Knowledge about Cataract and Associated Factors among Adults
Introduction: Cataract is the leading cause of blindness globally and accounts for half of the total blindness in Ethiopia. Despite being treatable, the need for knowledge about cataract and its treatment options is a barrier to timely service in developing countries. Improving community knowledge about cataracts can be vital in improving eye care-seeking behavior. Objective: To assess knowledge and associated factors about cataract among adults in Kombolcha, Northeast Ethiopia. Methods: Community-based cross-sectional study was implemented. A stratified multistage sampling technique was used to select 847 study participants aged 18 years or older. A face-to-face interview was applied using a pretested structured questionnaire in the Amharic language. The collected data was entered into Epidemiological Information version 7 and exported to the Statistical Package for Social Sciences version 20 for analysis. Descriptive statistics and binary logistic regression with odds ratio were used. Variables with a p-value of less than 0.05 in multivariable logistic regression were considered statistically significant predictors for knowledge about cataract. Results: A total of 771 participants completed the study with a response rate of 91%. Of the total, 86.0% were from urban kebeles, and 50.8% were female. The median age of the participants was 30 years. About 75.6% (583) of individuals were familiar with the word cataract. Overall 537 (69.6%, 95% CI: 66.3- 72.9) had good knowledge about cataract. Higher educational status (AOR: 6.041; 95% CI: 3.106-11.746), being married (AOR: 1.787; 95% CI: 1.174-2.721), history of a previous eye examination (AOR: 1.619; 95% CI: 1.053-2.488) and positive history of cataract (AOR: 10.443; 95% CI: 2.078-52.493) were factors significantly associated with good knowledge about cataract. Conclusion: Considerable proportion of study participants was knowledgeable about cataract. Higher educational status, being married, having a previous eye examination and having a positive history of cataract had a significantly positive association with good knowledge about cataract. Boosting knowledge about cataracts is required for the community segment without formal education.
Introduction
A cataract is an age-related or acquired crystalline lens opacity that results in total vision loss if left untreated. [1, 2, 3]. It is the first leading cause of blindness and the second leading cause of visual impairment worldwide. It contributed to 45% of blindness and 32% of visual impairment among older adults in sub-Saharan Africa [4]. Further, it is the leading cause of blindness (49.9%) and low vision (42.3%) in Ethiopia [5]. Vision loss from cataract is reversible with over 94% success rate using existing knowledge and technology [6]. But this treatment is underutilized in Africa mainly because of poor literacy about cataract and its treatment options [7, 8, 9, 10, 11]. This low knowledge level is attributed to delayed intervention. Treatment delay compromises the ability to perform routine activities and affects the quality of life [12, 13, 14, 15]. According to the community-based cross-sectional study conducted in Southeast Asian countries, good knowledge about cataract ranges from 38.6% in Malaysia to 80.3% in India [16, 17, 18, 19, 20]. Similarly, in Gulf countries, good knowledge about cataract range from 27.6% in Saudi Arabia to 57.3% in Iran [21, 22, 23, 24, 25]. In the African context, a community-based cross- sectional study conducted in Nigeria and Ghana reported that only 28.90% and 30.0% of the study population had good knowledge about cataract [12, 15]. Correspondingly, a population-based cross-sectional study conducted in Gondar, northwest Ethiopia revealed that 61.70% of the population had good knowledge about cataract [26].
Concerning factors, a higher level of education was positively associated with good knowledge about cataract [13, 18, 21, 22, 26]. The odds of good knowledge about cataract were four times higher among those with tertiary education than those without formal education [13]. Considering residency, urban resident adults were more knowledgeable about cataract [12, 13, 18]. However, in another study, young rural dwellers were more knowledgeable about cataract [18]. Being married [12], being female [21] and having high economic status was positively associated with good knowledge of cataract [24, 26]. Different studies conducted in different regions of the world showed that a history of a previous eye examination [26], previous diagnosis of cataract [22], history of cataract surgery [13] and family history of eye disease [17] was positively associated with good knowledge about cataract. One of the reasons for high cataract backlog in the study area could be poor knowledge about cataract in the population. Therefore, this study aimed to assess knowledge about cataract and associated factors to provide scientific evidence that can be used as a piece of evidence for stakeholders to maximize health promotion strategies. Therefore this study aimed to assess knowledge and associated factors about cataract among adults in Kombolcha city Northeast Ethiopia, 2019.
