Orthokeratology-A Historical Summary and Update
Objective: To present a comprehensive review of current and historical literature of orthokeratology treatment and lens technology. Methods: A summary of the history of orthokeratology lenses was compiled through literature research from a selection of databases. A summary of contact lens materials, corneal topography and associated lens design is presented. The history of orthokeratology is presented as well as developmental milestones since its inception. Orthokeratology appears to be a safe form of vision correction. Conclusions: Orthokeratology appears to be a safe form of contact lens correction for refractive errors. The advancement in lens design, contact lens manufacture and corneal topography has greatly aided its acceptance as a treatment modality of refractive errors.
Lallu J¹* and Wood J²
¹MSc Specialty Contact Lenses (Hons), The University of Auckland, New Zealand ²Graduate Optometrist, The University of Auckland, New Zealand Keywords: Orthokeratology; Cornea; Lens Design
Abbreviations
VST: Vision Shaping Treatment; CRT: Corneal Refractive Therapy; CAB: Cellulose Acetate Butyrate; FDA: Food And Drug Administration; OCT: Optical Coherence Tomography; DIMS: Defocus-Incorporated Multiple Segment Spectacle Lenses; CRTH: Corneal Refractive Therapy for Hyperopic Refractive Errors; AFZ: Adjacent Flat Zone; ASZ: Adjacent Steep Zone; SCL: Soft Contact Lenses.
Introduction
Orthokeratology is defined as the process where the superficial layers of the cornea are reshaped through programmed use of rigid contact lenses worn overnight [1]. The effect is used to correct spectacle refractive errors. The technique is reported to be successful in the correction of hyperopia, presbyopia, astigmatism, and myopia. However, conflicting reports of design and fitting philosophy affected reproducibility which meant that published orthokeratology research focused primarily on the correction of myopia. The development of reverse geometry lens designs coupled with the development of high Dk (oxygen permeability) lens materials was pivotal in the resurgence of orthokeratology in the 1990’s. Since 2006 when Helen Swarbrick [2] reviewed orthokeratology, our knowledge has further increased. There still appears to be significant disparities regarding current practitioner techniques in terms of the duration of the treatment, side effects long term, maximum and minimum prescription ranges, and long-term safety. Concurrent advancements in corneal surface measurement and rigid lens manufacture have brought us to the current clinical picture. This review serves as an introduction to what orthokeratology is, basic orthokeratology lens design, and the current safety profile.
History of Orthokeratology
In 1888, Eugene Kalt described the flattening of a keratoconic cornea using a contact shell [3]. This is believed to be the first report in literature of attempted shape manipulation of the cornea following lens fitting [3]. In 1962, Jessen described the “orthofocus technique” where a lens could be fitted relatively steep or relatively flat to alter the corneal curvature and vision of the contact lens wearer [4]. Steepening the cornea eliminated the hyperopic refractive error correction, while flattening the cornea corrected myopia [4]. At that time, eyelid pressure was the then proposed mechanism for this effect. This pressure helped in moulding the cornea to the shape of the contact lens [4]. The “orthofocus technique” was later named Orthokeratology, shortened to Ortho-K and is also known as vision shaping treatment (VST) or corneal refractive therapy (CRT).
Orthokeratology requires specially designed rigid contact lenses to reversibly alter the contour of the cornea thereby temporarily altering the refractive error. Key measurements to determine the effect of orthokeratology initially included: slit lamp biomicroscopy, keratometry, visual acuity, refraction, and contact lens assessment using sodium fluorescein. Between 1964 and 1980, a group of practitioners such as Grant, May, Neilson, Nolan, Ziff , et al. [5, 6, 7] developed and refined the fitting of these lenses. By 1980, the limits of refractive correction were up to a maximum of 4.00 dioptres (D) of myopia, 2.50 D of astigmatism and 2.00 D of hyperopia. The parameters available for modification and control of the orthokeratology effect on refractive error were: base curve, lens diameter and optic zone size. Results took from two weeks to eight months to develop. The technique required the use of polymethylmethacrylate (PMMA) lenses worn during the day with “lens free” vision in the afternoon. Lenses were not worn overnight at this point in time due to the concern of oxygen transmissibility of PMMA lenses. Patients were typically reviewed six weekly [6].
In 1983, The Berkeley Orthokeratology Study evaluated the efficacy and safety of orthokeratology, studied the mechanism of refractive correction, the duration of effect, and reviewed pre-disposing factors for success and complications associated with corneal refractive therapy [8, 9, 10]. Eighty subjects were enrolled in a randomized controlled trial where the treatment group were fitted with orthokeratology lenses and controls wore rigid contact lenses not designed to alter corneal curvature. The visual and ocular characteristics were monitored for eighteen months, though, approximately twenty five percent of the subjects failed to complete the study or were lost to follow-up from both groups total. This compares well with other studies where the range can vary from 18-30% [11, 12]. Significant changes in refraction were noted in the orthokeratology group versus the conventional wear group (1.01 ± 0.87 D versus 0.54 ± 0.58 D p = 0.02).
The key conclusions from The Berkeley Orthokeratology Study were that lens thickness, base curve to cornea relationship, and diameter were the lens factors that had the most significant effect on treatment outcome. A treatment of 1.00 dioptre of myopia was reasonable and the orthokeratology change was reversible. They found no indication of clinically significant adverse effects, but concluded orthokeratology patients require close follow-up. Visual acuity was unstable when lenses were removed from day to day and this was more variable with patients who had a higher refractive error. The authors suggested that methods to maintain stable vision whilst wearing lenses needed to be further refined.
In 1984, Coon evaluated the Tabb method, which involved fitting a lens steeper than the flattest keratometry reading with manipulation of the optic zone diameter to achieve reduction of myopic refractive error [2, 7]. The use of a slightly steep orthokeratology lens minimised unwanted astigmatism and aided lens centration. Up to this point flatter lenses were used to create the orthokeratology effect [13]. However, two key disadvantages of gradually fitting flatter lenses were the number of lenses required and superior displacement of the lens on the eye [13]. Tabb’s technique sought to solve the centration issue [13, 14] Tabb suggested an alternative theory to Jessen, principally that a post lens tear reservoir in steep fitting lenses created ‘a balance between the positive and negative forces of the lens cornea system’ [14]. Tabb’s theory was that corneal shape change in orthokeratology was due to pressure differentials formed within the post lens tear film, rather than direct moulding of the cornea to the contact lens shape [14, 15].
Other Historical Milestones Relating to Orthokeratology up Until the 1990’s
Materials
PMMA was the main lens material in use until 1973 when cellulose acetate butyrate (CAB) was purposed for contact lens use [16]. PMMA contact lenses were impermeable to oxygen and induced hypoxic changes in most patients even in in open eye wear [16]. In 1986, the Food and Drug Administration (FDA) approved Paragon Paraperm material for extended wear. Before long, safe overnight wear of the conventional RGP lens was adopted and a resurgence in orthokeratology developed with the aim of wearing lenses overnight to achieve clear unaided vision during the day [16].
