The Retinal Glide. A New Surgical Technique for the Myopic Traction Maculopathy Associated with Macular Retinal Detachment
A novel technique for the treatment of the traction myopic paculopathy is shown with previous review of the present techniques. In this unique approach after the ILM is peeled, the peripheral retina is detached and relaxed with a retinitomy. Therefore, the retina glides over the posterior staphyloma under heavy liquid to be definitely reattached. Also a case report of a 56 years old female patient with myopic traction maculopathy with lamellar macular hole and macular retinal detachment in her left eye is presented. The retina is reattached after the surgery with vision improvement observed at the third month with OCT image that confirm the macular hole closure.
Introduction
Degenerative myopia is an important cause of legal blindness in the world, being between the second and fourth cause depending on the country analyzed [1, 2, 3, 4, 5]. The elongation of the axial length and development of the posterior staphyloma in myops is closely related to the appearance of posterior pole complications that disrupt the patient's vision. These include choroidal neovascularization, chorioretinal atrophy and the so- called myopic traction maculopathy (MTM), including macular retinoschisis-like structure, macular hole and foveal retinal detachment [6, 7, 8, 9, 10, 11, 12].
The MTM is particularly occurs with an incidence of 67.7% in high myopic patients, increasing this rate with the age, which makes it relatively frequent in high myops in middle and advanced ages of life [9, 12, 13].
A Complex Etiologic Mechanism
Among the possible factors acting are the perpendicular tractions that axial elongation of the posterior staphyloma and the vitreous traction exert on the retina that has little capacity of distension. Associated to this phenomenon is also the tangential traction generated on the retina by the retinal vessels, the epimacular membranes and the internal limiting membrane. All this, aggravated with the atrophy of the choriocapillaris and the retinal pigment epithelium in the staphyloma (which decreases the ability of the retina to adhere in this area), results in a rigid retina that is unable to remodel itself to remain attached to the staphyloma.
Finally, this leads the formation of the so-called foveoschisis, the macular hole and the detachment of the myopic macular retina, which are only different stages of the same entity. The MTM syndrome [14, 15, 16].
A Difficult Condition to Treat
Taking into account this multifactorial etiologic mechanism, numerous techniques have been developed for the treatment of MTM, such as macular buckling and scleral shortening, among others [17, 18]. With these techniques, mainly macular buckling, retinal reattachment rates of up to 90% have been reported [19, 20]. However, the closure of the macular hole is seldom achieved because this technique does not acts on this factor, this is why poor vision is maintained even after a successful surgery and the risk of recurrent retinal detachment secondary to a persistent open macular hole is present.
For this reason, pars plana vitrectomy (PPV) with or without internal limiting membrane (ILM) peeling has been advocated as one of the most effective procedures to treat this condition. The idea behind this procedure is to relax the retina by acting on all the factors (except staphyloma) that cause traction on the retina with the formation of detachment and macular hole, thus allowing a better adaptation of the retina to the staphyloma. With this technique, anatomic success rates between 42 and 93% are reported, but again achieving the closure of the macular hole only between 10 and 73%, with the corresponding high rate of recurrence [21, 22, 23]. That is why there are authors who have not found significant improvements in the rates of reattachment and closure of the macular hole with this technique [24, 25, 26].
More recently Michalewska has described a variation of this technique: PPV with inversion of the ILM flap obtained and positioning it on the macular hole [27]. Theoretically this technique could increase the anatomical success rate of the macular hole related to retinal detachment, achieving a higher rate of macular hole closure [28, 29]. However, the final acuity remains low and the results are contradictory. This is possibly due to the fact that the inverted flap promotes the growth of glial tissue over the hole by plugging it (improving the rate of anatomical closure and retinal reattachment) but since this tissue is not from neural retina, the postoperative visual acuity does not have a significant difference with obtained with previous techniques. In a recently published meta-analysis showing the results of myopic patients treated with PPV with ILM peeling Alejandro Guerra GR and Gleydi PR. The Retinal Glide. A New Surgical Technique for the Myopic Traction Maculopathy Associated with Macular Retinal Detachment. J Ophthalmol 2019, 4(3): 000185.
compared with PPV, ILM peeling and inverted flap, this trend is very well demonstrated. The results are shown as follows. Retinal reattachment: 82 and 97.8% (P = 0.02). Anatomical closure of the macular hole: 28.5 and 93.5% (P = 0.02). Postoperative mean visual acuity (LogMar): 0.18 vs 0.42 respectively (P = 0.14) [30]. In summary, each technique used today is far from ideal, presenting some disadvantage. Could the creation of a new surgical technique improve the anatomical / visual results of myopic patients with MTM and posterior staphyloma?
