%) |
| Non-Traumatic Non-Infectious Group | 6 (30.0%) | |
| Patients without Corneal Perforation | Microbial Keratitis | 3 (15.0%) |
| (5; 25%) | Endophthalmitis | 2 (10.0%) |
Table 1: Demographic data and indications of evisceration surgery as a primary intervention.
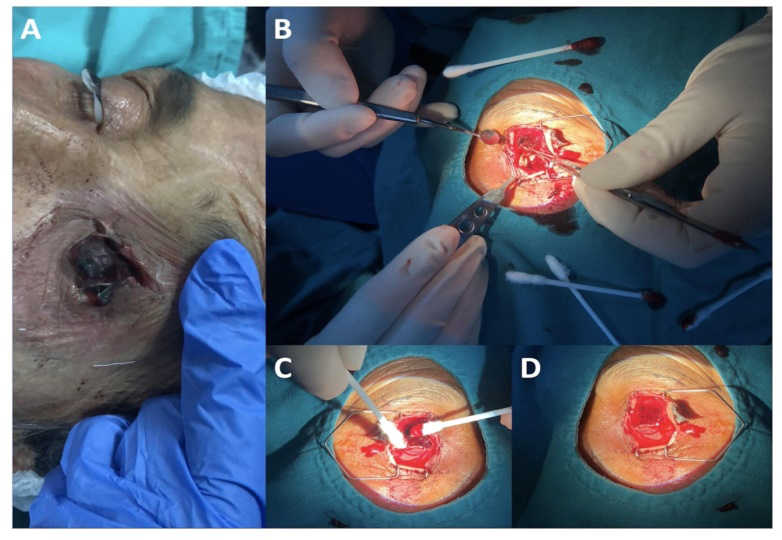
Primary evisceration surgery performed in 60% of all patients due to infectious etiologies. A total of 41.6% (3 microbial keratitis, 2 endophthalmitis) of these patients were uncontrolled microbial infections without spontaneous perforation. All microbial keratitis patients who underwent primary evisceration surgery were culture positive (1 patient Basillus spp, 1 patient H. influenzae non type B, and 3 patients S. pneumoniae, 2 patients Fusarium spp, 1 patient Stenotrophomonas maltophilia and Haemophilus influenzae non type B). Most of the patients (14/20) were 70 years or older. In 2 ocular penetrating trauma patients (traumatic non-infectious group), evisceration surgery was performed as a primary surgical intervention. One of these patients was hospitalized in the intensive care unit in whom the procedure was performed at the bedside. The other patient was a 90-year-old female, diagnosed with Alzheimer’s disease, injured by self-mutilation who had no caregivers (Figure 1).
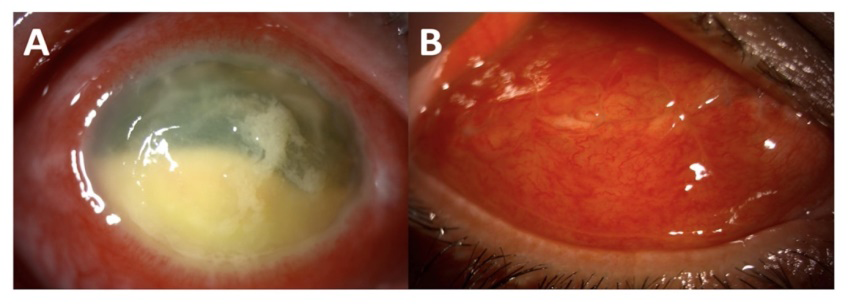
Likewise, non-traumatic infectious (4 patients) or non- traumatic non-infectious causes (6 patients) were mostly debile, elder age, with low self-care, without caregivers (Figure 2).
Uncontrolled ocular infection was present in 2 patients with general physical health deterioration. Post-operatively, standard medical treatment as topical tobramycin (Tobrased® %0.3 ophthalmic pomade, Bilim Inc., Istanbul, Turkey) and dexamethasone (Maxidex®%0.1 ophthalmic pomade, Novartis Inc., Istanbul, Turkey). No per- or post- operative complications were noted.
Discussion
In ophthalmological practice when medical and surgical treatments fail, the destructive surgeries (evisceration or enucleation) might be indicated.3 If there is no contraindication evisceration provides better prosthetic motility, cosmesis, and long-term implant stability than enucleation [5, 6]. It should be considered that any suspicion of intraocular malignancy is an absolute contraindication of evisceration [7, 8]. When managing a suspected or diagnosed intraocular malignancy, enucleation should be performed [9, 10]. Orbital evisceration is commonly performed to treat ‘painful blind eye’ due to underlying causes such as previous ocular trauma, chronic glaucoma, chronic ocular inflammation, retinal ischemia, and previous ocular infection [11]. Orbital evisceration may also be performed to treat severe open globe injuries and uncontrolled infections that do not respond to treatment [12]. Treatment of infected/ inflamed eyes with primary evisceration is relatively uncommon Chiu, et al [13] reported a total of 26 emergency evisceration cases between 2006 and 2018. Most cases were performed due to endophthalmitis/microbial keratitis with corneal perforation (61.5%). In the present study, while it was not performed as an immediate surgery, inconsistently, non-infectious corneal perforation was a more frequent indication of primary evisceration than infectious etiologies.