Topography
Keratometry was the main method for measuring induced corneal effects in early orthokeratology. However, keratometry only measures the central 3mm of corneal curvature accurately and the spacing of the keratometry mires are not accurate enough to depict the corneal change observed. The keratometer was unable to accurately compare the pre-treatment corneal topography to the post treatment mire change. The first computerised instrument for assessing corneal shape was the photo electronic keratoscope which was developed in the mid 1970’s Carney LG, et al. [17] however, its clinical use was limited by cost and because it was difficult to use in standard clinical practice. By the mid 1990’s, the modern computerised corneal topographer was developed which allowed corneal topographical changes due to lens wear to be analysed and reviewed Kanpolat A, et al. [18]. Even today, there is little written in the literature about normal topographical data with respect to baseline validation. In 1997, Kanpolat measured 114 normal corneas of 114 emmetropic patients and found in their population the following breakdown of topographic patterns; “asymmetric bow tie topography patterns were the most common (33%), followed by symmetric bow tie (29%), round (14%), irregular (12%), and oval (11%) patterns” Topuz H, et al. [19] (Figures 1 & 2). The authors concluded that the algorithm used by the EyeSys topographer to produce a topography map may not be accurate enough to determine the true shape of the corneal surface for reconstruction. The shape of the cornea tends to change with age, and a more recent paper concluded that the normal cornea becomes steeper in the horizontal meridian and superior vertical quadrant and shifts from with-the-rule astigmatism to against-the- rule astigmatism with age, however, the overall amount of physiological corneal astigmatism does not change with age [20].
![Figure 2: Corneal topography pattern of a symmetrical bow-tie cornea. It is important to understand that corneal topographer indices are not interchangeable with different manufacturers and different models. In a young Chinese population, Pauline Cho evaluated the performance of four topographers (Humphrey Atlas 991, Orbscan II, Dicon CT200, Medmont E300) and concluded that apical radius and eccentricity cannot be used interchangeably between machines in the calculation of orthokeratology lenses [21]. When comparing the apical radius, eccentricity, and elevation measures, the Orbscan II performed the poorest. Meaning the experiment compared apical radius, eccentricity and elevation where applicable between the machines, the Medmont E300 and the Humphrey Atlas 991 provided the most repeatable and reproducible measures of apical radius and eccentricity. For better first fit success the authors suggest that practitioners take repeated scans so that the practitioner has a more accurate representation and understanding of the cornea prior to treatment. They also found that the number of repeated readings that should be taken for a precision of 2 µm (elevation) were 12 measurements for the Humphrey but only 2 measurements for the Medmont.](/fulltextimages/13652/fig_2.png)
Figure 2: Corneal topography pattern of a symmetrical bow-tie cornea. It is important to understand that corneal topographer indices are not interchangeable with different manufacturers and different models. In a young Chinese population, Pauline Cho evaluated the performance of four topographers (Humphrey Atlas 991, Orbscan II, Dicon CT200, Medmont E300) and concluded that apical radius and eccentricity cannot be used interchangeably between machines in the calculation of orthokeratology lenses [21]. When comparing the apical radius, eccentricity, and elevation measures, the Orbscan II performed the poorest. Meaning the experiment compared apical radius, eccentricity and elevation where applicable between the machines, the Medmont E300 and the Humphrey Atlas 991 provided the most repeatable and reproducible measures of apical radius and eccentricity. For better first fit success the authors suggest that practitioners take repeated scans so that the practitioner has a more accurate representation and understanding of the cornea prior to treatment. They also found that the number of repeated readings that should be taken for a precision of 2 µm (elevation) were 12 measurements for the Humphrey but only 2 measurements for the Medmont.
In summary, the development of corneal topography, rigid lens materials, and orthokeratology design discussed above were all required in order for accelerated overnight orthokeratology to exist.
Accelerated Orthokeratology
Conventional (non-orthokeratology) back surface contact lens designs are usually depicted as a series of progressive curves flatter than the centrally aligned back optic zone radius. In contrast, the reverse geometry design for myopic orthokeratology features a central optic zone fitted flatter than flat K (Figure 3-5). The next zone is steeper and is termed the reverse curve(s). Peripheral to the reverse- curve(s) is a flatter curve fitted for corneal alignment and a final peripheral curve is often used to provide edge lift. The peripheral alignment curve controls the overall lens fitting by supporting the weight of the lens in the periphery [2]. Whereas in 1972, Fontana invented the one piece bifocal contact lens, which attempted to create a flatter central base curve however, the lathe technology at the time could not create the lenses as desired, and it was not until the late 1980’s that computers began controlling manufacturing lathes.
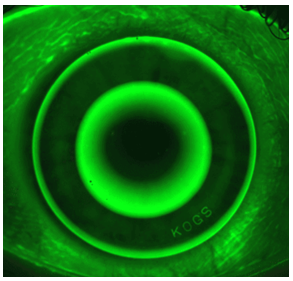
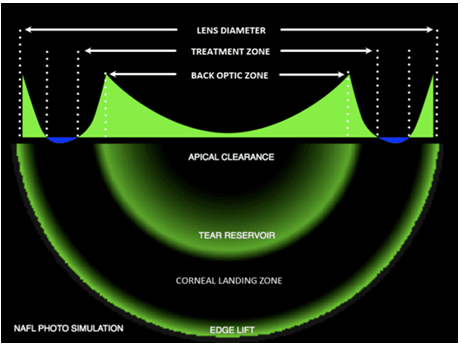
Figure 4: A schematic of the different curves of myopic orthokeratology lenses. This features a central back optic zone fitted flatter than flat K. There is then a steeper zone known as the reverse curve (tear reservoir), followed peripherally by a flatter curve for corneal alignment (corneal landing zone). The final most peripheral curve is the edge lift.
In 1989, Wlodyga and Bryla and independently in 1992 Stoyan and Harris outlined the use of reverse geometry lenses in orthokeratology [22, 23]. Accelerated orthokeratology showed vastly superior treatment times when compared to the Berkeley Orthokeratology Study; a -4.00 D refractive change could now be achieved with one pair of contact lenses. In 1997, John Mountford proposed an arguably more scientific lens design whereby the sag of the lens was equal to the sag of the cornea over a specified chord length plus 10 um in order to avoid lens bearing. The key difference between the Mountford lens design and its predecessors was that a unique lens was designed where the corneal eccentricity differed over a known chord of the same corneal curvature. This new design relied on two elements:
1) The corneal topographical information collected was accurate 2) The secondary steepening curve was spherical Furthermore, Mountford was able to show that corneal eccentricity could be used as a good predictor for the amount of myopic correction with orthokeratology lens wear using the BE system. Squeeze film pressure - which is defined as the force a fluid places on a surface under compression. A positive force is noted where the film is thickest and a negative force where the film is thinnest.
- Eccentricity – a lower eccentricity will predict a lower refractive change therefore limiting the range of correctable refractive errors.