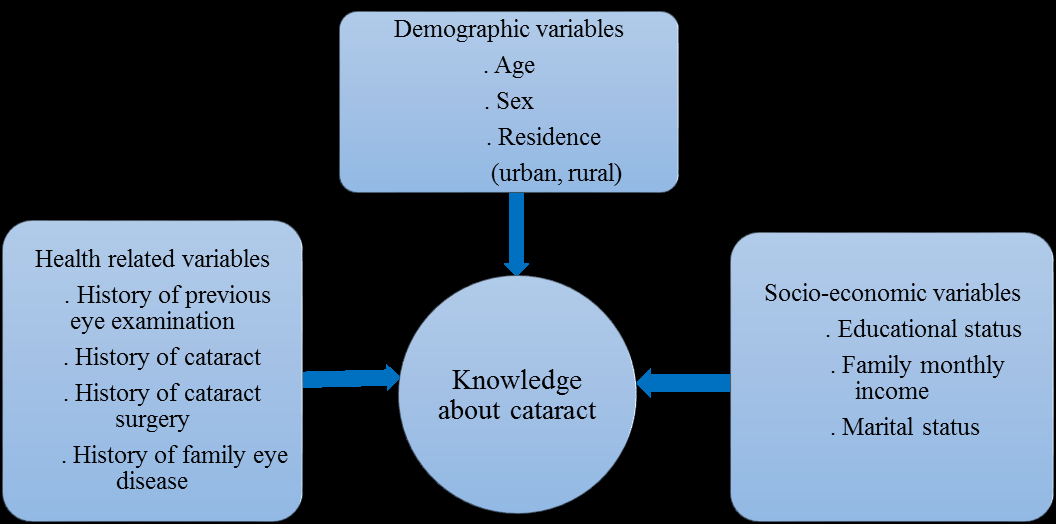
Conceptual Framework
The conceptual framework was developed by reviewing available literature and taking possible variables associated with knowledge about cataract (Figure 1).
Methods and Materials
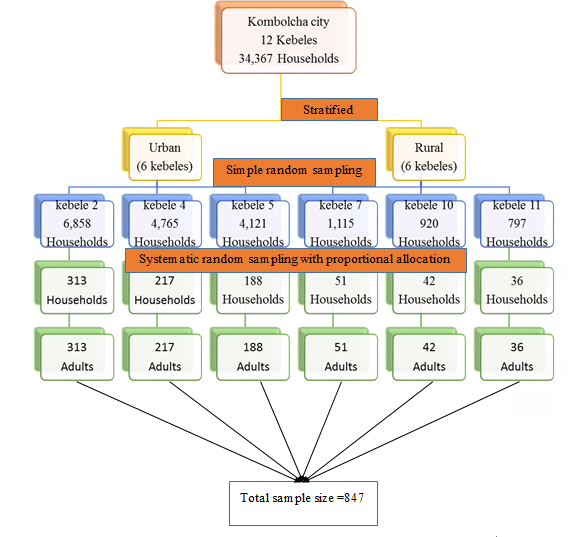
A community-based cross-sectional study was conducted at Kombolcha City, located 376 km North of Addis Ababa and 505 km East of Bahir Dar. The city has 12 kebeles/lower administrative units, with a total population 149,665 [27]. Four health centers and more than twenty private clinics provide health services to the population. Nevertheless, an established eye care center in the city has yet to be started. The study was conducted from April 26 - May 3. All people living in randomly selected kebeles of Kombolcha town were a study population, and all people aged over 18 years and who lived in the study area for at least six months were included in the study. Knowledge was categorized as good if the participant correctly answered six or more questions and categorized as poor if the participant answered less than six questions from the total 12 knowledge questions [18]. The dependent variable was knowledge about cataract (good, poor). Independent variables such as demographic, socio economic and health-related variables were included. The sample size was determined by using the single population proportion formula. Considering the proportion of adequate knowledge of 50 %, a marginal error of 5%, a design effect of 2 and 10 % of the non-response rate, the final sample size was 847. A stratified multistage sampling technique was applied. Kebeles were stratified into urban and rural strata. Then at stage one, three kebeles were selected from each stratum using simple random sampling. At stage two, participating households were selected from six selected kebeles using a systematic random sampling technique with a sampling fraction of K=21. The samples were proportionally allocated to their total number of households. One adult was selected randomly in houses that had more than one (Figure 2).
