Conservative Treatment of Chylous Ascites after left Nephrectomy
Chylous ascites is the accumulation of chyle in the peritoneal cavity, a rare postoperative complication linked to a lesion of the abdominal or retroperitoneal lymphatic trunks. We report the case of a 68-year-old patient who underwent radical left total nephrectomy. Postoperative evolution was marked by chylous ascites, managed by conservative treatment with good evolution. This is a complication that should always be considered as a differential diagnosis of abdominal distension after radical nephrectomy.
Introduction
Chylous ascites is the accumulation of chyle in the peritoneal cavity, rare post-operative complication linked to a lesion of the abdominal or retroperitoneal lymphatic trunks [1]. Most cases of traumatic chylous ascites resolve with conservative treatment but refractory cases may require surgical ligation of the lymphatics [2].
Case Presentation
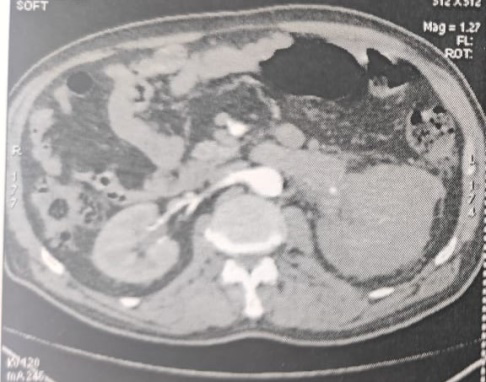
A 68 years old male, followed for benign prostatic hypertrophy on alpha-blocker for 3 years, chronic tobacco user, and hypertensive for 15 years on dual therapy, never operated. In his 6-month history, the patient had left low back pain with macroscopic total hematuria without fever or other associated signs. Clinical examination on admission found a conscious, apyretic patient at 37.1℃, left lumbar tenderness, on rectal examination he had a regular and flexible prostate of 80g. The pre-operative biological work-up was normal. The CT-Scann shows a left renal process of the medio and superior polar anterior lip of contrast-enhancing tissue density, measuring 81*43 mm, extending to the renal vein as well as the upper, middle calicial groups, the pyelon and the beginning of the ureter, including also the terminal portion of the renal artery (Figure 1).
The patient underwent a total left enlarged nephrectomy, the dissection of the renal vein being difficult ligated at its junction with the inferior vena cava (Figure 2).

The postoperative evolution was marked, on D2, by a redon drain of the renal compartment which brought back 1,500 of chylous fluid daily (Figure 3).
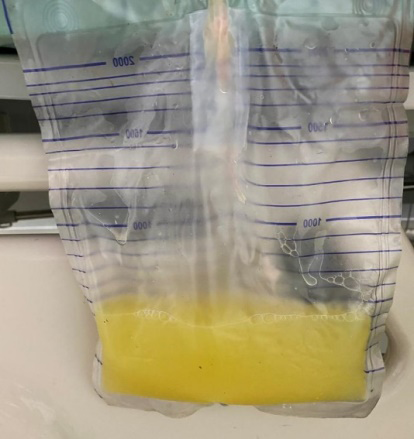
Biochemical analysis was consistent with the chyle. The patient was put on a low-salt, low-fat, high-protein diet, which resulted in a decrease in chylous production to about 1l/day, and was subsequently put on Sandostatin 100 µg three times a day. After 8 days of treatment the chyle decreased to 150 ml, and then at D12 we noticed a complete resolution of the chyle with an empty drain. The patient was discharged and advised to remain on a low-fat diet for 3 weeks.
Discussion
Although the main cause of postoperative chylous ascites is abdominal aortic surgery, transabdominal spinal, gynecological and urological procedures have also been described in case series and single case reports [3]. Chylous ascites can be classified as primary and secondary, the former being caused by a congenital dysfunction of the lymphatic system, while secondary chylous ascites can be caused by a malignant process, infection, trauma or post- surgical [1]. The incidence of postoperative chylous ascites is 1 to 17%, of which 0.6% are severe refractory cases for all surgeries combined [4]. In urology, it complicates 1.2-21% of retroperitoneal lymphadenectomies for testicular cancer and 3.8-5.1% of nephrectomies, particularly left nephrectomies (7.3%) [5]. Lymphatic drainage from the abdomen, pelvis and lower limbs goes to the paralumbar trunks which join the intestinal trunks to form the cisterna chyli. Thus, paraaortic renal artery dissection can result in injury to the paralumbar lymphatic trunks resulting in chylous leak and chylous ascites [6].
The clinical presentation of chylous ascites and chylous leakage differs according to whether there is a drain or not, with patients with a drain usually presenting with a persistent discharge of milky fluid, while those without a drain or with the drain removed presenting with abdominal distension, pain, nausea, or, more rarely, chylous discharge from the wound [7].
The diagnosis is made by CT scan or abdominal ultrasound. Chylous ascites is defined by a triglyceride level in the ascites fluid above 110 mg/dL. Typically this is 2 to 8 times higher than the plasma level [5].
Conservative treatment consists mainly of dietary modification (high protein, low fat, medium chain triglyceride diet), Somatostatin can be used to reduce intestinal fat absorption, thoracic duct triglyceride concentration and lymph flow. There is no exact timing for surgery, but some authors suggest that conservative management should be tried for 6 to 12 weeks before moving to surgical management [1, 5].
Conclusion
Chylous ascites should always be considered as a differential diagnosis of abdominal distension after radical nephrectomy. Conservative management should always be the first choice, and Sandostatin can play a vital role.
References
-
Alrabadi A, Ihmeidan M, Al Demour S (2021) Conservative management of chylous leak after open radical nephrectomy in an adult patient: a case report and literature review. Afr J Urol 27(1): 11.
-
Shah SS, Ahmed K, Smith R, Mallina R, Akhbari P, et al. (2008) Chylous ascites following radical nephrectomy: a case report. J Med Case Reports 2: 3.
-
Jairath A, Singh A, Ganpule A, Mishra S, Sabnis R, et al. (2015) Management Protocol for Chylous Ascites After Laparoscopic Nephrectomy. Urology 86(3): 521-528.
-
Hiffa A, Schulte K, Saeed M, Gani I (2022) Massive Chylous Ascites After Living Donor Nephrectomy Successfully Treated With Lymphatic Embolization. J Investig Med High Impact Case Rep 10: 23247096211065630.
-
Michel F, Lechevallier E, Boissier R (2019) Prise en charge de l’ascite chyleuse postopératoire. Prog En Urol – FMC 29(4): F95‑F97.
-
Meulen ST, van Donselaar-van der Pant KA, Bemelman FJ, Idu MM (2013) Chylous ascites after laparoscopic hand-assisted donor nephrectomy: Is it specific for the left-side. Urol Ann 5(1): 45‑46.
-
Kim BS, Yoo ES, Kim TH, Kwon TG (2010) Chylous ascites as a complication of laparoscopic nephrectomy. J Urol août 184(2): 570‑574.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report