Background
In 1979 Machemer described the therapeutic excision of the retina (retinotomy) as a safe procedure in the management of multiple diseases of the retina as used today [30].
Since 1993, Machemer and Steinhorst again used animal models to demonstrate the safety and reproducibility of the induction of therapeutic retinal detachments by subretinal infusion of fluid. The electron microscopy showed the preservation of the nuclei and mitochondrial material of the internal segments of the photoreceptors and low disruption of their external segments, suggesting that this technique was reasonably atraumatic and well tolerated. The Retinal Glide: The Thoughts behind the Process The creation of a peripheral retinotomy in the quadrants in relation to the posterior staphyloma during a PPV, with the aim of eliminate the acting tractive force, producing the rearrangement of the retina on the staphyloma, could act on almost all the factors known in the etiology of this condition. This proposed technique requires an induced retinal detachment in the area in which the retinotomy is planned, as this technique is developed for the patients with only macular detachment.
Eyes from high myops due to the continuous elongation of the axial diameter end up having a wide retinal periphery, with thinned and poorly vascularized retina. This situation makes the use of retinotomies in this area relatively safe. Here, the retina is easy to excise, there is considerable space for this manipulation in a retinal area of low participation in the visual process. In addition, low vascularity reduces bleeding possibilities.
Despite an exhaustive research in the national and international bibliography, we have not found the proposition or development of a similar technique.
Copyright© Alejandro Guerra GR and Gleydi PR.
Surgical Technique
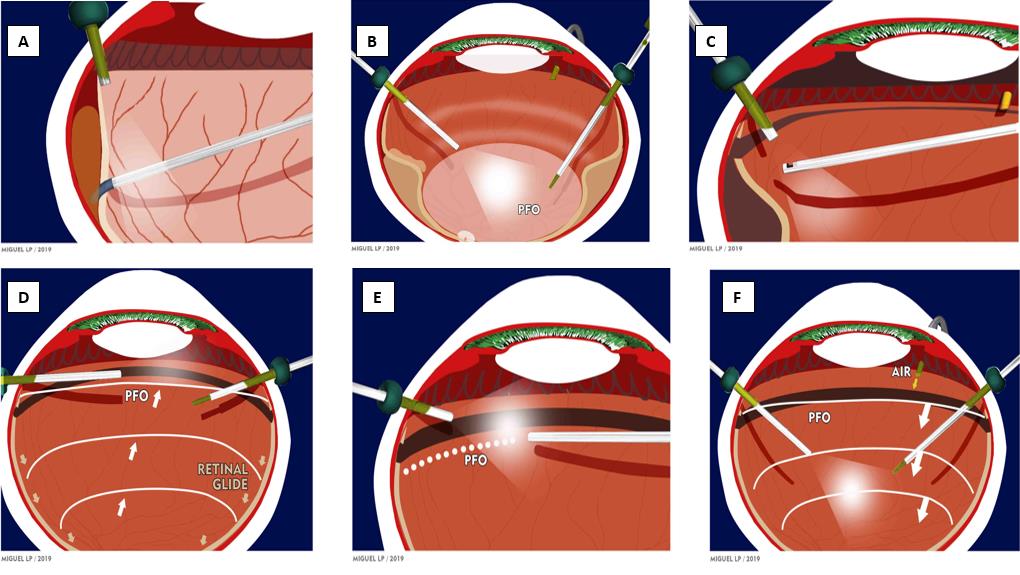
If lens is present, phacoemulsification with intraocular lens (IOL) implant is performed in the course of a PPV with 23 gauge instrumentation (R-Evolution, Optikon® 2000 S.p.A. Roma, Italy). A thorough shaving of the vitreous base is performed. Then an active detachment of the posterior hyaloid with triamcinolone aid and ILM peeling in the posterior pole using Brilliant Peel® (Fluoron, Geuder®. Heidelberg, Gemany) as a dye is carried out. In the periphery a localized retinal detachment is induced to the temporal quadrants, taking into account the staphyloma and macular detachment localization, using subretinal infusion microcannulas (Polytip®, Med One®. Sarasota, FL, USA), until both detachments are connected. A fluid-perfluoro octane (PFO) exchange is made, reaching the equatorial zone. In the temporal periphery, a circular retinotomy will be performed between 1000 and 1800 related with the detachment previously created. Once the posterior pole and the extreme peripheral retina is disconnected, the retina slides posteriorly and accommodates over the staphyloma by the action of the heavy liquid (retinal glide), thus leaving the retina rearranged on the macular area and free of all traction with the macular hole (if present) hopefully closed. Subsequently, a heavy liquid filling is performed up to the pars plana and the zone of the peripheral retinotomy is treated with photocoagulation. Finally, PFO/air/non-expansive C3F8 gas exchange is carried out (Figure 1).