A structured questionnaire adapted from previous studies was used to collect data [22, 23, 28]. In order to ensure the quality of data, the questionnaire was translated from English to Amharic (local language) and then back to English by language expertise for consistency. A pretest was conducted (on 5 % of the sample size) in an area with a similar setting outside the study area (Harbu town), and training was given to data collectors for one day. Six optometrists collected data using an interviewer-administered Amharic version questionnaire on a home-to-home base. The collected data was checked out for completeness, accuracy, and clarity. Data clean-up and cross-checking were done before analysis. After coding, the data were entered into Epidemiological Information (EPI INFO) version 7 and exported to Statistical Package for Social Science (SPSS) version 20 for analysis. The descriptive statistic was carried out for each variable to compute frequency and proportion/percentage. The variables that were found with P < 0.2 on bivariable analysis were entered into multivariable analysis using the enter method. The Hosmer and Lemeshow goodness of fit test was used to check model fitness. A variable inflation factor checked multicollinearity between variables. The odds ratio with a 95 % confidence interval at p<0.05 was used to determine a statistically significant association.
Results
A total of 771 participants completed the study with a response rate of 91%. About 86.0% were from urban kebeles, and 50.8% were females. The median age of the participants was 30 years, with an interquartile range of 16 years (Table 1).
| Socio-demographic characteristics | Frequency | Percentage | |
|---|---|---|---|
| Residence | Urban | 663 | 86 |
| Rural | 108 | 14 | |
| Sex | Male | 379 | 49.2 |
| Female | 392 | 50.8 | |
| Age (years) | ≤40 | 574 | 74.5 |
| 41-60 | 145 | 18.8 | |
| >60 | 52 | 6.7 | |
| Educational status | no formal education | 116 | 15 |
| Primary school | 170 | 22 | |
| Secondary school | 281 | 36.5 | |
| College or above | 204 | 26.5 | |
| Marital status | Single | 251 | 32.5 |
| Married | 433 | 56.2 | |
| Divorced | 50 | 6.5 | |
| Widowed | 37 | 4.8 | |
| Occupation | Merchant | 145 | 18.8 |
| Government employee | 140 | 18.2 | |
| Private workers | 145 | 18.8 | |
| Housewife | 154 | 20 | |
| Unemployed | 69 | 8.9 | |
| Others | 118 | 15.3 | |
| Family monthly income (ETB) | ≤1000 | 57 | 7.4 |
| 1001-3000 | 330 | 42.8 | |
| 3001-5000 | 230 | 29.8 | |
| >5000 | 154 | 20 | |
| Clinical Characteristics | Frequency | Proportion (%) | |
| Previous Eye Examination | |||
| Yes | 215 | 27.9 | |
| No | 556 | 72.1 | |
| History of Cataract | |||
| Yes | 33 | 4.3 | |
| No | 738 | 95.7 | |
| History of Cataract Surgery | |||
| Yes | 25 | 3.2 | |
| No | 746 | 96.8 | |
| History of Family Eye Disease | |||
| Yes | 217 | 28.1 | |
| No | 554 | 71.9 | |
| Chronic Disease ( DM & or/HTN) | |||
| Yes | 66 | 8.6 | |
| No | 705 | 91.4 |
Table 1: Socio-demographic characteristics of the studied participants in Kombolcha City, Northeast Ethiopia, (n=771).