Blindness secondary to ocular trauma is still a global challenge especially in developing countries [14]. Severe injuries may require the removal of the affected eye [15].
Though the Ocular Trauma Score predicts visual potential and has been used in the management, there is currently no definitive guideline on when primary enucleation/ evisceration should be considered. [16, 17]. Incidence of evisceration has been reported to be 10.7% – 28% in ocular trauma along the literature. [18, 19, 20, 21] A study from Nepal, Limbu3 et al reported that, ocular trauma and its sequel (55.2%) are the major causes for evisceration. When it comes to the primary surgical intervention, trauma and associated sequel tends to be a less common reason as it was reported in the present study. Evisceration surgery is a sensitive operation which may trigger psychosocial trauma and physical disability. For this reason, it is preferred not to perform evisceration surgery as a primary intervention even if the penetrating injury is extremely severe. Moreover, for forensic reasons it is always better to postpone the evisceration surgery unless it is really indicated [17, 18, 19, 20, 21, 22]. In the present study, although the penetrating injury was not severe the rough decision for primary evisceration was made in 2 patients due to both poor prognosis of the situation and diminished self-care of the patients. Evisceration surgery is not a primary indication in the management of non-traumatic corneal perforations. In this condition, ocular integrity restoration is the main goal. Treatment can be medical or surgical depending on the etiology, size, location of the perforation, and the underlying disease status [23, 24]. In the presented study, evisceration was performed as a primary surgical intervention in 6 patients for non-traumatic non- infectious reasons. In all these eyes, perforation was resistant to both medical and surgical interventions. All patients were in elder age and debile with no light perception.
Although it should be a final decision to perform evisceration in order to control ocular infection, there can be challenging cases with extensive corneal melting or extraocular dissemination of the disease despite intensive antimicrobial treatment [25, 26, 27]. In the literature; the incidence of eye removal due to uncontrolled microbial keratitis has been reported between 7% and 15% [28]. Constantinou, et al. [25] reported that, the most common indications for evisceration were uncontrolled severe keratitis (13.4%) and corneal perforation (8.9%) [25]. Yarimada, et al. [7] reported evisceration rate among culture positive keratitis as 5.6%. In the present study, it was reported that the most common cause of primary evisceration was microbial ocular infection with or without accompanying corneal perforation. There are various complications of evisceration surgery including implant exposure, infection, proptosis, enophthalmos, superior sulcus deformity, socket contraction, ptosis and ectropion. [29] The reported rates of implant exposure following evisceration for all causes are estimated to be between 0 and 67%. [30] Conventionally, primary orbital implant use in infectious etiologies is discouraged to reduce the risk of implant exposure. For this reason, in the present group of cases, orbital implant use in infectious cases was not preferred.
Conclusion
In conclusion, while evisceration surgery is predominantly an elective procedure, it can be performed in particularly challenging cases as a primary surgical intervention. Ophthalmologists tend to postpone evisceration surgery as much as possible in order to avoid its psychosocial trauma and physical disability side effects, especially in traumatic or infectious cases. However, in especially elderly cases with corneal perforation and infection primary evisceration surgery might be a good decision. Clinicians should think wisely and consider the benefit and damage balance when deciding to perform evisceration surgery as a primary intervention. As a result of such an evaluation, instead of performing several unsuccessful surgeries that cause discomfort for both the patient and the clinician, it may provide an effective final clinical outcome.
Conflicts of Interest and Source of Funding: None of the authors have conflict of interest with the submission. This study is not funded by any source.
References
-
Rasmussen MLR, Prause JU, Johnson M, Kamper- Jørgensen F, Toft PB (2010) Review of 345 eye amputations carried out in the period 1996–2003, at Rigshospitalet, Denmark. Acta Ophthalmol 88(2): 218- 221.
-
Dada T, Ray M, Tandon R, Vajpayee RB (2002) A study of the indications and changing trends of evisceration in north India. Clin Experiment Ophthalmol 30(2): 120- 123.
-
Limbu B, Saiju R, Ruit S (2009) A retrospective study on the causes for evisceration at Tilganga Eye Centre. Kathmandu Univ Med J (KUMJ) 7(26): 115-119.
-
Ibanga A, Asana U, Nkanga D, Duke R, Etim B et al. (2013) Indications for eye removal in southern Nigeria. Int Ophthalmol 33(4): 355-360.
-
Timothy NH, Freilich DE, Linberg JV (2003) Evisceration versus enucleation from the ocularist’s perspective. Ophthal Plast Reconstr Surg 19(6): 417-420.
-
Gurdal C, Erdener U, Irkec M, Orhan M (2002) Incidence of sympathetic ophthalmia after penetrating eye injury and choice of treatment. Ocul Immunol Inflamm 10(3): 223-227.