Alternatively, prone and supine position is asked to the patient during the week following the surgery.
Case Report
A 56-year-old female patient with history of high myopia complained a two month lasting visual loss in her left eye. In examination, the right eye showed completely normal anterior segment with myopic fundus Alejandro Guerra GR and Gleydi PR. The Retinal Glide. A New Surgical Technique for the Myopic Traction Maculopathy Associated with Macular Retinal Detachment. J Ophthalmol 2019, 4(3): 000185.
and maculopathy. No peripheral degenerations. In the left eye, mild opacification of the lens was present. In the background, large posterior staphyloma with macular retinal detachment were spotted. No posterior or peripheral breaks were identified.
Copyright© Alejandro Guerra GR and Gleydi PR.
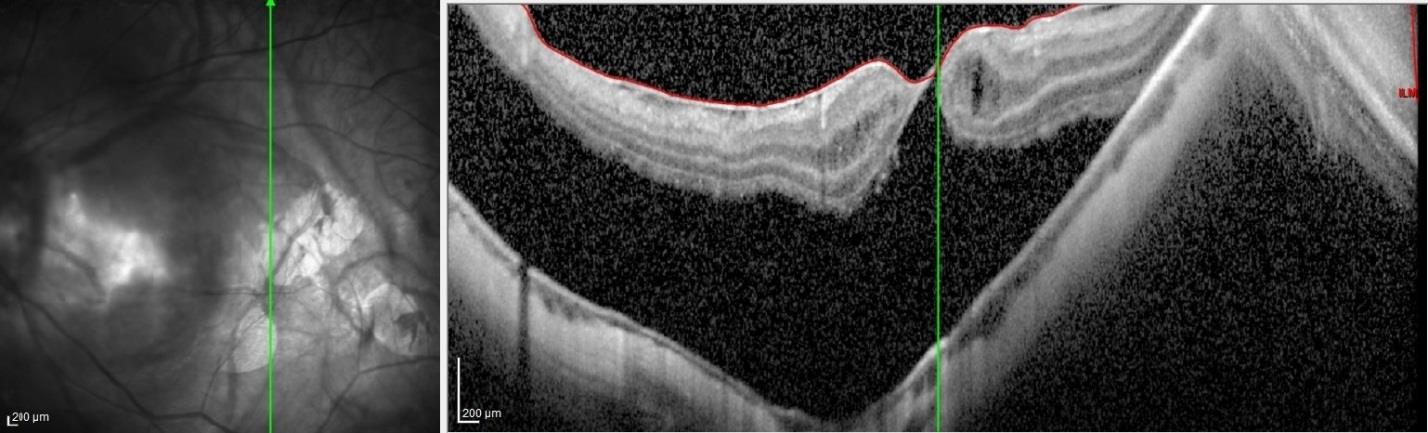
retinal detachment with myopic staphyloma and a still roofed macular hole with some cysts and epiretinal membrane in the left eye (Figure 2).
Considering the fact that we were facing a high myop with big posterior staphyloma, lamelar hole and macular detachment, we decided to perform a cataract extraction, leaving the patient aphakic (taking into account the result of the biometry and intra ocular lens calculation). Then, PPV was executed using 23 gauge instrumentation, performing the retinal glide technique and leaving C3F8 as tamponade.
After an uneventful phaco with PPV, the patient came to our office in day one of the post operatory for her left Alejandro Guerra GR and Gleydi PR. The Retinal Glide. A New Surgical Technique for the Myopic Traction Maculopathy Associated with Macular Retinal Detachment. J Ophthalmol 2019, 4(3): 000185.
eye with mild corneal edema and few cells in the anterior chamber. The capsular bag remained in place showing a posterior capsulotomy. The retina was reattached under C3F8.
At the third month after the surgery, the patient referred visual acuity improvement. The right eye was unchanged and in the left eye's anterior segment there was nothing remarkable to say. Retina was totally attached with good aspect at the retinotomy and posterior pole, however, staphyloma and the retinal pigment Copyright© Alejandro Guerra GR and Gleydi PR.
epithelium atrophy (myopic maculopathy) were present as described before. In addition, normal ocular tension levels were observed.