About 215 (27.9%) participants had a history of previous eye examinations at least once in their life, and 33 (4.3%) had a positive history of cataract (Table 2).
In this study, 537 (69.6%, 95% CI: 66.3-72.9) study participants had good knowledge about cataract and 583 (75.6%) study participants were familiar with the term cataract. Broadcast media (television or radio), people having cataract and eye care professionals were the primary sources of information for 256 (43.9%), 197 (33.8%) and 76 (13.0%) of the study participants, respectively. During bivariable analysis using binary logistic regression, sex, educational status, marriage, and occupation, family monthly income level, history of a previous eye examination, history of cataract and history of family eye disease were significantly associated with knowledge about cataract. In multivariable analysis, only educational status, marital status, previous eye examination history and cataract history showed significant association (Table 3). The odds of good knowledge about cataract were 1.95 times higher among study participants with primary education than those without formal education (AOR: 1.954; 95% CI: 1.139-3.355). Compared with these participants without formal education, the likelihood of having good knowledge about cataract among participants who completed secondary school education and those with college and above were 2.5 (AOR: 2.545; 95%CI: 1.499, 4.321) and 6.0 (AOR: 6.041; 95%CI: 3.106-11.746) times higher respectively. The odd of good knowledge about cataract was 1.78 more among married study participants than single participants 1.78 (AOR: 1.787; 95% CI: 1.174-2.721). Adults who had eye examinations at least once in their life were 1.6 times more knowledgeable about cataract than those with no history of a previous eye examination 1.6 (AOR: 1.619; 95% CI: 1.053-2.488). Also, adults with a history of cataracts were more than ten times more likely to have good knowledge about cataract than those who did not develop the disease (AOR: 10.443; 95% CI: 2.078-52.493) (Table 3).
| Variables | Knowledge about cataract | COR (95% CI) | AOR (95% CI) | |
|---|---|---|---|---|
| Good | Poor | |||
| Residence | ||||
| Rural | 67 | 41 | 1 | 1 |
| Urban | 470 | 193 | 1.490 (0.976-2.275) | 1.084 (0.670-1.753) |
| Sex | ||||
| Female | 258 | 134 | 1 | 1 |
| Male | 279 | 100 | 1.449 (1.063-1.975) | 1.365 (0.923-2.017) |
| Educational Status | ||||
| No formal education | 65 | 51 | 1 | 1 |
| Primary school | 109 | 61 | 1.402 (0.866-2.271) | 1.954 (1.139-3.355)* |
| Secondary school | 192 | 89 | 1.693 (1.085-2.640) | 2.545 (1.499-4.321)** |
| College or above | 171 | 33 | 4.066 (2.410-6.858) | 6.041 (3.106-11.746)** |
| Marital Status | ||||
| Single | 164 | 87 | 1 | 1 |
| Married | 316 | 117 | 1.433 (1.024-2.004) | 1.787 (1.174-2.721)** |
| Divorced | 33 | 17 | 1.030 (0.543-1.953) | 1.726 (0.825-3.612) |
| Widowed | 24 | 13 | 0.979 (0.475-2.019) | 1.184 (0.467-3003) |
| Occupation | ||||
| Unemployed | 41 | 28 | 1 | 1 |
| Merchant | 97 | 48 | 1.380 (0.763-2.495) | 1.238 (0.652-2.349) |
| Government employee | 118 | 22 | 3.663 (1.890-7.100) | 1.574 (0.745-3.328) |
| Private worker | 105 | 40 | 1.793 (0.981-3.276) | 1.607 (0.843-3.065) |
| Housewife | 101 | 53 | 1.301 (0.726-2.334) | 1.542 (0.769-3.089) |
| Other | 75 | 43 | 1.191 (0.648-2.191) | 1.113 (0.573-2.163) |
| Household Income | ||||
| ≤1000 | 31 | 26 | 1 | 1 |
| 1001-3000 | 221 | 109 | 1.701 (0.962-3.005) | 1.710 (0.929-3.149) |
| 3001-5000 | 160 | 70 | 1.917 (1.060-3.466) | 1.378 (0.721-2.633) |
| >5000 | 125 | 29 | 3.615 (1.870-6.991) | 1.981 (0.957-4.101) |
| Eye Examination | ||||
| No | 365 | 191 | 1 | 1 |
| Yes | 172 | 43 | 2.093 (1.435-3.052) | 1.619 (1.053-2.488)* |
| History of Cataract | ||||
| No | 506 | 232 | 1 | 1 |
| Yes | 31 | 2 | 7.107 (1.687-29.945) | 10.443 (2.078-52.493)** |
| Chronic Disease | ||||
| No | 486 | 219 | 1 | 1 |
| Yes | 51 | 15 | 1.532 (0.843-2.784) | 0.966 (0.472-1.977) |
| Family Eye Disease | ||||
| No | 374 | 180 | 1 | 1 |
| Yes | 163 | 54 | 1.453(1.018, 2.073) | 1.619(1.053, 2.488) |
Table 2: Factors associated with knowledge about cataract by bivariable and multivariable logistic regression analysis among adul