- Epithelial displacement and treatment zone size - the epithelium has a maximum compressibility of 20 microns and with this there is an associated maximum theoretical treatment zone size for any given prescription.
Using this information Mountford demonstrated that a 0.22 eccentricity increment correlated to a 0.75 dioptric reduction in myopia [24]. Since 2000, there has been considerable further research into applications of orthokeratology with a plethora of new designs to achieve treatment of myopia control, hyperopia, post LASIK, high myopia and astigmatism [8, 25, 26, 27].
| Decade | Contact lenses | Technology | Orthokeratology |
|---|---|---|---|
| 1970’s | PMMA and CAB lenses available | Photo electronic keratoscope developed | Refinement and renaming of orthofocus by Ziff, Grant, May, Neilson, Nolan |
| 1980’s | Overnight GP lenses available and approved by FDA. Fluorosilicon acrylate material invented | Corneal videokeratoscopes for sale ~$85,000 USD | Berkeley Orthokeratology study, Tabb review by Coon |
| 1990’s | Marketing of contact lenses | Modern corneal topographer developed | Accelerated Orthokeratology technique described and indication for overnight wear |
| 2000’s to 2020 | Overnight orthokeratology approved by the FDA Menicon Z approved for overnight wear for 30 days | Latest generation of topographers combining OCT technology developed. Current video keratoscopes are around 1/5th the price they were when first released. | Research on going into the development of novel designs to treat a wide variety of prescriptions. |
Table 1: Summary of the relevant history between contact lens materials, corneal evaluation using topographers and orthokeratolog
Mechanism of Refractive Correction in Myopic Orthokeratology
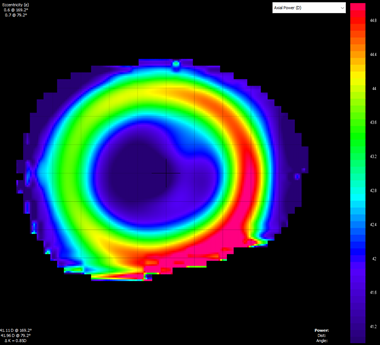
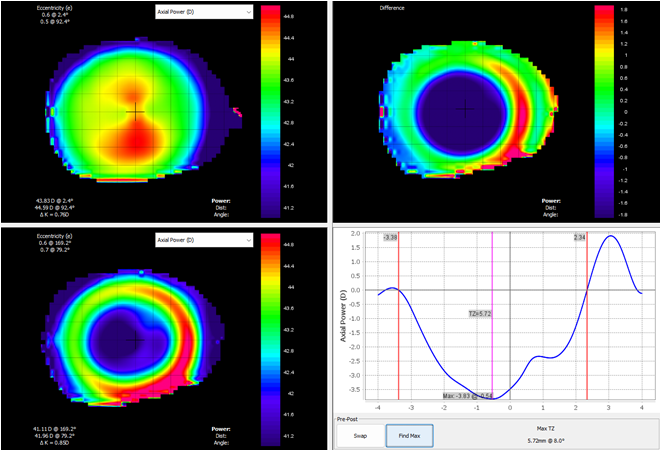
It is now commonly accepted that the corneal epithelium is the primary structure undergoing change in low myopic orthokeratology. The corneal epithelium has been examined histologically Choo JD, et al. [1], with optical pachometry and optical coherence tomography (OCT) [28, 29, 30]. Using all these technologies, epithelial thinning is noted centrally following lens wear. Some reports show stromal thickening, however, this comprises less than one third of epithelial thinning [31]. Epithelial thinning corresponds to myopic refractive error on corneal topography, whilst areas of epithelial thickening correspond to hyperopic refractive error change. (Figure 6-8).
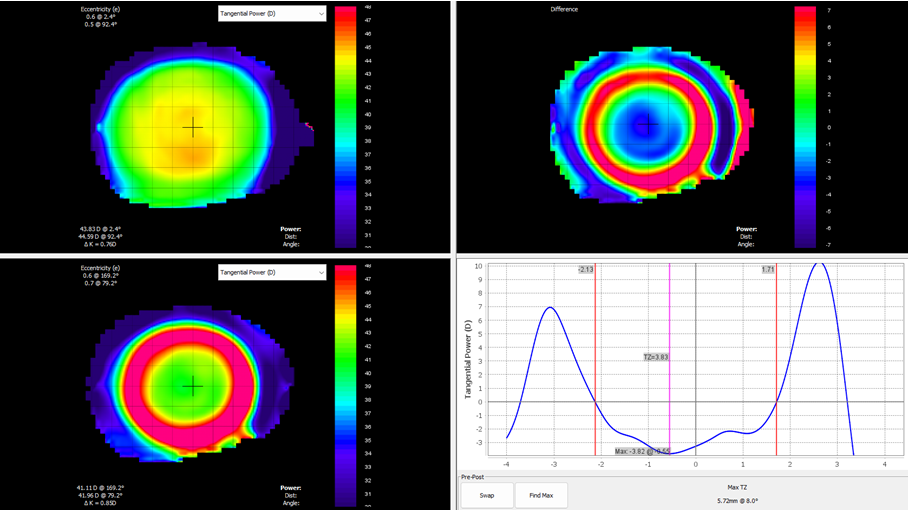
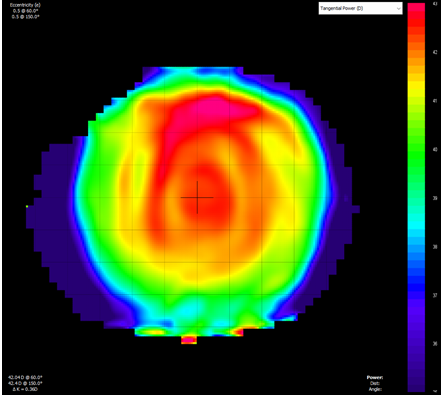
Figure 6: Tangential power difference map that describes instantaneous curvature of the cornea. The top left map is the pre-fitting map whilst the bottom left map is following orthokeratology lens wear. This shows where a lens has landed on the eye. Blue areas indicate flattening (bearing) whilst steep areas (reverse curve) are indicated in red. This does not show the refractive optics of the eye.
The construction of an orthokeratology lens can be simplified into two groups; traditional designs and modern reverse geometry designs. Traditional designs can be described as steep or flat curved lenses with a peripheral curve or curves that were manipulated in an effort to maintain stabilisation and centration. Modern “reverse geometry” lenses consist of a central base curve, which is fit flatter than the corneal curvature in most designs, following by a series of peripheral curves. The key design alteration from traditional designs is the addition of a “reverse curve zone” that is generally significantly steeper than the base curve and acts as a tear reservoir. The base curve is responsible for a positive force and the creation of a pressure differential between the centre and reverse curve. The alignment curve zone is responsible for the position of the lens on the eye and is usually between 1.0 mm and 1.5 mm in width and may be spherical, aspherical or tangential in nature. The peripheral curve is the final curve of the lens, responsible for edge lift and can vary from 0.40mm to 0.8mm wide across designs [32].
