Clinical and Epidemiological Aspects of Traumatic Cataracts in Children at CHU Campus of Lome
Introduction: Traumatic cataracts are the leading cause of unilateral cataracts, with a risk of amblyopia in young children. The objective of this study was to describe the epidemiological and clinical aspects of traumatic cataracts in children at CHU Campus of Lome. Methods: This was a retrospective descriptive study conducted using records of children with cataract due to blunt or penetrating trauma who were admitted to the ophthalmology department at CHU Campus from January 2015 to December 2020 (6 years). Results: Eighty over the 7,800 children examined had traumatic cataracts. The mean age was 7.70 ± 3.64 years [1.1 years; 15 years]. Patients aged 5 to 10 years were the most represented with 47.50% of cases. The predominance was male, with a sex ratio of 1.5. Play was the main cause of ocular trauma in 32.50% of cases. The most common vulnerating agent was wood in 29.48% of cases, followed by a punch in 26.93%. Trauma was blunt in 57.50% of cases and penetrating in 42.50%. Anatomically, total cataract was the most common type in 70.59% of children, with a low vision on admission ≤ 1/10 in 51.25% of cases. Conclusion: Traumatic cataracts in children are uncommon but serious. Play was the primary circumstance of onset, as well as wood for the vulnerating agent. Cataracts were mostly unilateral and total, with a risk of amblyopia in young children.
Introduction
Traumatic cataract is any opacity of the crystalline lens following a lens aggression by an external vulnerating agent. Traumatic cataracts, mainly in the youth, are the leading cause of unilateral cataracts and involve a major risk of amblyopia when affecting young children [1]. It is a frequent disease that poses not only medico-legal problems (fights, accidents at work), but also social ones, as it most often affects young people [2].
In Africa, studies have focused on pediatric ocular trauma and traumatic cataracts in children [3]. From these studies, it appears that the high frequency of ocular trauma seems to be linked to a culture of violence, and traumatic cataracts, often unilateral, can jeopardize functional visual prognosis through the injuries they cause [4]. In Togo, a study of traumatic cataracts in a predominantly rural area showed that schoolchildren were the most affected with 34.40% [5]. The objective is to study the epidemiological and clinical aspects of traumatic cataracts in children at the University Hospital Center (CHU)-Lome Campus.
Study Method
This is a 6-year retrospective cross-sectional study conducted in the ophthalmology department of CHU Campus of Lome from January 2015 to December 2020. CHU Campus of Lome is the only center in Togo with a pediatric ophthalmology department.
The study included the records of all children whose age is between 0 and 15 years who consulted at the ophthalmology department of CHU Campus and were diagnosed with a traumatic cataract following blunt or penetrating trauma. Children with chemical, thermal or with intraocular foreign body (IOFB) traumatic cataracts were excluded.
The confidentiality and privacy of data collected were respected with reference to the ethical principles set out in the declaration of Helsinki.
- Data studied were:
- -Socio-demographic: age, sex, level of education
- -Clinical: general and ophthalmological personal history, circumstances of the trauma, time before consultation, laterality, visual acuity, fundus and other associated injuries.
- -B scan ultrasonography: retinal and vitreous condition. Data entry and analysis were performed using Epi info software version 7. Variables were compared using the Chi 2 test, with a significance threshold of p< 0.05. Qualitative and quantitative variables were respectively expressed as frequency and mean ± standard deviation.
Results
During our study period, 80 cases of traumatic cataracts in children were identified over 7,800 consultations that is a hospital frequency of 1.03% out of all consultations.