Discussion
Timely intervention is a crucial factor in reducing the burden of visual impairment and blindness caused by cataract. Hence, good knowledge about cataract likely improves timely eye care service-seeking behavior. In this study, about 69.6% of the participants had adequate knowledge about cataract. This finding is higher than the study done in Gondar (61.7%) [26]. This might be due to the difference in the composition of study participants. In this study, 25.5% of participants were older than 40 years, as compared to 15.7% in the latter study. Hence, the age-related nature of the disease might contribute to a better knowledge of aged participants, which is supported by different studies [22, 28, 29]. Further, this finding is higher than the study conducted in rural Nigeria, 18.2% [12]. This difference may be mainly attributed to variations in the participant’s residential area. In this study, 86% of the study participants were urban residents, unlike in the case of a later study in which more rural residents participated. People living in urban areas are more likely to have better exposure to media and access to consult eye care professionals, which can increase access to health education and knowledge [28]. Similarly, knowledge towards cataract in this study was higher than in the study conducted in Ghana, 4.40% [13] and the hilly region of Nepal, 39.1%. [20]. This might be due to the variation in the cut point categorized good knowledge and educational status of the participants. In this study, the cut point was 50%; in Ghana, greater than 75% of the total questions were used to categorize. Additionally, 15% of the study participants had yet to formal education in this study compared to 28.8% in the Nepal study. Educational background affects knowledge towards cataract supported by different studies [18, 21, 26].
In contrast, this finding is lower than the study conducted in Indian 80.3% [18]. This difference might be due to the difference in knowledge measurement. In the current study, the proportion was computed among all participants, but in the latter study, the term cataract was only computed among those familiar with it. Nevertheless, this finding aligns with previous studies conducted in Saudi Arabia, Tabuk City 66.30% [23] and Hail region 70.90% [24]. The similarity in the study design and age distribution of study participants might explain it. Educational status, marital status, previous eye examination history and cataract history had significant association with knowledge about cataract in multivariable logistic regression. Adults with higher educational status were more likely to have good knowledge about cataract compared with those who did not have formal education. Preceding studies support it [13, 18, 21, 26]. People with a high level of education are more likely to attend health education programs, understand written and audio-visual documents and approach the information sources improve knowledge [29]. Marriage was also positively associated with good knowledge in this study. The previous stud reported this positive association [12]. This might be because married individuals are more likely to get the courage and support to visit eye care centers [30]. Thus, it increases the possibility of meeting eye care professionals who can contribute to better awareness and knowledge.
The other associated factor was a history of a previous eye examination. Participants who had a history of eye examination at least once were more likely to have good knowledge about cataract. A similar finding was also reported in a previous study [28]. This may be because an eye examination increases the possibility of attending health education that can improve knowledge. Those who heard about a cataract from a health professional or diseased individuals had a better understanding [16]. Having a history of cataracts was also positively associated with good knowledge. This association was also mentioned in another study [22]. People having problems with cataract were more likely to contact eye care professionals, and they might have got an explanation about the condition that improves knowledge about it.
