Profile of Ametropia in Children Aged 6 to 18 in HospitalEnvironments in Garoua
Introduction: Ametropia is one of the main ophthalmological pathologies in children. Uncorrected, they are the leading causeof visual impairment and blindness worldwide. The aim of this study was to describe the profile of ametropia in hospitalizedchildren.Methods: This was a retrospective, analytical study conducted in the ophthalmology department of the Garoua RegionalHospital (HRG) over a 04-year period from January 1,2020 to December 29, 2023. All children aged 6 to 18 diagnosed withametropia after an objective refraction study under cycloplegia were included. Epidemiological, clinical, and therapeuticvariables were studied. Analysis was performed using SPSS 20 software, with a significance level of p < 0.05.Results: Of the 11085 patients consulted during the study period, 5361 children (48.3%) were aged between 6 and 18, ofwhom 2863 (25.8%) had ametropia. The average age was 13.29±3.46 years, with the 16-18 age group the most representedin 33.3% of cases. The predominant sex was female (71%), with a sex ratio of 2.4. Headaches were the most frequent reasonfor consultation, accounting for 30.8% of cases. The most frequent types of ametropia were hypermetropic astigmatism,hyperopia, and myopic astigmatism in 44.1%, 28% and 15.1% respectively. Hyperopic astigmatism was more prevalent infemale children (in 65.0% of female children vs. 35.0% of male children p-value = 0.002). Twenty-five cases (16.7%) hadanisometropia.Conclusion: Ametropia is found in a quarter of children aged 6 to 18 in Garoua hospitals. Raising awareness with a view toearly consultation would enable early detection and treatment of ametropia.
Abbreviations
WHO: World Health Organization; ICD: International Classification of Diseases; OC: Optical Correction.
Introduction
Ametropia, or refractive errors, is one of the main pathologies diagnosed in children in ophthalmological consultations [1]. In ametropia, parallel light rays coming from infinity pass through, forming the image before or after the retina [2]. Left untreated, refractive errors can lead to amblyopia, which is characterized by low visual acuity that cannot be improved optically [3]. Ametropias are a major cause of ocular morbidity in children, with a detrimental impact on school performance [3].
The World Health Organization (WHO) estimates that some 153 million people worldwide have uncorrected or poorly corrected ametropia, with around 6.3 million living in Africa. Ametropia is the second leading cause of avoidable blindness after trachoma [4]. In sub- Saharan Africa, the prevalence of ametropia is 12.6% [5]. In Cameroon, a 2009 study of children aged 6 to 15 in Yaoundé showed an ametropia prevalence of 43.1%, with hyperopia accounting for 23.7% [6].
The distribution of refractive disorders seems to vary from one country to another, but we have no data on ametropia in children in northern Cameroon. We proposed to carry out a descriptive study at Garoua Regional Hospital on the profile of ametropia in children aged 6 to 18, to document the situation of this condition in our context.
Methodology
Our study was carried out in the ophthalmology department of the HRG. It was a retrospective, analytical study conducted over a 4-year period from January 1, 2020, to December 30, 2023. It was made up of all the records of patients aged between 6 and 18 who consulted a doctor during the study period and were diagnosed with ametropia. Patients aged 6 to 18 who were diagnosed with ametropia during the study period and had a complete file were included. Sampling was non-probability and exhaustive. The variables studied were sociodemographic characteristics (age, sex, school level, ethnicity, religion, place of residence, profession), clinical characteristics (medical history (notion of personal or family optical correction,) complaints, distance and near vision and type of ametropia). We selected the medical records of children aged between 6 and 18 years who had undergone:
- An AVL measurement for each eye using the SNELLEN/ ROSSANO E scale or MONOYER numbers and letters (1/10 corresponding to 0.1).
- Objective measurement of refraction with a TOPCON KR 8900 refractometer under cycloplegia (cyclopentolate (marketed as Skiacol® 0.5% or Cyclogyl® 0.5% or 1%)) 30 minutes after 4 instillations. A drop of sodium cyclopentolate (Skiacol) was instilled into each eye at time T0(s)-T5(m)-T10(s)-T15(m), then 30min later, the examination was performed using the RA RK 8400 POPCON at time T45.
