Nodular Fasciitis of Upper Lid Mimicking as Sebaceous Gland Carcinoma – Case Report with Review of Literature
Nodular fasciitis is a benign form of reactive lesion of subcutaneous tissue or superficial fascia, mimicking as malignant lesion due to its rapid growth pattern and morphological features. Our patient was a 46 years aged female, presented with upper lid lesion with suspicion of sebaceous gland carcinoma. She was managed with excision of lesion with lid reconstruction by lid sharing method. Histopathology plays an important role to diagnose such cases. The proper knowledge and diagnosis of these cases can avoid unnecessary aggressive management.
Roy SR¹*, Anjum R² and Biswas SK³
¹Department of Oculoplasty and Ocular Oncology, Consultant and Head, Chittagong Eye Infirmary, Bangladesh ²Department of Histopathology and Cytopathology, Associate Consultant, Apollo Imperial Hospitals, Bangladesh ³Department of Cornea, Consultant and Head, Chittagong Eye Infirmary, Bangladesh Keywords: Nodular Fasciitis; Sebaceous Gland Carcinoma; Histopathology; Lid Reconstruction
Introduction
Nodular fasciitis is a rare and benign inflammatory reaction of subcutaneous or superficial fascia. It arises as a very fast-growing, usually single, painless, soft to firm solid lump in different places of body where fibrous tissue or fascia is available such as subcutaneous, intramuscular and fascial plan [1].
In 1955, this condition was first described by Konwaler BE, et al. [2] and termed as subcutaneous pseudo-sarcomatous fibromatosis [3]. The ancient and original term was applied due to its morphological feature as it was mimicking as malignant sarcoma. It is now termed as pseudo-sarcomatous fasciitis, infiltrative fasciitis, and proliferative fasciitis along with nodular fasciitis [4].
These lesions may be superficial or deep. The common anatomical site of this lesion are upper extremities especially volar aspect of forearm and trunk [5, 6]. It is uncommon to arise from head and neck region and reported prevalence is 7%- 15% [4]. Ocular, periorbital and orbital nodular fasciitis is rare and about 34 cases are reported in English literature till date with a age range of 9 months to 81 years [7]. This lesion is also reported in lower extremity, breast, vulva, inguinal region, supraclavicular area, skin, intra-articular, intravascular, intra-parotid, cranial and placenta [8, 9, 10].
In this article we are reporting a case of nodular fasciitis of upper eye lid mimicking as sebaceous gland carcinoma.
Case Report
A 46 years old female presented with a rapidly growing painless lesion in left upper lid for 2 weeks. She also gave history that the lesion was smaller in size and it rapidly grew after surgery in same site 3 weeks back, diagnosing the lesion as chalazion elsewhere. She had diabetes without any other systemic disease. Ocular examination revealed, 6/6 vision in both eyes. A firm, mildly tender, whitish to pink colored nodular lesion about 3.1 x 2 x 1.5 cm sized with superficial ulceration was found occupying lateral part of left upper eyelid and extending to temporal area. The lesion was not fixed with underlying tarsus. The conjunctival surface of the eyelid was not ulcerated. Anterior segment, posterior segment of left eye and right eye was normal. There was no palpable lymph node. Her complete blood count showed normal parameters except a moderately high ESR of 35 mm in 1st hour. Differential diagnosis were made as inflammatory lid lesion, sebaceous gland carcinoma or other lid malignancy due to its rapid growth pattern. Patient was treated with systemic steroid with oral antibiotic and in seven days follow up the lesion improved less. We decided for excision of lesion and upper lid reconstruction. The lesion was excised with 3 mm healthy margin and reconstruction done by modified Cutler-Beard procedure. Histopathology revealed spindle stellate cells in a loose fascicular to storiform pattern with variable cellularity in a myxoid to collagenous extracellular matrix. There was scattered lymphocytes and histiocytes with conspicuous mitotic activity. No atypical mitosis or necrosis was found. These features were consistent with nodular fasciitis. Her ankyloblepharon was released after 1.5 months of reconstruction surgery. There was no recurrence in next 6 months follow up (Figures 1 & 2).