High Myopia Orthokeratology in Literature
There is keen interest in the correction of high myopia in orthokeratology as it has been reported that the higher spherical equivalent refractive error is associated with slower axial length elongation and in turn, control of myopia [33]. There are currently two approaches for the correction of high myopia with orthokeratology, the first involves the partial correction of high myopia with spectacle wear to “top-up” the uncorrected residual myopia [34]. A reported complication in the treatment of orthokeratology in higher degrees of myopia is the presence of corneal staining. This has been demonstrated on a prospective research project where group one had a target of -6.00 D correction and group two had a target of -4.00 D [35]. This leads to the conclusion that designing a lens for high myopia requires design consideration to mitigate an increase in corneal staining, presumably with more central clearance. The other involves utilizing custom designed “Off label” Orthokeratology lenses to target the entire high myopic spectacle prescription. The Orthokeratology for High Myopia study currently taking place in Hong Kong is undergoing recruitment and at the time of writing, 66 participants have been enrolled to evaluate the safety and efficacy of high myopia correction using the Euclid Topaz lens design. This is a new lens available commercially to correct up to 10 dioptres of myopia in highly myopia children. Clinical observations in high myopia and its correction with orthokeratology are optimistic. A prospective study in China of 30 high myopia patients (10M 20F) demonstrated stable correction of up to -7.34 +/- 0.91 D for a period of five years, with an observation of stable axial length control [36]. In Japan, researchers at Jyoto eye clinic evaluated 8 eyes of 5 patients with a spherical equivalent of between -6.00 and -9.00 D and mean -7.22 D concluding that orthokeratology for high myopia is an effective option for the treatment of high refractive error. In Malaysia, records of school children (age 7-17 years) were undergoing OK treatment, all patients noted significant reductions in refractive error, improvement in visual acuity and flattening of corneal curvature with a conclusion that high myopes with refractive power of up to -8.25 D would benefit significantly from OK lenses [27, 37] Orthokeratology in high myopia and astigmatism has also been demonstrated as being safe and effective of up to -6.00D [38, 39].
In 2024, a prospective study was conducted investigating the efficacy of orthokeratology for myopia control in 540 children aged 7 to 14 years compared to another spectacle method of myopia control using defocus-incorporated multiple segment spectacle lenses (DIMS) [40]. This study further divided patients into three groups based on their degree of myopia: low, moderate, and high myopia (classified as -3.00 to -5.00D) and compared axial length elongation over the course of a year. In both the moderate and high myopia group, orthokeratology was found to be significantly effective in slowing axial length elongation. More interestingly, orthokeratology was also found to be more effective in controlling axial length elongation when compared to DIMS lenses in patients with higher degrees of myopia.
Hyperopic Orthokeratology in Literature
Orthokeratology for low myopic prescriptions has been researched and FDA validated as being both safe and effective for spherical dioptric corrections of up to -5.00D and up to -1.50D with-the-rule astigmatism and -0.75D against-the-rule astigmatism. It has been suggested by the limited research base that low hyperopic prescriptions are achievable (up to +3.00 D), yet, there is currently limited research in this area and no time course on effectivity data past seven days [41, 42]. There is one pilot study following one month’s wear of a new design of orthokeratology lens [43]. Currently, there are only eleven clinical papers devoted to hyperopic orthokeratology, most of which were written after 2009 by Paul Gifford and co-workers at the University of New South Wales [25, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50].
In 2004, Swarbrick et al studied the effects of PMMA and Boston XO lenses fitted 0.3 mm steeper than flattest K. Significant corneal steepening over a 5-6 mm zone was noted in both materials, with the most significant change in corneal curvature in the mid-periphery (1.5-4.0 mm from the corneal apex). The corresponding refractive change in the central cornea was not significant and tended toward myopia. Significant central corneal oedema (8.2±2.2%) was found in eyes fitted with the PMMA lenses. Carney had previously identified that different patterns of change in corneal curvature arise from oedema versus moulding Holladay JT [51] and the primary factor responsible for the change was corneal moulding [47].
In 2007, Lu reviewed 20 patients (14 myopic, 4 hyperopic and 2 emmetropic) following one night’s wear of the CRT Hyperopia lens. The design used was a modified CRT myopia design where the initial base curve was selected as 0.7mm steeper than flattest K. The reverse curve zone was set 175µm deeper than the slide rule recommendation for myopia because the hyperopic treatment zone was set at 5mm (CRT myopia is set at 6mm). The authors were able to show that a hyperopic orthokeratology effect could be achieved with recovery to baseline within 28 hours of ceasing wear. The treatment group showed a refractive error change of 1.23±0.21 D following wear whilst the control group showed no significant refractive change.
Spherical aberration is often discussed in refractive surgery and the aim is to reduce this to zero Koffler BH, et al. [52] to improve visual acuity. Decentration of the optics will also create aberrations and decrease optical performance. In cataract surgery, decentration of the intraocular lens will tend to create coma. It is therefore important to be precise when correcting higher order aberrations.
The normal cornea has negative spherical aberration (SA), and the crystalline lens shifts from negative SA to positive SA with age. Hyperopic orthokeratology in Lu’s study induced more negative spherical aberration. Given the natural aging of the lens, this could be beneficial to the overall optics of the eye with respect to presbyopic hyperopic correction, by reducing overall spherical aberration. A cause for this could be uneven epithelial distribution from the treatment. An increase in coma was reported, the authors suggest that this is because of the decentration of the treatment effect within subjects [48].
In 2008 Gifford studied the hyperopic effect of orthokeratology lenses over a 7-day time course. Initially, 10 subjects 1 hyperopic, 3 emmetropic, and 6 myopic) wore a lens designed to achieve a +1.50 D refractive change. In the second phase eight participants continued in the study to wear a lens of +3.50 D target power. The results demonstrated that the hyperopic effect was most likely related to mid peripheral thinning. This may limit the viable treatment range of this modality as most of the refractive change in both phases was noted after day 1. The lens design may also affect the outcome of the refractive target. The +3.50 D target lens “achieved 56% (95% confidence intervals CI±27% of its intended refractive change at lens removal on day 7, reducing to 40% (CI±23%) 8 hours later”. The hyperopic effect on epithelium is in agreement with histological studies of cat epithelia which found thickening of the central epithelium and thinning of the mid-peripheral epithelium with increased lens wear time [1]. The +3.50 D target power group showed more variability at day 7 than the +1.50 D power group. Most of the refractive and topographic change occurs after the first night of wear with regression during the day but greater retention of effect by day 7 [42].
The conclusions of this study showed that hyperopic orthokeratology is a viable treatment option for low levels of hyperopia. However further work needs to be carried out to ascertain the reasons for treatment effect variation between individuals. The treatment effect appears to be analogous to myopic orthokeratology within the first week of wear, with most of the refractive change occurring in the first night of wear.