- Only children who had undergone cycloplegic RA with normal SA and SP examination were included in the study.
- Patients with a spherical dioptric power ≤ -0.5D were considered myopic. Patients whose spherical dioptric power ≥ to +0.5D were said to be hyperopic. Astigmatic patients were those whose cylindrical dioptric power was either ≤ to -0.5D for myopic astigmatism or ≤ to +0.5D for hyperopic astigmatism or both and are termed mixed astigmatism. We used the International Classification of Diseases (ICD-11, 2018) to classify visual impairments [7].
Data were entered and analyzed in SPSS statistics 20. For categorical data we used the Chi-squared test and for continuous variables we used Pearson’s correlation. The significance level p<0.05.
Results
Epidemiological Aspects
A total of 11085 children were enrolled during the study period, and 2352 patients had ametropia, a frequency of 21.21%. The (16-18) age group was the most affected by ametropia, i.e. 33.6% (n=790). The average age was 13.29 ± 3.46, with extremes of 6 and 18 years (Figure 1).
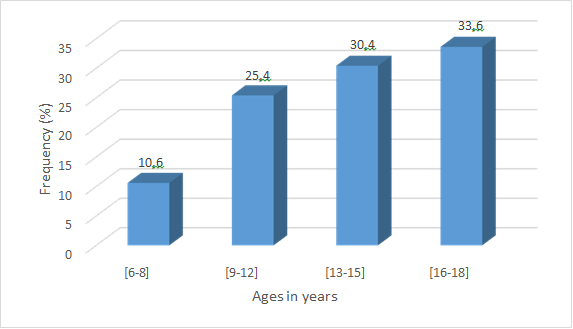
Figure 1: Age distribution of patients. Most cases were female (1671 or 71%), compared with 681 male cases (29%), giving a sex ratio of 2.4. In our study, 99.6% (n=2343) of children attended school, while 0.4% (n=9) were illiterate. Schoolchildren were predominantly represented in 94.5% (n=2223). Most patients (94.9% or 2231 cases) came from urban areas, while 121 cases (5.1%) came from rural areas.
Clinical Aspects
Headache was the main complaint in 1825 cases (30.8%), followed by watery eyes in 1195 children (20.1%). However, the same patient could complain of several functional signs. Speaking of history of optical correction (OC), 921 children (39.1%) had a history (personal and/or family) of OC, with 28.8% having a family history and 16.4% a personal history.
Among the files listed, 1755 patients had an AVL s/c ≥00.5 in the right eye and 1747 patients in the left eye, a frequency of 74.4% (3502 eyes in total), 14.4% (n=680 eyes) with an AV between [0.3-0.5], 7.2% (n=335) with an AV between [0.1-0.3] and 187 eyes had an AV˂ 0.05 i.e. a blindness frequency of 4% (n=187 eyes) (Table 1).
| AVL_Sc_OD | AVL_Sc_ | ||||
|---|---|---|---|---|---|
| Value | Number(n) | Percentage(%) | Number(n) | Percentage(%) | Total n(%) |
| ≥0,5 | 1755 | 74,6 | 1747 | 74,2 | 3502(74,4) |
| [0,3-0,5] | 340 | 14,4 | 340 | 14,4 | 680(14,4) |
| [0,1-0,3] | 170 | 7,2 | 165 | 7,2 | 335(7,2) |
| ˂0,05 | 87 | 3,8 | 100 | 4,2 | 187(4) |
| Total | 2352 | 100 | 2352 | 100 | 4704(100) |
Table 1: Distribution of eyes according to uncorrected AVL.
The most frequently diagnosed ametropia in our study was hyperopic astigmatism, accounting for 44.1% (2074 affected eyes in total). This was followed by hyperopia, which accounted for 28% (1315 affected eyes), 15.1% myopic astigmatism, 11.3% myopia and 1.5% mixed astigmatism (Table 2).
| OD | OG | ||||
|---|---|---|---|---|---|
| Ametropia | Number(n) | Percentage(%) | Number(n) | Percentage(%) | Total n(%) |
| Myopia | 265 | 11,3 | 265 | 11,3 | 530(11,3) |
| Hyperopia | 685 | 29,1 | 630 | 26,8 | 1315(28) |
| Astigmatism hyperopia | 972 | 41,3 | 1102 | 46,9 | 2074(44,1) |
| Myopic astigmatism | 390 | 16,6 | 320 | 13,6 | 710(15,1) |
| Mixed astigmatism | 40 | 1,5 | 40 | 1,5 | 80(1,5) |
Table 2: Summary of ametropia frequencies according to patients’ eyes.