Limitations of the study
The proportion of good knowledge might be overestimated because of the considerable number of urban resident study participants.
Conclusion
In this study, the predominant participants had good knowledge of cataract. Higher educational status, being married, having a history of previous eye examinations and having a positive history of cataract had a significantly positive association with good knowledge about cataract. Maximizing health promotion programs about cataract is recommended, targeting people without formal education.
Acknowledgments
The authors acknowledge the University of Gondar, the Kombolcha town administration office, and all study participants for their cooperation and willingness.
Ethical Considerations
Ethical clearance was obtained from the School of Medicine, University of Gondar College of Medicine and Health Science, ethical review committee. Support letters were obtained from respective administrative areas (kebeles). The purpose of the study was explained to each participant, and verbal and written consent was obtained from each participant before starting the interview.
Funding
The University of Gondar supported the data collection process
Data Availability
The dataset on which the conclusion was made is available in software and only available on request from Mr Haile Woretaw (contact address: haileworetaw@gmail. com). SM developed the proposal document, entered data and analyzed it. FA reviewed the proposal and developed a data collection tool. HW interpreted the data, reviewed the research concept and prepared the manuscript. All the authors reviewed and approved the final manuscript.
Computing Interest
The authors declare that they have no competing interests.
Consent for Publication
Not applicable
References
-
Brian G, Taylor H (2001) Cataract blindness: Challenges for the 21st century. Bulletin of the World Health Organization 79(3): 249-256.
-
Praveen M, Shah G, Vasavada A, Mehta P, Gilbert C (2010) A study to explore the risk factors for the early onset of cataract in India. Eye 24(4): 686-694.
-
Virgolici B, Popescu L (2006) Risk factors in cataract. Oftalmologia 50(2): 3-9.
-
Flaxman SR, Bourne RRA, Resnikoff S, Ackland P, Braithwaite T, et al. (2017) Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. The Lancet Global Health 5(12): e1221-e1234.
-
Berhane Y, Worku A, Bejiga A, Adamu L, Alemayehu W, et al. (2007) Prevalence and causes of blindness and low vision in Ethiopia. Ethiopian Journal of Health Development 21(3): 204-210.
-
Lundstrom M, Barry P, Henry Y, Rosen P, Stenevi U (2013) Visual outcome of cataract surgery; study from the European Registry of Quality Outcomes for Cataract and Refractive Surgery. Journal of Cataract & Refractive Surgery 39(5): 673-679.
-
Batlle JF, Lansingh VC, Silva JC, Eckert KA, Resnikoff S (2014) The cataract situation in Latin America: barriers to cataract surgery. Am J Ophthalmol 158(2): 242-250.
-
Li Z, Song Z, Wu S, Xu K, Jin D, et al. (2014) Outcomes and barriers to uptake of cataract surgery in rural northern China: the Heilongjiang Eye Study. Ophthalmic epidemiology 21(3): 161-168.
-
Odugbo OP, Mpyet CD, Chiroma MR, Aboje AO (2012) Cataract blindness, surgical coverage, outcome, and barriers to uptake of cataract services in Plateau State, Nigeria. Middle East African Journal of Ophthalmology 19(3): 282-282.
-
Mehari ZA, Zewedu RTH, Gulilat FB (2013) Barriers to cataract surgical uptake in central ethiopia. Middle East African journal of ophthalmology 20(3): 229-233.
-
Briesen S, Geneau R, Roberts H, Opiyo J, Courtright P (2010) Understanding why patients with cataract refuse free surgery: the influence of rumours in Kenya. Tropical Medicine & International Health 15(5): 534-539.
-
Onwubiko SN, Eze BI, Udeh NN, Okoloagu NN, Okosa CMC (2015) Knowledge and attitudes towards eye diseases in a rural south-eastern Nigerian population. Journal of health care for the poor and underserved 26(1): 199- 210.