Socio-demographic aspects
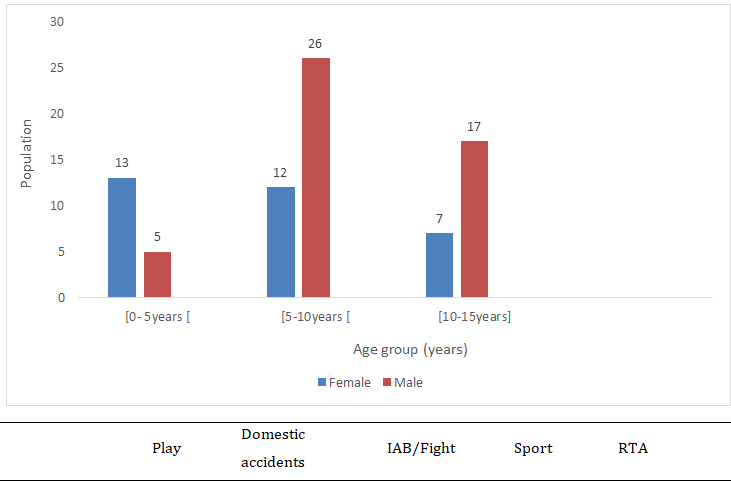
The mean age of patients was 7.70 ± 3.64 years [1.1years-15 years]. The age group between 5 and 10 years was the most represented, with 47.50% of patients. We counted 48 male and 32 female patients, that is a sex ratio of 1.5 (figure 1).
Fifty percent of children attended primary school, 27.50% secondary school and 22.50% had no education.
IAB = intentional assault and battery. RTA = road traffic accident.
| Play | Domestic Accidents | IAB/Fight | Sport | RTA | |
|---|---|---|---|---|---|
| [0- 5 years ] | 3 | 10 | 1 | 0 | 0 |
| [5-10 years ] | 17 | 11 | 10 | 2 | 2 |
| [10-15 years ] | 6 | 2 | 6 | 7 | 1 |
| 15 years | 0 | 0 | 2 | 0 | 0 |
| Total | 26 | 23 | 19 | 9 | 3 |
Table 1: Distribution of patients by circumstances of onset of the trauma and age group.
The trauma was blunt in 57.50% and penetrating in 42.50%. The most common vulnerating agent was wood in 29.48% of cases, followed by a punch in 26.93%, a knife in 11.54% and a catapult in 11.54%. Children who consulted within the first 72 hours represented 35%, followed by those who consulted between 72 hours and 1 week, 25% (Table 2).
| Population | Frequency (%) | |
|---|---|---|
| Within the 72H | 28 | 35 |
| 72H-1week | 20 | 25 |
| [1week-1 month ] | 4 | 5 |
| [1 month- 3months ] | 13 | 16.25 |
| ≥3months | 15 | 18.75 |
| Total | 80 | 100 |
Table 3: Distribution of patients by time before consultation.
Traumatic cataracts in children were all unilateral, with 45% in right eyes and 55% in left eyes.
Visual acuity was reduced to positive light perception (PL+) in 28.75% of cases, and ≥ 3/10 in 5% of cases. The majority of patients had low vision on admission ≤ 1/10th, i.e. 51.25% of cases (Table 3).
VA= Uncorrected visual acuity, RE= right eye, LE = left eye LP- = no light perception, LP+= light perception.
| RE | LE | Total | ||||
|---|---|---|---|---|---|---|
| N | % | n | % | n | % | |
| LP- | 0 | 0 | 6 | 13.6 | 6 | 7.5 |
| LP+ | 13 | 36.1 | 10 | 22.7 | 23 | 28.75 |
| LP+ <VA<1/10 | 3 | 8.33 | 9 | 20.5 | 12 | 15 |
| 1/10 ≤VA< 3/10 | 8 | 22.2 | 8 | 18.2 | 16 | 20 |
| ≥ 3/10 | 4 | 11.1 | 0 | 0 | 4 | 5 |
| Not measurable | 8 | 22.2 | 11 | 25 | 19 | 23.75 |
| Total | 36 | 100 | 44 | 100 | 80 | 100 |
Table 4: Distribution of patients by visual acuity on admission.
Anatomically, according to the type of the traumatic cataract in children, total cataract was the most represented, with 70.59% of cases, followed by anterior subcapsular, cortical and posterior subcapsular cataracts in 14.71%, 8.82% and 5.88% respectively. Traumatic cataracts were without capsular rupture in 85% of cases. Traumatic cataracts were non-dislocated in 93.75%, subluxated in 3.75% and dislocated in the vitreous body in 2.50%.