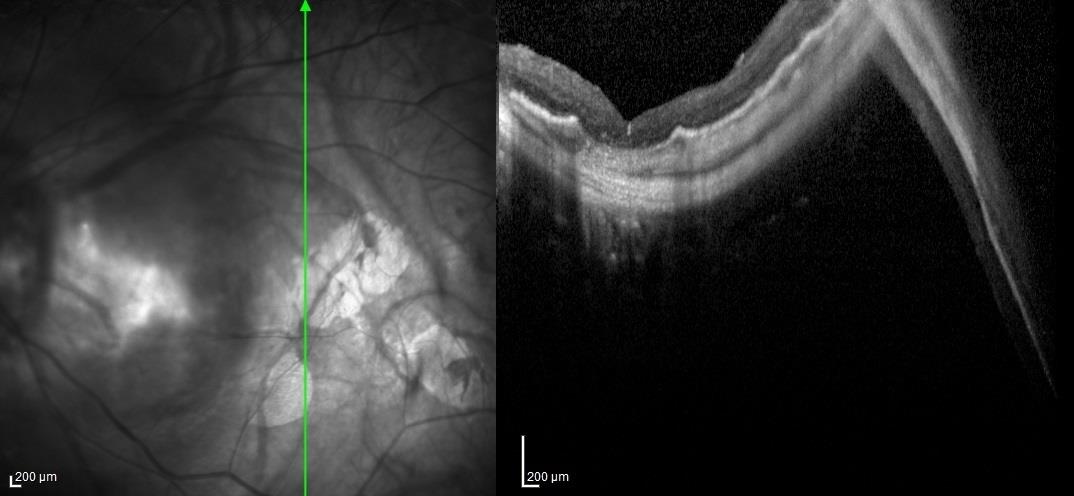
BCVA: OD -18.00 esf (20/30), OS -1.00 esf (20/100). OCT scan taken in the left eye at this visit showed the macula totally reattached with myopic staphyloma. A type II macular hole closure with alterations at the retinal pigment epithelium and the choriocapillaris were also visible (Figure 3). Right eye was unchanged.
Conclusion
Retinal glide seems to be an option to treat MTM when macular detachment is present. Further studies are needed to establish this technique as a possible gold standard treatment for this condition.
References
-
Iwase A, Araie M, Tomidokoro A, Yamamoto T, Shimizu H, et al. (2006) Tajimi Study Group. Prevalence and causes of low vision and blindness in a Japanese adult population: the Tajimi Study. Ophthalmol 113(8): 1354-1362.
-
Xu L, Wang Y, Li Y, Wang Y, Cui T, et al. (2006) Causes of blindness and visual impairment in urban and rural areas in Beijing: the Beijing Eye Study. Ophthalmology 113(7): 1134-1141.
-
Cedrone C, Culasso F, Cesareo M, Nucci C, Palma S, et al. (2003) Incidence of blindness and low vision in a sample population: the Priverno Eye Study, Italy. Ophthalmology 110(3): 584-588.
-
Buch H, Vinding T, La Cour M, Appleyard M, Jensen GB, et al. (2004) Prevalence and causes of visual impairment and blindness among 9980 Scandinavian adults: the Copenhagen City Eye Study. Ophthalmology 111(1): 53-61.
-
Klaver CC, Wolfs RC, Vingerling JR, Hofman A, de Jong PT (1998) Age-specific prevalence and causes of blindness and visual impairment in an older population: the Rotterdam Study. Arch Ophthalmol 116(5): 653-658.
-
Hayashi K, Ohno-Matsui K, Shimada N, Moriyama M, Kojima A, et al. (2010) Long-term pattern of progression of myopic maculopathy: a natural history study. Ophthalmology 117(8): 1595-1611. Alejandro Guerra GR and Gleydi PR. The Retinal Glide. A New Surgical Technique for the Myopic Traction Maculopathy Associated with Macular Retinal Detachment. J Ophthalmol 2019, 4(3): 000185.
-
Ohno-Matsui K, Kawasaki R, Jonas JB, Cheung CM, Saw SM, et al. (2015) International photographic classification and grading system for myopic maculopathy. Am J Ophthalmol 159(5): 877-883.
-
Ohno-Matsui, K Lai TY, Lai CC, Cheung CM (2016) Updates of pathologic myopia. Prog Retin Eye Res 52: 156-187.
-
Henaine-Berra A, Zand-Hadas IM, Fromow-Guerra J, García-Aguirre G (2013) Prevalence of macular anatomic abnormalities in high myopia. Ophthalmic Surg Lasers Imaging Retina 44(2): 140-144.
-
Hsiang HW, Ohno-Matsui K, Shimada N, Hayashi K, Moriyama M, et al. (2008) Clinical characteristics of posterior staphyloma in eyes with pathologic myopia. Am J Ophthalmol 146(1): 102-110.