Lu reported on the malleability of the cornea and optical properties between CRT (Corneal Refractive Therapy for correction of myopic refractive errors) and CRTH (Corneal Refractive Therapy for hyperopic refractive errors) lens designs. The most malleable cellular layer was noted to be the epithelium when sandwiched between the rigid lens and Bowman’s layer. Whilst both CRT and CRTH demonstrated the ability to correct refractive error, the effect from the CRTH lens design was noted to be only approximately 2/3 the efficacy of the myopic design within the same testing period probably due to the design of the contact lens. Rapid steepening and flattening was noted in little time for the correction of myopia with orthokeratology lenses [45].
The mechanism for corneal reshaping in hyperopic orthokeratology was investigated in 2009. Twelve myopes were fitted with hyperopic orthokeratology design lenses and their response measured following an hour of wear and then overnight wear. It was concluded that a general corneal moulding effect may be the primary change causing central steepening. This was further assessed by applying fenestrations to the orthokeratology lenses and assessing any clinical difference. It was noted that the central corneal curvature closely correlated to spherical equivalent refraction when fenestrations were applied. This and other anecdotal evidence indicates that there could be an element of both a paracentral moulding effect and a shape change aiding the conformation to the central base curve of the lens [49].
The BE hyperopic orthokeratology lens design was used to assess the differences in the size of the treatment zone comparing myopia and hyperopic orthokeratology. The treatment zones in hyperopic orthokeratology were defined via tangential difference maps to comprise of a central steep zone (CSZ) with an adjacent flat zone (AFZ). In contrast, myopic orthokeratology has a central flat zone (CFZ) with an adjacent steep zone (ASZ). When comparing the outcomes, it was noted at both day one and day seven the hyperopic treatment zone was smaller and tends to become even smaller, whilst the AFZ tends to get larger. Conversely in myopic orthokeratology treatment the CFZ and ASZ become larger with time and this has been attributed somewhat to the shape of the back surface of the lens. For an improvement in the treatment effect of hyperopic orthokeratology an increase in the diameter of the CSZ will be required [44].
Hyperopic orthokeratology has also been used to create monovision correction for presbyopic patients. Sixteen adult emmetropic presbyopes were fitted with BE Orthokeratology lenses in one eye only for seven nights designed to create a target prescription of +2.00 D, in one eye only for seven nights. Thirteen participants completed the study with the other three discontinuing due to lens discomfort following the first nights wear. Results showed an improvement in monocular near visual acuity without degradation of binocular distance visual acuity in all cases. A greater retention of effect was noted at day seven (eight hours following morning appointment). Distance visual acuity in the corrected eye did not drop in relation to the refractive change with the authors suggesting this was due to the multifocal effect (centre near) created with hyperopic orthokeratology [26]. In 2019 a prospective pilot study including 8 hyperopic eyes of 4 non-presbyopic patients aged between 22 and 44 years of age were fit with the Alexa H contact lens, this is an aspheric 5-curve design. Main conclusions were that hyperopic correction is achievable with orthokeratology and there is an increase in negative Q and spherical aberration with central corneal steepening [43]. Fitting guides for Hyperopic Orthokeratology must be improved to avoid suboptimal outcomes such as central volcanoes, decentration and incomplete treatment. A summary table of relevant research related to hyperopic orthokeratology is supplied as appendix A.
Safety
Between 1997 and 2007 there were 123 reported cases globally of microbial keratitis associated with orthokeratology use [53]. In 2007, the Singapore National Eye Centre presented a five-patient case series suggesting an association of pseudomonas aeruginosa infection with overnight orthokeratology lens use [54]. In 2008, the American Academy of Ophthalmology reviewed seventy- five articles investigating the safety of orthokeratology and concluded that ‘‘future research should be directed at assessing the rate of infectious keratitis among overnight orthokeratology users and whether the rate varies by age” [55]. In 2010, a Canadian study presented three cases of keratitis related to overnight orthokeratology lens use [56]. Choo, et al. studied pseudomonas and infection rates on cat epithelia and compared alignment fit and orthokeratology lenses [57]. In order to elicit a infectious response with overnight orthokeratology lens wear the lenses had to be soaked in pseudomonas and a corneal abrasion present, whereas lenses soaked and worn in the absence of corneal trauma, showed no significant increase in risk [57]. Bullimore et al concluded that the overall estimated incidence of microbial keratitis is 7.7 per 10,000 years of wear (95% CI = 0.9 to 27.8) whilst the estimated incidence of microbial keratitis is nearly twice as high (13.9 per 10,000 patient- years 95% CI = 1.7 to 50.4) in children [58]. This contrasts to adults, where the estimated incidence of microbial keratitis is 0 per 10,000 patient-years (95% CI = 0 to 31.7) [58]. The fact that the confidence intervals for the rates estimated overlap should not be interpreted as evidence of no difference [58].
Key factors in complications include poor patient knowledge of cleaning systems and hygiene. Systematic review into the safety of orthokeratology has included 170 publications by Yue and Xie where it was concluded that the most common complication was corneal staining and insignificantly there is corneal iron deposit [59]. A prospective study was carried out on the predictability and safety of orthokeratology in up to -5.50 D of myopia in semi- tropical countries [60]. The lens material chosen was Boston XO and the lenses were 10.6mm in diameter. No significant adverse events were noted [60]. Other materials including Boston XO2, XO and Menicon Z all appear to be safe when prescribing orthokeratology lenses. The main determinant of an adverse event appears to be clear patient direction on how to wear and take care of lenses followed by regular examination by the eye care professional [61, 62]. In China, the rates of compliance are not high and this will continue to be a main focus of practitioner and patient education [63]. Ten year review of the safety and efficacy of orthokeratology has now been published and compared complication rates to soft contact lenses (SCL) with no significant difference noted, with allergic conjunctivitis and acute conjunctivitis rates of incidence being similar (25/119 OK v 23/103 SCL) [64].
More recently in 2024, a Japanese study involving 1,438 patients (the largest sample size in current literature investigating the safety profile of orthokeratology) whom had worn orthokeratology lenses for at least three months was conducted [65]. In this study, only four cases of microbial keratitis were reported throughout the study period [65]. The incidence was found to be 5.4 per 10,000 patient- years amongst orthokeratology wearers [65]. The authors concluded that orthokeratology was found to be very safe with the incidence of microbial keratitis to be “comparable to that of daily wear soft contact lenses” [65]. Additional studies conducted in 2024 investigating the safety profile of orthokeratology further support these findings [66, 67]. These studies found no serious adverse effects amongst myopic children and also reported rates of microbial keratitis to being similar to that of daily soft contact lens wear [66, 67]. Some adverse events were reported however, most were found to be affecting the cornea, largely due to corneal staining and abrasions [66].
Orthokeratology has been reported to have an effect on the ocular surface in teenagers with myopia. Of note, following orthokeratology wear the tear meniscus height and tear secretion was observed following the wearing of OK lenses, with no corresponding change to the function of the meibomian gland [68].