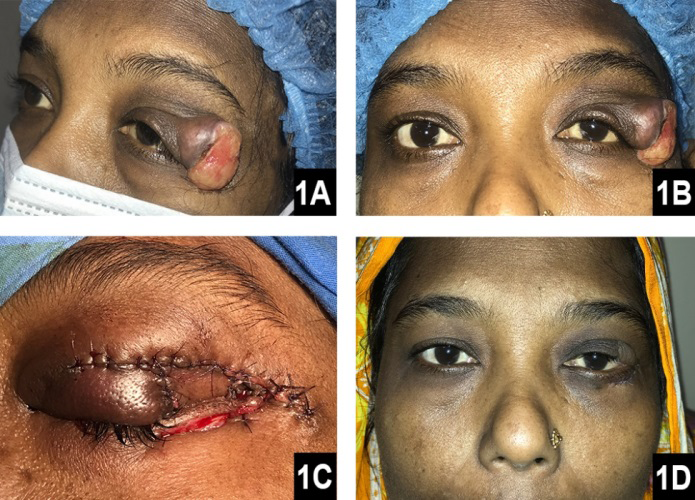
A & B: Presented with left upper eye lid lesion showing whitish pink excoriated surface. C: Immediate post-operative showing lid sharing by Cutler- Beard method D: After release of ankyloblepharon. Figure 1: Patients picture
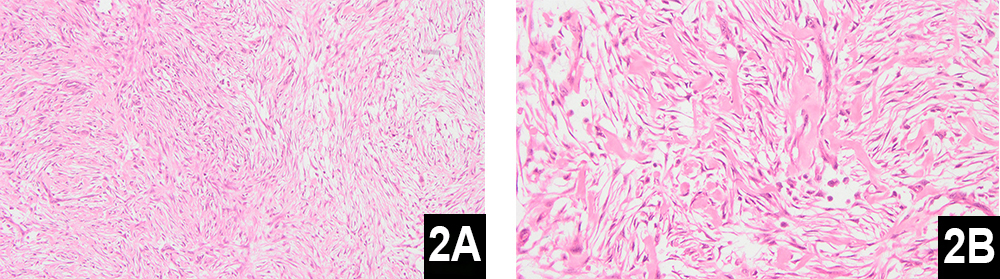
A: With eosin -hematoxylin stain showing the bundles of spindle cells in different direction in 10 x magnification. B: Eosinophilic cytoplasm with mildly basophilic stained nucleus of spindle cells and some lymphocytes in 20x magnification. Figure 2: Picture of histopathology
Discussion
The nature of rapid growth, morphological features and rarity of nodular fasciitis in ocular and periorbital area makes physician confused and raised suspicion of malignancy. The exact etiology is unknown but trauma is thought to be inciting factor though this is considered now unlikely. In literature, analysis of 23 cases showed only one case had history of trauma and one had history of localized infection [11].
Recent cytogenetic analysis found the peculiar and sometimes malignant behavior of nodular fasciitis is due to USP6 rearrangements. USP gene is located on chromosome 17p13 which is encoding for ubiquitin-specific proteases [9]. Among different genes MYH9 gene is the commonest USP6 fusion partner and Erickson-Johnson et al. reported a rearrangement of USP6 in 92% of nodular fasciitis [12].
This disease can occur at any age but young adult (20 to 40 years) is mostly affected without any sex predilection. The site of lesion also depends on age. In adults, 46% lesions are found in upper extremities, 20% in trunk and 18% in neck. In children, there is female predominance and lesions are mostly located in head, neck and maxillofacial region [7]. Generally, the size of lesion is less than 3 cm but can grow up to 7 cm and in eye the lesion is usually round to oval with a size of 0.5 to 1.5 cm [10, 11]. Our case was a 46 years old lady presented with an oval upper eye lid lesion which was about 3 cm in size which is bigger than usual size of eye lesion. The largest and first reported series of ocular (adnexal and orbital) nodular fasciitis was of 10 cases which was reported by Font and Zimmerman in 1966 [13].
Diagnosis of this lesion are based on morphological and histopathological features and role of immunohistochemistry is limited but USP6 rearrangement can be confirmed by FISH, PCR or next generation sequencing [10]. Imaging findings are also non-specific but in CT scan the lesions near bone may show bony remodeling or bone erosion [7, 10].