Corneal wound was the most common associated injury in 17.50% of cases, followed by corneal edema in 15% (Table 4).
| Population | Frequency (%) | |
|---|---|---|
| Corneal wound | 14 | 17.5 |
| Corneal edema | 12 | 15 |
| Corneal cover | 9 | 11.25 |
| Nephelion | 5 | 5 |
| Adherent leukoma | 4 | 5 |
| Corneoscleral wound | 2 | 2.5 |
Table 2: Distribution of patients by corneal anomalies associated with traumatic cataract.
Injuries to the iris were associated with cataracts in 51.25% of cases, and dominated by synechiae in 17.50% of cases.
As the fundus is inaccessible, injuries of the posterior segment are objectified by a B-scan ocular ultrasound. The B-scan ultrasonography showed posterior vitreous detachment, vitreous hemorrhage and retinal detachment associated with traumatic cataract in 17.39%, 13.04% and 10.87% of cases respectively.
Discussion
Socio-demographic
The study of the age distribution showed a predominance of children aged between 5 and 10 years in 47.50% of cases. The mean age of patients was 7.70 years, as reported in the studies by Kharbouch, et al. [6] and Jinagal, et al. [7], respectively 7.76 and 7.67 years. That age group between 5 and 10 years is the one in which children have more freedom of movement, are curious and have less awareness of danger. Boys were the most affected in our study, with 60% of cases [8]. Male predominance has also been noted by several authors [9, 10]. This male predominance could be explained by the turbulent behavior of boys, who are more often involved in risky activities than girls.
Clinical
The circumstances of ocular trauma responsible for traumatic cataracts were recreational accidents in 32.50% of cases. This result is similar to that of studies with proportions of 35% and 38.82% [11, 12]. The literature review reports higher rates such as 75.7% and 65% [6, 13]. All these authors agree that play in the absence of adult supervision is the main cause of ocular trauma in children, and that play is the child’s main intuitive activity. In this series, 57.50% of patients had predominantly blunt trauma, as noticed in studies from the West African
sub-region, with rates between 92.8% to 94.7% [2, 5]. On the other hand, in studies from Tunisia, perforating mechanism dominated, with rates of 56.2% and 55% [4, 14]. Are children in sub-Saharan Africa less violent than those in North Africa? The most commonly reported vulnerating agent was wood in 29.48%. Plant body is easily accessible in our countries and is present in our daily activities, what explains that it is the most frequently reported vulnerating agent.
Thirty-five percent of our patients consulted within the first 72 hours after the trauma. The time before consultation in the series was dominated by that between 1 month and 1 year, with 36% of cases after the trauma [11]. This relatively short time before consultation in our study may be linked to the accessibility of ophthalmology infrastructures in an urban area, and to the study setting. Indeed, CHU campus is the reference center for pediatric eye diseases.
Anatomically, according to the type of traumatic cataract, total cataracts were most represented in 70.59%. This result is close to the 75% found by Baklouti, et al. [14].
Visual acuity was less than 1/10 in 51.25% of cases. Initial low vision between 82 and 95% has been reported by several authors [6, 13]. Unilateral low vision in children with traumatic cataracts could be explained by the fact that most of them were total, sometimes with associated eye injuries. These children are at risk of amblyopia, which seriously jeopardizes their functional visual prognosis.
The associated injuries were of all kinds, and corneal wound is the most frequently found in 17.50% of cases. Kharbouch et al. [6] and Baklouti et al. [14] found respectively 80.3% and 55% for corneal wound. The literature notes that the cornea remains the most injured structure of the eyeball in cases of ocular trauma [15, 16, 17]. This is understandable, since the cornea is the outermost structure of the eyeball, in direct contact with the external environment. It is therefore immediately exposed to any form of aggression from the external environment. Posterior segment injuries associated with traumatic cataracts in children, as detected by the B-scan ocular ultrasound, were dominated by vitreous hemorrhage and retinal detachment in 13.04% and 10.87% of cases respectively. Studies have found the same posterior segment injuries, but in varying proportions [4, 6].