However, this has been debated in recent literature. A study conducted in 2018 assessed tear film function parameters and bulbar redness in children following wear of orthokeratology lenses [69]. It was found that orthokeratology wear might affect the stability of the tear film in the short-term following lens wear. However, orthokeratology lens wear was not found to have induced any significant tear deficiency or bulbar redness following lens wear [69].
In 2023, a study was conducted investigating long-term changes in the ocular surface during orthokeratology lens wear [70]. It was found that orthokeratology lens wear did increase symptoms of ocular discomfort and decrease tear film function which correlated with each other following three months of wear. However, no infectious keratitis or other serious complications were reported Rah MJ, et al. [70]. More interestingly, it was found that these symptoms of ocular discomfort and tear film function parameters gradually restored again following three months of lens wear.
It has been suggested that corneal iron lines may be caused by hyperopic orthokeratology corrections over +3.50, with the current proposed mechanism being microepithelial trauma or irregular folding of the epithelium from irregular pooling of tear film beneath the contact lenses [50]. Other case series of iron line formation have concluded that this is a benign finding with no long term effect on visual acuity and physiology [68, 71]. The research is yet to report on their resolution following cessation of orthokeratology lens wear. There is a correlation between lens wear and intensity of pigmented arcs. An inferior location for a pigmented arc is more common. Customisation of the inferior portion of the reverse curve can lead to resolution [72]. Steeper and tighter more aggressive myopia reduction lens designs are positively correlated with more intense pigmented arcs [72, 73].
Discussion
This review has demonstrated that orthokeratology is becoming a more mainstream contact lens wear modality of choice for patients and practitioners alike. Significant advancements in contact lens manufacture, corneal measurement, and contact lens design have enabled practitioners to seek knowledge and train in this subspecialty area. Many optometry schools are teaching orthokeratology worldwide. More clinical resources are available via websites, textbook and interactive media (YouTube and Vimeo). Without significant technological advancement, this modality would have been limited to fringe practice. Clinically, we have found that practitioners are more cautious and fear infectious keratitis, however, rates of microbial keratitis appear low and, Keay et al have reported on the importance of risk factors and patient awareness with respect to hygiene [74]. Stapleton F, et al. have also reported on independent risk factors such as smoking and socioeconomic status [74]. As with soft lenses, key risk factors for the development of keratitis include: overnight use, patient compliance, hygiene and frequent lens solution replacement. The reality is that the incidence of microbial keratitis in orthokeratology patients is similar to soft contact lens wear [53, 58]. and concerns regarding infection rates in orthokeratology patients may be unfounded. Practitioners use a variety of systems including peroxides, daily cleaners, and in-house deep cleaning treatments such as Menicon Progent to help reduce the risks of adverse events. Designs are becoming more advanced and lead toward a bright future with respect to the limits of refractive correction. Clinical reports of successful correction of astigmatism, high myopia, and hyperopia using the modality now exist in the literature. Nevertheless, there is still need for larger studies to explore the effectiveness of various orthokeratology treatment modalities particularly in regard to time-course of corneal changes and limits of refractive correction.
High myopic patients may benefit from Orthokeratology treatment as there have been associations of increased axial length control related to higher amounts of spherical equivalent refractive error. The main complications of high myopic orthokeratology correction are corneal staining and more care must be taken in the design of lenses for this degree of ametropia. More prospective research would be useful to adequately show the clinical findings that practitioners are reporting versus the evidenced research available. A key step forward in this will be the results and conclusion of the Orthokeratology for High Myopia Study. Hyperopic refractive outcomes for the correction of presbyopia appear promising. Gifford et al noted a reduction of monocular distance visual acuity to 0.25 LogMAR (Snellen equivalent 6/9 – 6/12 or 20/30 – 20/40 vision) with no change in binocular distance acuity. Corresponding near visual acuity increased to Jaegar 3.2 (approximately equal to N5.5) compared with uncorrected near vision measurements. Near visual acuity improvement and distance visual acuity reduction did not correspond with the near addition prescribed. Near addition spectacle lenses in monovision reduce distance visual acuity at approximately one line per 0.25 D. Hyperopic orthokeratology allows binocular vision and also maintains stereopsis and this effect has been documented in aspheric hyperopic laser refractive surgery as welFl [74]. As with all other forms of presbyopic vision correction, orthokeratology lens fitting will alter spherical aberration. The current opinion in refractive surgery is to aim for zero spherical aberration. Hyperopic orthokeratology can be tailored to decrease spherical aberration toward zero with appropriate lens design. This could be a future innovation worthy of investigation.
The main limitation in the advancement of orthokeratology lens fitting lies with research. The research base is disparate when compared to the practitioner reporting of the breadth and depth of this sub-specialty and consists mainly of case studies and small case series. This
is particularly true of studies investigating the efficacy of hyperopic orthokeratology. All hyperopic orthokeratology studies are limited in patient numbers with no studies containing more than 20 participants in the treatment group. The refractive errors of the participants are rarely hyperopic with most studies primarily recruiting myopic or emmetropic participants and only small numbers of young hyperopic patients. This has potential implications to the clinical applicability of results particularly if there are differences between corneae of hyperopic and non-hyperopic individuals. There is lack of follow up past seven days of treatment whereas in primary care there are patients that have been followed for many years, but no published data exists for this group of patients. It is very difficult to design randomized masked control trials with orthokeratology as it is very difficult to mask corneal topographical outcomes from observers and treatment effect from patients. Case series need to be presented to stimulate research moving forward.
A potential solution to the need for more published research could be a more active engagement in multicentre optometry practices to enable publication of retrospective and prospective case series and studies. Technological advancement allows the use of cloud-based servers to store vast amounts of data safely and securely and to create masked trials. Using technologies like this could help to aggregate required informational statistics to gain a deeper understanding and to bridge the gap in literature that seems to be ever widening. By using this approach more research could be collected and analysed to answer questions such as global incidence of infection, limits of correction, safety and efficacy, and number of lenses to reach a desired clinical outcome.
With respect to hyperopic orthokeratology there is little in the literature regarding success rates, infection profile and time-course past one month. Practitioners report that hyperopic orthokeratology appears to be more complex to fit, however there is currently no evidence to support this claim. Many practitioners claim that the main orthokeratology effect in hyperopic orthokeratology does not reach stability until two or more weeks wear. This is yet to be reported on and is a natural progression for the development of hyperopic orthokeratology research. Practitioner engagement in research is key into its advancement.
Overall, orthokeratology appears to be a safe form of contact lens correction for refractive errors. Despite several unanswered questions this modality is growing in popularity. The advancement in lens design, contact lens manufacture and corneal topography has greatly aided its acceptance as a treatment modality of refractive error.
References
-
Choo JD, Caroline PJ, Harlin DD, Papas EB, Holden BA (2008) Morphologic changes in cat epithelium following continuous wear of orthokeratology lenses: a pilot study. Contact Lens and Anterior Eye; 31(1):29-37.
-
Swarbrick HA (2006) Orthokeratology review and update. Clin Exp Optom 89(3): 124-143.