-
Ikuno Y, Jo Y, Hamasaki T, Tano Y (2010) Ocular risk factors for choroidal neovascularization in pathologic myopia. Invest Ophthalmol Vis Sci 51(7): 3721-3725.
-
Oie Y, Ikuno Y, Tano Y (2005) Relation of posterior staphyloma in highly myopic eyes with macular hole and retinal detachment. Jpn J Ophthalmol 49(6): 530- 532.
-
Morita H, Ideta H, Ito K, Yonemoto J, Sasaki K, et al. (1991) Causative factors of retinal detachment in macular holes. Retina 11(3): 281-284.
-
Panozzo G, Mercanti A (2004) Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol 122(10): 1455-1460.
-
Ishida S, Yamazaki K, Shinoda K, Kawashima S, Oguchi Y (2000) Macular hole retinal detachment in highly myopic eyes: ultrastructure of surgically removed epiretinal membrane and clinicopathologic correlation. Retina 20(2): 176-183.
-
Kuhn F (2003) Internal limiting membrane removal for macular detachment in highly myopic eyes. Am J Ophthalmol 135(4): 547-549.
-
Feman SS, Hepler RS, Straatsma BR (1974) Rhegmatogenous retinal detachment due to macular hole. Management with cryotherapy and a Y-shaped sling. Arch Ophthalmol 91(5): 371-372.
-
Ando F, Ohba N, Touura K, Hirose H (2007) Anatomical and visual outcomes after episcleral Copyright© Alejandro Guerra GR and Gleydi PR. macular buckling compared with those after pars plana vitrectomy for retinal detachment caused by macular hole in highly myopic eyes. Retina 27(1): 37- 44.
-
Sasoh M, Yoshida S, Ito Y, Matsui K, Osawa S, et al. (2000) Macular buckling for retinal detachment due to macular hole in highly myopic eyes with posterior staphyloma. Retina 20(5): 445-449.
-
Sayanagi K, Ikuno Y, Tano Y (2006) Tractional internal limiting membrane detachment in highly myopic eyes. Am J Ophthalmol 142(5): 850-852.
-
Kadonosono K, Yazama F, Itoh N, Uchio E, Nakamura S, et al. (2001) Treatment of retinal detachment resulting from myopic macular hole with internal limiting membrane removal. Am J Ophthalmol 131(2): 203-207.
-
Oie Y, Emi K, Takaoka G, Ikeda T (2007) Effect of indocyanine green staining in peeling of internal limiting membrane for retinal detachment resulting from macular hole in myopic eyes. Ophthalmology 114(2): 303-306.
-
Lim LS, Tsai A, Wong D, Wong E, Yeo I, et al. (2014) Prognostic factor analysis of vitrectomy for retinal detachment associated with myopic macular holes. Ophthalmology 121(1): 305-310.
-
Li X, Wang W, Tang S, Zhao J (2009) Gas injection versus vitrectomy with gas for treating retinal detachment owing to macular hole in high myopes. Ophthalmology 116(6): 1182-1187. Alejandro Guerra GR and Gleydi PR. The Retinal Glide. A New Surgical Technique for the Myopic Traction Maculopathy Associated with Macular Retinal Detachment. J Ophthalmol 2019, 4(3): 000185.
-
Nakanishi H, Kuriyama S, Saito I, Okada M, Kita M, et al. (2008) Prognostic factor analysis in pars plana vitrectomy for retinal detachment attributable to macular hole in high myopia: a multicenter study. Am J Ophthalmol 146(2): 198-204.
-
Michalewska Z, Michalewski J, Adelman RA, Nawrocki J (2010) Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology 117(10): 2018-2025.
-
Kinoshita T, Onoda Y, Maeno T (2017) Long-term surgical outcomes of the inverted internal limiting membrane flap technique in highly myopic macular hole retinal detachment. Graefes Arch Clin Exp Ophthalmol 255(6): 1101-1106.
-
Michalewska Z, Michalewski J, Dulczewska-Cichecka K, Nawrocki J (2014) Inverted internal limiting membrane flap technique for surgical repair of myopicmacular holes. Retina 34(4): 664-669.
-
Machemer R (1979) Cutting of the retina: a means of therapy for retinalreattachment (author’s transl). Klin Monbl Augenheilkd 175(5): 597-601.
-
Machemer R, Steinhorst UH (1993) Retinal separation, retinotomy, and macular relocation: I Experimental studies in the rabbit eye. Graefes Arch Clin Exp Ophthalmol 231(11): 629-634. Copyright© Alejandro Guerra GR and Gleydi PR.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report