After optical correction, the majority of patients in the study had an AVLAc ≥ of 0.5, i.e. 4,368 eyes (93%) with mild visual impairment, 99 patients or 276 eyes (5.8%) with low vision, and 30 patients with an AVLAc of less than 0.05, i.e. 60 eyes (1.4%) with blindness (Table 3).
| AVLAc OD | AVLAc OG | ||||
|---|---|---|---|---|---|
| Value | Number(n) | Percentage(%) | Number(n) | Percentage(%) | Total n(%) |
| ≥0,5 | 2188 | 93 | 2180 | 92,7 | 4368(93) |
| [0,3-0,5] | 97 | 4,1 | 101 | 4,2 | 198(3,9) |
| [0,1-0,3] | 38 | 1,6 | 40 | 1,7 | 78(1,7) |
| ˂ 0,05 | 29 | 1,3 | 31 | 1,4 | 60(1,4) |
| Total | 2352 | 100,0 | 2352 | 100,0 | 4704(100) |
Table 3: Distance visual acuity with correction.
Discussion
During our study, 11085 patients were seen in the ophthalmology department of the HRG, of whom 5361 children (48.3%) were aged between 6 and 18, all diagnoses combined, and of these only 2863 (25.8%) had ametropia. This result is higher than that found by Kalamba, et al. [3] in Congo in 2023, in their study: out of 6534 patients consulted,
1035 or 15.8% were aged 0 to 16 years, and among them 140 patients or 13.5% had ametropia. In the Ethiopia a review showed a 6% prevalence of ametropia responsible for visual impairment in children and adolescents [8]. In Nigeria, a prevalence of 33.3% was found in children aged 6 to 14 years [9]. In Somalia, the main cause of impairment of visual acuity was ametropia with a frequency of 76.8% [10].
The prevalence of ametropia varies considerably for the following reasons: variability in the study population regarding age, ethnic group, screening method, refractive error measurement method, sampling, and demographic distribution of populations.
Socio-demographic aspects
Age: The mean age in our study was 13.29 ± 3.46 with extremes of 6 and 18 years. The most represented age group was 16 to 18 in 33.6%. This result is comparable with those of Kalamba, et al. [3] who found that the most represented age group was 11-16 years in 81.49% and Eddrazi, et al. [11]: age range 9-14 years; mean age 8.8+/- 2.2 years (6-16 years). Eballé, et al. [12] in Cameroon in 2009 found an ametropia frequency of 43.1% of all pathologies in schoolchildren aged 6 to 15. This may be due to the fact that younger children do not express their visual impairment well, or to parental neglect, or because the expressiveness of the visual impairment increases with the level of schooling.
Gender: The ametropic children in our series were predominantly female (71%), with a sex ratio of 2.4. The same finding was found in most African studies: Gbé, et al. [13] (Côte d’Ivoire, 2014): 54.47%, Sounouvou, et al. [10] (Benin, 2008): 52.7%, Kalamba, et al. [3] (Congo, 2023): 65% and Eballé, et al. [12] (Cameroon, 2009): 60.7%.
In contrast, Edrrazi, et al. [11] in Morocco in 2013, found a male predominance (58%, sex ratio: 1.37). Sex does not determine the onset of ametropia.
Study Level: Most ametropic children aged 6 to 18 in our study attended school (94.5%). This result is identical to those of Eballé, et al. [12], who found that 100% of children attended school. This is due to the difference in methodology (study location).
Clinical Aspects
Reason for Consultation: The most frequent reason for consultation in our series was headache (30.8%). This result is comparable to those of Gbé, et al. [13] in Côte d’Ivoire, who found that headaches and BAV by far constituted 60.87% of the reasons for consultation. Similarly, Jeddi, et al. [14] reported in their series 82% headache and 41% distant AVB as the most frequent reasons for consultation. Kalamba, et al. [3] also reported AVB (42.1%) and headaches (25%).