-
Yarımada S, Ozlem BS, Palamar M, et al. (2022) Comparison of Culture Positive and Negative Microbial Keratitis. Turk J Ophthalmol 52(1): 1–5.
-
Onay MP, Yagci A, Akalin T (2011) Choroid Melanoma Causing Contralateral Amaurosis via Orbital Invasion. Turkish J Ophthalmol 41(3): 194-196.
-
Phan LT, Hwang TN, McCulley TJ (2012) Evisceration in the Modern Age. Middle East Afr J Ophthalmol 19(1): 24.
-
Nalcaci S, Palamar M, Yaman B, Akalin T, Mentes J (2016) Choroidal malignant melanoma with no extraocular extension presenting as orbital cellulitis. Orbit 35(5): 285-287.
-
Migliori ME (2002) Enucleation versus evisceration. Curr Opin Ophthalmol 13(5): 298-302.
-
Al-Dahmash SA, Bakry SS, Almadhi NH, Alashgar LM (2017) Indications for enucleation and evisceration in a tertiary eye hospital in Riyadh over a 10-year period. Ann Saudi Med 37(4): 313-316.
-
Chiu SJ, Tan JHY, Currie ZI (2021) To implant or not to implant: emergency orbital eviscerations with primary orbital implants. Eye (Lond) 35(11): 3077-3086.
-
Selver OB, Palamar M, Egrilmez S, Yagci A (2016) Traumatic wound dehiscence after penetrating keratoplasty. Ulus Travma Acil Cerrahi Derg 22(5): 437- 440.
-
Wong TY, Tielsch JM (1999) A population-based study on the incidence of severe ocular trauma in Singapore. Am J Ophthalmol 128(3): 345-351.
-
Soni NG, Bauza AM, Son JH, Langer PD, Zarbin MA et al. (2013) Open globe ocular trauma: functional outcome of eyes with no light perception at initial presentation. Retina 33(2): 380-386.
-
Gauthier AC, Oduyale OK, Fliotsos MJ, Sidra Zafar, Nicholas R Mahoney, et al. (2020) Clinical Characteristics and Outcomes in Patients Undergoing Primary or Secondary Enucleation or Evisceration After Ocular Trauma. Clin Ophthalmol 14: 3499-3506.
-
Genevois O, Millet P, Retout A, Quintyn JC (2004) Comparison after 10 years of two 100-patient cohorts operated on for eviscerations or enucleations. Eur J Ophthalmol 14(5): 363-368.
-
Ozgur OR, Akcay L, Dogan OK (2007) Primary implant placement with evisceration in patients with endophthalmitis. Am J Ophthalmol 143(5): 902-904.
-
Chaudhry IA, Alkuraya HS, Shamsi FA, Elzaridi E, Riley FC (2007) Current indications and resultant complications of evisceration Ophthalmic Epidemiol. 14(2): 93-97.
-
MacEwen CJ, Baines PS, Desai P (1999) Eye injuries in children: the current picture. Br J Ophthalmol 83(8): 933-936.
-
Rahman I, Maino A, Devadason D, Leatherbarrow B (2005) Open globe injuries: factors predictive of poor outcome. Eye (Lond) 20(12): 1336-1341.
-
Loya-Garcia D, Serna-Ojeda JC, Pedro-Aguilar L, Jimenez- Corona A, Olivo-Payne A et al. (2017) Non-traumatic corneal perforations: aetiology, treatment and outcomes. Br J Ophthalmol 101(5): 634-639.
-
Cikmazkara I, Selver OB, Palamar M, Egrilmez S, Yagci A (2020) Tectonic Keratoplasty in Patients with Non- traumatic, Non-infectious Corneal Perforations. Open Ophthalmol J 14(1): 75-77.
-
Constantinou M, Jhanji V, Tao LW, Vajpayee RB (2009) Clinical review of corneal ulcers resulting in evisceration and enucleation in elderly population. Graefes Arch Clin Exp Ophthalmol 247(10): 1389-1393.
-
Jain R, Bhutia KL, Mohan N, Gupta CKC, Ghai A (2018) Outcome of Therapeutic Keratoplasty in Hopeless Microbial Keratitis Cases Otherwise Advised Evisceration. Cornea 37(2): 151-155.
-
Selver OB, Egrilmez S, Palamar M, Arici M, Polat SH, et al. (2015) Therapeutic Corneal Transplant for Fungal Keratitis Refractory to Medical Therapy. Exp Clin Transplant 13(4): 355-359.
-
Kunimoto DY, Sharma S, Garg P, Gopinathan U, Miller D et al. (2000) Corneal ulceration in the elderly in Hyderabad, south India. Br J Ophthalmol 84(1): 54-59.
-
Al-khersan H, Pirakitikulr N, Kalavar M, Clauss K, Patel NA, et al. (2021) Primary evisceration for neonatal endogenous endophthalmitis: A report of two cases. Am J Ophthalmol case reports 22.
-
Gupta R, Hari P, Khurana B, Kiran A (2019) Risk factors for orbital implant exposure after evisceration: A case control study of 93 patients. Indian J Ophthalmol 67(7): 1148-1151.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report