-
Pearson RM (1989) Kalt, keratoconus, and the contact lens. Optom Vis Sci 66(9): 643-646.
-
Jessen GN (1962) Orthofocus techniques. Contacto 6: 200-204.
-
Ziff SL (1976) Orthokeratology. J Am Optom Assoc 47(3): 376.
-
Grant SC, Safir A (1980) Viewpoints-Orthokeratology. Waring GO, editor. Surv Ophthalmology pp: 291-297.
-
Coon LJ (1984) Orthokeratology. Part II: Evaluating the Tabb method. J Am Optom Assoc 55(6): 409-418.
-
Brand RJ, Polse KA, Schwalbe JS (1983) The Berkeley Orthokeratology Study, Part I: General Conduct of the Study. Am J Optom Physiol Opt 60(3): 175-786.
-
Polse KA, Brand RJ, Schwalbe JS, Vastine DW, Keener RJ (1983) The Berkeley Orthokeratology Study, Part II: Efficacy and duration. Am J Optom Physiol Opt 60(3): 187-198.
-
Polse KA, Brand RJ, Keener RJ, Schwalbe JS, et al. (1983) The Berkeley Orthokeratology Study, part III: safety. Am J Optom Physiol Opt 60(4): 321-328.
-
Swarbrick HA, Alharbi A, Watt K, Lum E, Kang P (2015) Myopia control during orthokeratology lens wear in children using a novel study design. Ophthalmology 122(3): 620-630.
-
Charm J, Cho P (2013) High myopia-partial reduction ortho-k: a 2-year randomized study. Optom Vis Sci 90(6): 530-539.
-
Dave T, Ruston D (1998) Current trends in modern orthokeratology. Ophthalmic Physiol Opt 18(2): 224- 233.
-
Coon LJ (1982) Orthokeratology: part I historical perspective. J Am Optom Assoc 53(3): 187-195.
-
Paul Gifford (20009) PhD thesis 25: 1-252.
-
Gardner HP, Fink BA, Mitchell LG, Hill RM (2005) The effects of high-Dk rigid contact lens center thickness, material permeability, and blinking on the oxygen uptake of the human cornea. Optom Vis Sci 82(6): 459-566.
-
Carney LG, Clark BA (1972) Experimental deformation of the in vivo cornea. Am J Optom Arch Am Acad Optom 49(1): 28-34.
-
Kanpolat A, Simşek T, Alp NM (1997) The evaluation of normal corneal topography in emmetropic eyes with computer-assisted videokeratography. CLAO J 23(3): 168-171.
-
Topuz H, Ozdemir M, Cinal A, Gumusalan Y (2004) Age-related differences in normal corneal topography. Ophthalmic Surg Lasers Imaging 35(4): 298-303.
-
Cho P, Lam AKC, Mountford J, Ng L (2002) The performance of four different corneal topographers on normal human corneas and its impact on orthokeratology lens fitting. Optom Vis Sci 79(3): 175-783.
-
Wlodyga RJ, Bryla C (1989) Wlodyga: Corneal molding: the easy way - Google Scholar. Contact Lens Spectrum.
-
Harris DH, Stoyan N (1992) A new approach to orthokeratology. Contact Lens Spectrum.
-
Mountford J (1997) An Analysis of the Changes in Corneal Shape and Refractive Error Induced by Accelerated Orthokeratology. ICLC 24: 128-144.
-
Gifford P, Swarbrick HA (2013) Refractive changes from hyperopic orthokeratology monovision in presbyopes. Optom Vis Sci 90(4): 306-313.
-
Cheung SW, Cho P, Chan B (2009) Astigmatic Changes in Orthokeratology. Optom Vis Sci 86(12): 1352-1358.
-
Xie P (2015) Orthokeratology for the high myopia and high astigmatism is worth watching. Zhonghua Yan Ke Za Zhi 51(1): 8-10.
-
Haque S, Fonn D, Simpson T, Jones L (2004) Corneal and Epithelial Thickness Changes After 4 Weeks of Overnight Corneal Refractive Therapy Lens Wear, Measured With OpticalCoherence Tomography. Eye & Contact Lens: Science & Clinical Practice 30(4): 1-5.
-
Nieto-Bona A, González-Mesa A, Nieto-Bona MP, Villa- Collar C, Lorente-Velázquez A (2011) Long-term changes in corneal morphology induced by overnight orthokeratology. Curr Eye Res 36(10): 895-904.
-
Nieto-Bona A, González-Mesa A, Nieto-Bona MP, Villa- Collar C, Lorente-Velázquez A (2011) Short-term effects of overnight orthokeratology on corneal cell morphology and corneal thickness. Cornea 30(6): 646-654.
-
Li F, Jiang ZX, Hao P, Li X (2015) A Meta-analysis of Central Corneal Thickness Changes With Overnight Orthokeratology. Eye Contact Lens 42(2): 1-146.
-
Caroline PJ (2001) Contemporary orthokeratology. Contact Lens and Anterior Eye 24(1): 41-46.
-
Fu AC, Chen XL, Lv Y, Wang SL, Shang LN, et al. (2015) Higher spherical equivalent refractive errors is associated with slower axial elongation wearing orthokeratology. Cont Lens Anterior Eye 39(1): 62-66.
-
Charm J, Cho P (2013) High Myopia–Partial Reduction Ortho-k. Optometry and Vision Science 90(6): 530-539.
-
Lyu T, Wang L, Zhou L, Qin J, Ma H, et al. (2020) Regimen Study of High Myopia-Partial Reduction Orthokeratology. Eye Contact Lens 46(3): 141-146.
-
Zhou J, Xie P, Wang D, Guo X, Yang L (2015) The long- term clinical effects of orthokeratology in high myopia children]. Zhonghua Yan Ke Za Zhi 51(7): 515-519.
-
Liong SL, Mohidin N, Tan BW, Ali BM (2015) Refractive error, visual acuity, and corneal-curvature changes in high and low myopes with orthokeratology treatment: A Malaysian study. Taiwan Journal of Ophthalmology 5(4): 164-168.
-
Luo M, Ma S, Liang N (2015) Clinical efficacy of toric orthokeratology in myopic adolescent with moderate to high astigmatism. Eye Sci 29(4): 209-218.
-
Pauné J, Cardona G, Quevedo L (2012) Toric double tear reservoir contact lens in orthokeratology for astigmatism. Eye Contact Lens 38(4): 245-2451.
-
Lu W, Ji R, Jiang D, Shi L, Ding W, et al. (2024) Different efficacy in myopia control: Comparison between orthokeratology and defocus-incorporated multiple segment lenses. Cont. Lens Anterior Eye 47(2): 102122.
-
Gifford P, Alharbi A, Swarbrick HA (2011) Corneal thickness changes in hyperopic orthokeratology measured by optical pachometry. Investigative Ophthalmology & Visual Science 52(6): 3648-3653.