Headaches and AVB are the most frequent and well-known symptoms that bring the general population to the doctor.
History: Regarding personal history of optical correction (OC), the majority did not wear glasses, only 386 children (16.4%) wore glasses, and those with family history of OC (22.7%). These results were similar to those of:
- Kalamba, et al. [3]: children wearing glasses: 37 (26%) and family CO: 29 (21%)
- Eddrazi, et al. [11] (Morocco, 2013): Personal CO: 15% and family CO: 38.3%.
This suggests that ametropia is hereditary and genetic. Neglect of children’s complaints by their parents, low socio- economic status and lack of information about refractive errors and their complications could be the causes that prevent or delay the treatment of ametropia.
Uncorrected Distance Visual Acuity: We found 1.3% of patients to be blind in the right eye and 1.4% in the left. This result is lower than that of Kalamba, et al. [3] who found that 12 patients (8.6%) were visually impaired in the right eye and 9 (6.4%) in the left.
According to the WHO, uncorrected ametropia is the second leading cause of avoidable blindness.
Corrected Distance Visual Acuity: After correction, more than half the patients had an AVL≥ 10/10é, i.e. 64.7% in the right eye and 63.9% in the left. Patients with an AVL of less than 3/10é after correction were negligible, i.e. 0.9%. These results are identical to those of Kalamba, et al. [3] although they used the classification according to visual impairment, after CO only one patient was visually impaired in both eyes. Wearing CO improves the AV of children with all types of ametropia, by reducing visual impairment.
Types of Ametropia Found
In Our Study, the Ametropias were Classified in Ascending Order as Follows:
- Myopia: 11.3% in the OD and the same in the OG
- Hyperopia: 29.1% OD and 26.8% OG
- Astigmatism: 59.6% OD and 61.9% OG. Astigmatism was therefore the most frequent ametropia of all types.
These results are similar to those of Eddrazi, et al. [11], who found that astigmatism was the most frequent refractive anomaly (46.7%), followed by hyperopia in 35% of cases and myopia in 18.3%.
On the other hand, Kalamba, et al. [3] found in their study: 24% for hyperopia, 29% for myopia and 47% for astigmatism. Astigmatism remains the most common ametropia.
Ametropia by Age and Gender: Myopia, hyperopic and mixed astigmatism were more common in the 16-18 age group, and hyperopia and myopic astigmatism in the 13- 15 age group. All types of ametropia were predominantly female. The prevalence of ametropias was statistically significant according to age and gender (p=0.0001). Gbé, et al. [13] found simple myopia only in children under 10 and simple hyperopia in children over 8. Kalamba, et al. [3] found that most of the ametropias were in the 11-16 age group, i.e. 81.42%. All this is due to differences in methodology.
Summary of Ametropia Types: In our study, hypermetropic astigmatism was the most common ametropia, with 41.3% OD and 46.9% OG. The same observation was made by Gbé, et al. [13], who showed that astigmatism was the most frequent refractive anomaly with 72.72%, especially in its compound form. On the other hand, Hashemi, et al. [15] in Morocco in 2004 noted a predominance of hyperopia at 56.6%. Lian Hong Pi, et al. [16] in China found a predominance of myopia in their series. Another study in China reveals prevalence of myopia of 63.1% [17]. Study in Iran found in children age 6 to 12, a prevalence of 11.6% for myopia and 6/7% for hyperopia with astigmatism being 28.9% especially in primary school children [18]. These differences in results are thought to be linked to ethnic and genetic factors. This is undoubtedly due to the variability of recruitment methods. Our study was retrospective in a hospital setting, whereas the other studies were prospective in a school setting.
Visual aids, are essential in the management of ametropia in children. Using optical glasses to correct ametropia are essential. In the case of partial, amblyopia or total blindness, they can use the study of bray, visual aids like pictograms, timer. Conclusion An overall frequency of 25.8% of ametropias was found, with a frequency of 21.21% of all cases included, underlining the importance of this condition.