Though morphologically sometime it mimics as sarcoma and histologically is also confused with sarcoma as some reactive lesions in nodular fasciitis and ischemic fasciitis may show a cut off proliferating fibroblasts that surround a central hypocellular zone of fibrinoid change [14]. In such cases it’s diagnosis can be made on the basis of microscopic features by most experienced pathologists. The features of nodular fasciitis are:
- finely tapered spindle cells that resembled fibroblasts found in tissue culture,
- fibroblast with large vesicular nuclei and or prominent nuclei but never hyperchromatic,
- cytoplasmic basophilia and
- atypical mitoses are virtually never seen [5, 14].
Treatment of nodular fasciitis depends on location and size. This lesion may regress spontaneously, that’s why small lesion of face can be kept in observation which will reduce the chances of scar formation. Most authors suggest surgical excision of the lesion [7]. In incomplete excision, there is chances of recurrence of less than 5% and subtotal excision is recommended in close proximity of sensitive structures as the residual lesion will regress spontaneously [7, 15]. There are other non-surgical options of treatments such as, intralesional triamcinolone injection a carbon dioxide (CO2) laser. These options work on superficial lesion and usually used on face lesion [16].
Conclusion
Though nodular fasciitis is rare in ocular adnexal and orbital region, it may keep as differential in any rapidly growing lesion. Diagnosis of the disease is also important to avoid unnecessary aggressive treatment.
References
-
Ranschaert E, Thibodeau R, Knipe H (2024) Nodular fasciitis. Reference article, Radiopaedia.
-
Konwaler BE, Keasbey L, Kaplan L (1955) Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin Pathol 25(3): 241-252.
-
Martínez-Blanco M, Bagán JV, Alba JR, Basterra J (2002) Maxillofacial nodular fasciitis: a report of 3 cases. J Oral Maxillofac Surg 60(10): 1211-1214.
-
Lee YJ, Kim SM, Lee JH, Jun YJ, Kim YJ, et al. (2014) Nodular Fasciitis of the Periorbital Area. Arch Craniofac Surg 15(1): 43-46.
-
Riffle JE, Prosser AH, Lee JR, Lynn JJ (2011) Nodular fasciitis of the orbit: a case report and brief review of the literature. Case Rep Ophthalmol Med 2011: 235956.
-
Shimizu S, Hashimoto H, Enjoji M (1984) Nodular fasciitis: an analysis of 250 patients. Pathology 16(2): 161-166.
-
Liua RT, Henkelmanb E, Popescuc O, Yin VT (2019) Nodular fasciitis: A rapidly enlarging destructive periorbital mass in an infant. American Journal of Ophthalmology Case Reports 13: 119-121.
-
Spinelli N, Khorassani N (2013) Nodular Fasciitis: An Uncommon Disease with Common Medical Management Challenges at a Remote Naval Hospital. Military Medicine 178(9): e1051-e1054.
-
Balko J, Stanek M, Krskova L, Zamecnik J (2024) Unusual fusion gene rearrangements in patients with nodular fasciitis: a study of rare and novel USP6 fusion partners with a review of the literature. J Clin Pathol 77(6): 411- 416.
-
Dickson BC (2024) Nodular fasciitis.
-
Massop DJ, Frederick PA, Li HJ, Lin A (2016) Epibulbar Nodular Fasciitis. Case Rep Ophthalmol 7(1): 262-267.
-
Erickson-Johnson MR, Chou MM, Evers BR, Roth CW, Seys AR, et al. (2011) Nodular fasciitis: a novel model of transient neoplasia induced by MYH9-USP6 gene fusion. Lab Invest 91(10): 1427-1433.
-
Font RL, Zimmerman LE (1966) Nodular fasciitis of the eye and adnexa. A report of ten cases. Arch Ophthalmol 75(4): 475-481.
-
Husain N, Verma N (2011) Current Concepts in Pathology of Soft Tissue Sarcoma. Indian J Surg Oncol 2(4): 302- 308.
-
Pasternack MS, Swartz MN (2015) 95 - Cellulitis, Necrotizing Fasciitis, and Subcutaneous Tissue Infections. In: Bennett JE, et al. (Eds.), Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 8th(Edn.), Philadelphia, pp: 1194-1215.
-
Oh BH, Kim J, Zheng Z, Roh MR, Chung KY (2015) Treatment of Nodular Fasciitis Occurring on the Face. Ann Dermatol 27(6): 694-701.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report