-
Akowuah P, Kabir MA, Sadik AA, Forfoe S (2018) Knowledge about cataract and its risk factors among an adult population in the Cape Coast Metropolis, Ghana. Optom open access 3(1): 127.
-
Lamoureux EL, Fenwick E, Pesudovs K, Tan D (2011) The impact of cataract surgery on quality of life. Current opinion in ophthalmology 22(1): 19-27.
-
Hong T, Mitchell P, Burlutsky G, Gopinath B, Liew G, et al. (2015) Visual impairment and depressive symptoms in an older Australian cohort: longitudinal findings from the Blue Mountains Eye Study. British Journal of Ophthalmology 99(8): 1017-1021.
-
Zhang B, Gao J, Pan C, Luan M, Chen X (2016) Awareness and knowledge about cataract, glaucoma, and age-related macular degeneration in Chengdu, China. International Eye Science 16(3): 397-402.
-
Chew Y, Reddy S, Karina R (2004) Awareness and knowledge of common eye diseases among the academic staff (non-medical faculties) of University of Malaya. Med J Malaysia 59(3): 305-311.
-
Lakshmipriya K (2017) Awareness and knowledge about glaucoma and cataract in rural population and urban population. Adv Ophthalmol Vis Syst 7(5): 00237.
-
Thapa SS, Berg RV, Khanal S, Paudyal I, Pandey P, et al. (2011) Prevalence of visual impairment, cataract surgery and awareness of cataract and glaucoma in Bhaktapur district of Nepal: The Bhaktapur Glaucoma Study. BMC ophthalmology 11(1): 1-9.
-
Shrestha GS, Sigdel R, Shrestha JB, Sharma AK, Shrestha R, et al. (2018) Awareness of eye health and diseases among the population of the hilly region of Nepal. Journal of ophthalmic & vision research 13(4): 461-469.
-
Katibeh M, Ziaei H, Panah E, Moein HR, Hosseini S, et al. (2014) Knowledge and awareness of age related eye diseases: a population-based survey. Journal of ophthalmic & vision research 9(2): 223-231.
-
Magliyah MS, Nageeb MR, Abdulmannan DM, Badr HM, Hemmeish MM, et al. (2015) Assessment of knowledge regarding cataract among Saudi adult population in Makkah city, Saudi Arabia. International Journal of Medical Science and Public Health 4(5): 595-599.
-
Lahim WAA, Ghofaili RSA, Mirghani H, ALBalawi H (2018) Evaluation of awareness and attitudes towards common eye diseases among the general population of Northwestern Saudi Arabia. The Egyptian Journal of Hospital Medicine 70(11): 1983-1989.
-
Bandar A (2016) Assessment of awareness, knowledge, attitudes and practices associated with eye diseases in the population of Aljouf and Hail Province of Saudi Arabia. Int J Med Res Prof 2(2): 33-39.
-
Haddad MF, Bakkar MM, Abdo N (2017) Public awareness of common eye diseases in Jordan. BMC ophthalmology 17(1): 177.
-
Alimaw YA, Hussen MS, Tefera TK, Yibekal BT (2019) Knowledge about cataract and associated factors among adults in Gondar town, northwest Ethiopia. Plos one 14(4): e0215809.
-
Ethiopia (2019) Population projections for Ethiopia - central statistical agency.
-
Shrestha MK, Guo CW, Maharjan N, Gurung R, Ruit S (2014) Health literacy of common ocular diseases in Nepal. BMC ophthalmology 14(1): 1-8.
-
Dagtekin G, Dermirtas Z, Soysal A, Yildirm N, Onsuz F, et al. (2018) The assessment of the knowledge and awareness about glaucoma in glaucoma patients and general population: A sample from Turkey. Int J Res Med Sci 6(1): 35-41.
-
Blumberg SJ, Vahratian A, Blumberg JH (2014) Marriage, cohabitation, and men’s use of preventive health care services: NCHS Data Brief (154): 1-8.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report