The study population was predominantly female, with a sex ratio of 2.4 and an average age of 13.29, ranging from 6 to 18 years. Adolescents aged between 16 and 18 were the most represented, and schoolchildren represented the most affected school level of the study population, which would have influenced the prevalence and management of ametropia. The most frequent reasons for consultation were headaches and watery eyes. Hypermetropic astigmatism was the most common ametropia, followed by hypermetropia and myopic astigmatism. The limitations of the study were conducted in a single hospital in the city of Garoua. The study was retrospective and limited to symptomatic ametropias. Future prospects would be to extend the study to the general population of Garoua, include even non- symptomatic ametropias and pediatricians.
Conflict of Interest
We have no conflict of interest. References
1. Ayed T, Sakkah M, Chargi O, El Matril (2002) Epidemiology of refractive errors in socioeconomically disadvantaged schoolchildren in Tunisia. J Fr Ophtalmol 25(7): 72-77.
2. Zanlonghi X (2022) Visual impairment and blindness: how to serve our patients. Éditions Med-Line, Paris.
3. Kalamba DM, Muyombi KE, Makonga NA, et al. (2023) Epidemioclinical profile of ocular refractive errors in urban-rural and low-income children in Kamina. Int J Current Res 15(1): 23406-23409.
4. Kleinstein RN, Mutti DO, Sinnott LT, Jones-Jordan LA, Cotter SA, et al. (2021) Uncorrected refractive error and distance visual acuity in children aged 6 to 14 years. Optom Vis Sci 98(1): 3-12.
5. Atlaw D, Shiferaw Z, Sahiledengele B, Degno S, Mamo A, et al. (2022) Prevalence of visual impairment due to refractive error among children and adolescents in Ethiopia: a systematic review and meta-analysis. PLoS One 17(8).
6. Prema N (2011) Prevalence of refractive error in school children. Indian J Sci Technol 4(9): 1160-1161.
7. Bui Quoc E, Gomez A, Roth A, Amar R, Colliot JP, et al. (2022) Refractions: From diagnosis to optical and surgical treatments. Paris: Elsevier Masson.
8. Atlaw D, Shiferaw Z, Sahiledengele B, Degno S, Mamo A, et al. (2022) Prevalence of visual impairment due to refractive error among children and adolescents in Ethiopia: a systematic review and meta-analysis. PLoS One 17(8).
9. Ezegwui IR, Oguego NC, Okoye OI, Maduka-Okafor FC, Udeh N, et al. (2021) Prevalence of refractive errors and visual impairment in school children in Enugu South- East Nigeria. Niger J Clin Pract 24(3): 380-386.
10. Ahmed ZA, Alrasheed SH, Alghamdi W (2020) Prevalence of refractive error and visual impairment among school- age children of Hargesia, Somaliland, Somalia. East Mediterr Health J 26(11): 1362-1370.
11. Eddrazi H, Kriet M, Oubaaz A (2013) Epidemiology of refractive disorders in children. Medicine and Pharmacy, Marrakech.
12. Eballé AO, Bella AL, Owono D, Mbome S, Mvogo CE (2009) Eye pathology in children aged 6 to 15 years: hospital study in Yaoundé. Cahiers de Santé 19(2): 61-66.
13. Gbé K, Kouassi L, Coulibaly F, Boni S, Ouattara A, et al. (2014) Refractive errors in children in a private consultation in Abidjan: about 635 cases. Revue Soao 1: 40-43.
14. Jeddi Blouza A, Loukil I, Mhenni A, Khayati N, Malhouche N, et al. (2007) Management of hyperopia in children. J Fr Ophtalmol 30(3): 255-259.
15. Hashemi H, Fotouhi A, Mohammad K (2004) The age and gender specific prevalence of refractive errors in Tehran: the Tehran Eye Study. Ophthalmic Epidemiol 11: 213- 215.
16. Pi L, Linchen, Ke N, Fang J, Zhang S, et al. (2012) Prevalence of eye diseases and causes of visual impairment in school-aged children in western China. J Epidemiol 22(1): 37-44.
17. Wang J, Ying GS, Fu X, Zhang R, Meng J, et al. (2020) Prevalence of myopia and vision impairment in school students in Eastern China. BMC Ophthalmol 20(1).
18. Tajbakhsh Z, Talebnejad MR, Khalili MR, Masoumpour MS, Mahdaviazad H, et al. (2022) The prevalence of refractive error in schoolchildren. Clin Exp Optom 105(8): 860-864.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report