-
Gifford P, Swarbrick HA (2008) Time course of corneal topographic changes in the first week of overnight hyperopic orthokeratology. Optom Vis Sci 85(12): 1165- 1171.
-
Sánchez-García A, Batres-Valderas L, Piñero DP (2019) Orthokeratology With a New Contact Lens Design in Hyperopia: A Pilot Study. Eye & Contact Lens: Science & Clinical Practice 46(3): e17-e23.
-
Gifford P, Swarbrick HA (2009) The effect of treatment zone diameter in hyperopic orthokeratology. Ophthalmic and Physiological Optics 29(6): 584-592.
-
Lu F, Simpson T, Sorbara L, Fonn D (2008) Malleability of the ocular surface in response to mechanical stress induced by orthokeratology contact lenses. Cornea 27(2): 133-141.
-
Sorbara L, Lu F (2011) Corneal Refractive Therapy Gas Permeable Lenses for the Correction of Hyperopia After One Night of Lens Wear. Eye & Contact Lens: Science & Clinical Practice 37(1): 26-30.
-
Swarbrick HA, Hiew R, Kee AV, Peterson S, Tahhan N (2004) Apical clearance rigid contact lenses induce corneal steepening. Optometry and Vision Science 81(6): 427-435.
-
Lu F, Sorbara L, Simpson T, Fonn D (2007) Corneal Shape and Optical Performance After One Night of Corneal Refractive Therapy for Hyperopia. Optometry and Vision Science 84(4): 357-364.
-
Gifford P, Au V, Hon B, Siu A, Xu P, et al. (2009) Mechanism for corneal reshaping in hyperopic orthokeratology. Optom Vis Sci 86(4): e306-311.
-
Kirkwood BJ, Rees IH (2011) Central corneal iron line arising from hyperopic orthokeratology. Clin Exp Optom 94(4): 376379.
-
Carney LG (1975) The basis for corneal shape change during contact lens wear. Am J Optom Physiol Opt 52(7): 445-454.
-
Holladay JT (2015) Effect of corneal asphericity and spherical aberration on intraocular lens power calculations. Journal of Cataract & Refractive Surgery 41(7): 1553-1554.
-
Koffler BH, Sears JJ (2013) Myopia Control in children through refractive therapy gas permeable contact lenses: is it for real? Am J Ophthalmol 156(6): 1076-1081.e.1.
-
Chee EWL, Li L, Tan D (2007) Orthokeratology-related infectious keratitis: a case series. Eye Contact Lens 3(5): 261-263.
-
Van Meter WS, Musch DC, Jacobs DS, Kaufman SC, Reinhart WJ, et al. (2008) American Academy of Ophthalmology. Safety of overnight orthokeratology for myopia: a report by the American Academy of Ophthalmology. Ophthalmology 115(12): 2301-2301.
-
Choo JD, Holden BA, Papas EB, Willcox MDP (2009) Adhesion of Pseudomonas aeruginosa to orthokeratology and alignment lenses. Optom Vis Sci 86(2): 93-97.
-
Bullimore MA, Sinnott LT, Jones-Jordan LA (2013) The risk of microbial keratitis with overnight corneal reshaping lenses. Optom Vis Sci 90(9): 937-944.
-
Liu YM, Xie P (2016) The Safety of Orthokeratology--A Systematic Review. Eye Contact Lens 42(1): 35-42.
-
Singh K, Bhattacharyya M, Goel A, Arora R, Gotmare N, et al. (2020) Orthokeratology in Moderate Myopia: A Study of Predictability and Safety. J Ophthalmic Vis Res 15(2): 210-217.
-
Soni PS, Nguyen TT (2006) Overnight Orthokeratology Study Group. Overnight orthokeratology experience with XO material. Eye & Contact Lens: Science & Clinical Practice 32(1): 39-45.
-
Cheng HC, Liang JB, Lin WP, Wu R (2015) Effectiveness and safety of overnight orthokeratology with Boston XO2 high-permeability lens material: A 24 week follow- up study. Cont Lens Anterior Eye 39(1): 67-71.
-
Jun J, Zhiwen B, Feifu W, Lili L, Fan L (2018) Level of Compliance in Orthokeratology. Eye & Contact Lens: Science & Clinical Practice 44(5): 330-344.
-
Hiraoka T, Sekine Y, Okamoto F, Mihashi T, Oshika T (2018) Safety and efficacy following 10-years of overnight orthokeratology for myopia control. Ophthalmic Physiol Opt 38(3): 281-289.
-
Hiroka T, Matsumura S, Hori Y, Kamiya K, Miyata K, et al. (2024) Incidence of microbial keratitis associated with overnight orthokeratology: a multicentre collaborative study. Jpn J Ophthalmol.
-
Santodomingo-Rubido J, Cheung SW, Villa-Collar C (2024) The safety of orthokeratology contact lens wear in slowing the axial elongation of the eye in children. Cont. Lens Anterior Eye pp: 102258.
-
Santodomingo-Rubido J (2023) Orthokeratology for myopia control in everyday practice. Cont. Lens Anterior Eye 46(1): 101798.
-
Wang X, Li J, Zhang R, Li N, Pang Y, et al. (2019) The Influence of Overnight Orthokeratology on Ocular Surface and Meibomian Gland Dysfunction in Teenagers with Myopia. Journal of Ophthalmology 2019: 5142628.
-
Xie W, Zhang X, Xu Y, Yao YF (2018) Assessment of Tear Film and Bulbar Redness by Keratograph 5M in Paediatric Patients After Orthokeratology. Eye Contact Lens 55: S382-S386.
-
Xie C, Wei R (2023) Long-term changes in the ocular surface during orthokeratology lens wear and their correlations with ocular discomfort symptoms. Cont Lens Ant Eye 46(1): 101757.
-
Rah MJ, Barr JT, Bailey MD (2002) Corneal pigmentation in overnight orthokeratology: a case series. Optometry 73(7): 425-434.
-
Liang JYB, Chou PI, Wu R, Lee YM (2003) Corneal iron ring associated with orthokeratology. Journal of Cataract & Refractive Surgery (3): 624-626.
-
Huang PW, Yeung L, Sun CC, Chen HM, Peng SY, et al. (2020) Correlation of corneal pigmented arc with wide epithelial thickness map in orthokeratology- treated children using optical coherence tomography measurements. Cont Lens Anterior Eye 43(3): 238-243.
-
Keay L, Stapleton F (2008) Development and evaluation of evidence-based guidelines on contact lens-related microbial keratitis. Contact Lens and Anterior Eye 31(1): 3-12.
-
Stapleton F, Edwards K, Keay L, Naduvilath T, Dart JKG, et al. (2012) Risk factors for moderate and severe microbial keratitis in daily wear contact lens users. Ophthalmology 119(8): 1516-1521.
-
Leray B, Cassagne M, Soler V, Villegas EA, Triozon C, et al. (2015) Relationship between induced spherical aberration and depth of focus after hyperopic LASIK in presbyopic patients. Ophthalmology. 122(2): 233-243.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report