Conclusion
Traumatic cataracts in children are relatively rare but amblyogenic, and preferentially affect the age group between 5 and 10 years. The main circumstance of onset of traumatic cataracts was recreational accidents, and the mechanism found in the majority of cases was blunt. Children generally had unilateral total cataracts, with initial visual acuity often less than or equal to 1/10. Associated eye injuries of the anterior segment as well as of the posterior jeopardize the anatomical and functional prognosis, and are evidence of the violence of the trauma. Educating children about the dangers of violent play would reduce the frequency of this pathology in our environment.
References
-
Dembele A, Sidibe M, Napo A, Bakayoko S, Sylla F, et al. (2015) Functional results of childhood post-traumatic cataract at chu iota Bamako (Mali). Revue SOAO 1: 7-11.
-
Doutetien C, Tchabi S, Sounouvou I, Yehouessi L, Deguenon J, et al. (2008) Traumatic cataract at the Cotonou, hospital (Benin): epidemiological, clinicaland therapeutic considerations. J Fr Ophtalmol 31: 522-526.
-
Makita C, Ngabou NCGF, Madzou M (2016) Ocular trauma in children: epidemiological, clinical and therapeutic aspects. Revue SOAO 2: 46-50.
-
Midi KH, Gharbi J, Attia S, Tritar Z, Mgarrech M, et al. (2009) Pediatric traumatic cataract. J Fr Ophtalmol 32: 1S118.
-
Nonon-Saa KB, Maneh N, Vonor K, Banla M, Sounouvou I, et al. (2016) Management and functional results of traumatic cataract in the central region of Togo. Pan Afr Med J 24: 25: 107.
-
Kharbouch H, Benchrifa F, Mellal Z, Loudghiri MA, Berraho A (2009) Children traumatic cataract. J Fr Ophtalmol 32: 118-119.
-
Jinagal J, Gupta G, Gupta PC, Yangzes S, Singh R, et al. (2019) Visual outcomes of pediatric traumatic cataracts. Eur J Ophthalmol 29: 23-27.
-
Langlois B, Dureau P, Metge F, Audren F, Edelson C, et al. (2009) Traumatic cataract in children. J Fr Ophtalmol 32: 1S40.
-
Daoudi K, Bhallil S, Elmesbahi I, Chraibi F, Benatiya AI, et al. (2008) Pediatric traumatic cataract: what prognosis? J Fr Ophtalmol 3: 67-68.
-
Belkacem MTA, Hali A, Merad Z, Tiar M (2009) Pediatric traumatic cataract: management and prognosis. J Fr Ophtalmol 32: 1S207.
-
Diomandé IB, Ouattara Y, Diomandé GF, Diabaté Z (2012) Post-traumatic cataracts: clinical and functional prognostic aspects at Bouaké University Hospital. Revue SOAO 1: 7-14.
-
Ben Zina Z, Trigui A, Feki J, Ellouze S, Dhouib I, et al. (1998) Traumatic cataracts: epidemiology, treatment and prognosis (about 60 cases). Tunisie Médicale 76: 254-257.
-
El Kettani A, Lahlou G, Mazzouz H, Lazrak Z, Allali B, et al. (2009) Traumatic cataracts of the children. J Fr Ophtalmol 32: 1S26.
-
Baklouti K, Mhiri N, Mghaieth F, El Matri L (2005) Traumatic cataracts: clinical and therapeutic aspects. Bull Soc Belge Ophtalmol 2005(298): 13-17.
-
Çetin EN, Sarac G, Kasikçi A, Avunduk AM, Yaylali V, et al. (2012) Epidemiologic and clinical features of open- globe injuries in childhood. Turk J Ophthalmol 42: 16-19.
-
Tok O, Tok L, Ozkaya D, Eraslan E, Ornek F, et al. (2011) Epidemiological characteristics and visual outcome after open globe injuries in children. J AAPOS 15(6): 556-561.
-
Hosseini H, Masoumpour M, Keshavarz-Fazl F, Razeghinejad MR, Salouti R, et al. (2011) Clinical and epidemiologic characteristics of severe childhood ocular injuries in Southern Iran. Middle East Afr J Ophthalmol 18: 136-140.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report