Assessment of Ureteric Stone Composition Along with Medical Expulsive Treatment of Distal Unilateral Ureterolithiasis in Emergency Department
Background: Ureterolithiasis is among the foremost painful and prevalent among urologic disorders which will substantially impact health-related quality of life. The objective of this study is to provide a brief description regarding ureteric stone composition and treatment of ureterolithiasis. Method: The method of this study was chosen to be cross sectional prospective. The study was carried out in department of urology of Sialkot Medical Complex and Amina Hospital Sialkot cant. Sample size for this study was taken as 200 patients. Well-structured data collection form was prepared, analyzed and then filled by interviewing the patients. Result: The highest occurring stone type was calcium oxalate dihydrate stone (39.5%) and calcium oxalate monohydrate stone (33%). Tamsulosin (96%) was highest recommended for calculus expulsion therapy along with citro soda (90%), diclofenac sodium (76%) and omeprazole (62.5%).
Introduction
Ureteral stones disease is among the foremost painful and prevalent among urologic disorders particularly in patients with a history of recurrent stones [1]. Ureterolithiasis can be defined as the consequence of an alteration of the normal crystallization conditions of urine in the urinary tract specifically ureter [2]. Subjective stone related symptoms were defined as acute and chronic flank pain, dysuria, gross hematuria, anuria and urinary tract infection [3]. Often the etiology of a patient’s kidney stone is unknown. Unless a patient passes a stone, is able to retrieve the stone, and sends it for analysis, the components of the stone usually remain unknown [4]. Patients with distal ureteral stones but 10 mm in diameter are often treated with tamsulosin, a α1 -adrenergic antagonist usually used for benign prostatic hypertrophy, to assist stone passage [5].
Methodology
Study Design
A prospective cross-sectional study was carried out on the patients suffering from ureterolithiasis. Total number of ureterolithiasis patients participated in this study was 200. Study was carried out in Sialkot Medical Complex (SMC) and Amina Hospital Sialkot located in Sialkot, Pakistan.
Data Collection Procedure
The research was carried out in OPD of Sialkot Medical Complex and Amina Hospital Sialkot. A data collection form was designed for questioning about ureterolithiasis including; Do you feel urinary urgency frequently? Do you have oliguria? Do you have hypertension? Patients were asked about their diet plan including; how much you take milk, rich protein diet? Do you take fruit juices? Do you eat salad? The patient reports including renal function test and ultrasound were assessed. The parenchymal echogenicity, hydronephrosis, cyst or mass, wall thickness, focal lesions, the values of; urea, creatinine, uric acid, sodium, calcium, potassium etc. were also documented.
Inclusion Criteria
- Patients who signed the consent form and were interested in research work were included.
- Patients diagnosed with ureterolithiasis were included in this study
- Patients having cyst with Ureteral calculi were included.
- Patients of Sialkot premises were included.
Exclusion Criteria
- People with unethical believe were excluded.
- Patient without ureterolithiasis were excluded.
- Patients having cysts without ureteral calculi were excluded.
- Patients outside the premises of Sialkot were excluded.
Data Analysis
The data was analyzed and interpreted after collection. The graphs and tables were plotted on Microsoft word and Microsoft excels to analyze the prevalence and prescription trends for ureterolithiasis patients.
Results and Discussion
Prevalence of Multiple Types of Ureteric Stones
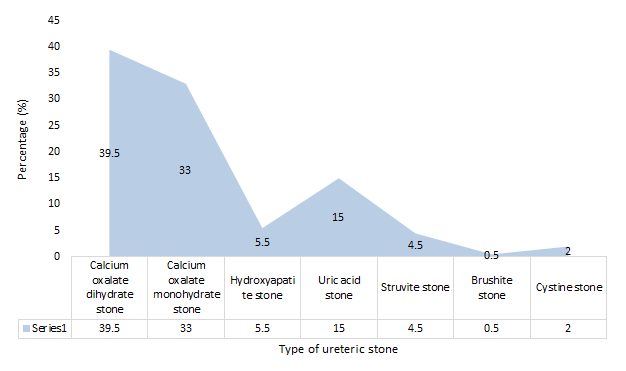
Out of the participants suffering from ureterolithiasis, the results showed predominance of calcium oxalate dihydrate (n=79, 39.5%). Other stones that were diagnosed were calcium oxalate monohydrate (n=66, 33%), uric acid stone (n=30, 15%), hydroxyapatite stone (n=11, 5.5%), struvite stone (n=9, 4.5%), cystine stone (n=4, 2%) and brushite stone (n=1, 0.5%). Figure showed predominance of participants for calcium oxalate dihydrate and monohydrate uric acid stone. This is also relatable to another study which showed that 80% of stones that were diagnosed in ureterolithisis were composed of calcium oxalates [6]. Another study showed that majority of the ureter stones are calcium oxalate and are the result of metabolic and environmental factors [7] Table 1 & Figure 1.
| Frequency | Percentage (%) | |
|---|---|---|
| Calcium oxalate dihydrate stone | 79 | 39.5 |
| Calcium oxalate monohydrate stone | 66 | 33 |
| Hydroxyapatite stone | 11 | 5.5 |
| Uric acid stone | 30 | 15 |
| Struvite stone | 9 | 4.5 |
| Brushite stone | 1 | 0.5 |
| Cystine stone | 4 | 2 |
Table 1: Prevalence of multiple types of ureteric stones (N=200).
Assessment of Treatment Trends of Ureterolithiasis
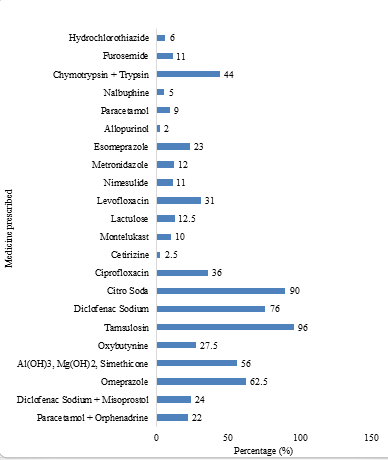
Medicines mostly prescribed in Sialkot for treatment of ureterolithiasis from sample of 200 patients were tamsulosin (n=192, 96%), citrosoda (n=180, 90%), diclofenac sodium (n=152, 76%), omeprazole(n=125, 62.5%), simeticone + aluminium hydroxide + magnesium hydroxide (n=112, 56%), trypsin + chymotrypsin (n=88, 11%), ciprofloxacin (n=72, 36%), levofloxacin (n=62, 31%), oxybutynin (n=55, 27.5%), diclofenac sodium + misoprostol (n=48, 24%), paracetamol + orphenadrine (n=44, 22%), lactulose (n=25, 12.5%), furosemide (n=22, 11%), nimesulide (n=22, 11%), montelukast (n=20, 10%), paracetamol (n=18, 9%), hydrochlorothiazide (n=12, 6%), nelbuphine (n=10, 5%), cetirizine (n=5, 2.5%) and allopurinol (n=4, 2%). Figure 4.6 showed tamsulosin was highly recommended for ureter stones as it is believed that it is used for medical expulsive therapy and benign prostatic hyperplasia (BPH). It also helps with the passage of ureter stones. Tamsulosin appears to be effective only for stones over 4 mm and less than 10 mm in size. Results of this study are relatable to the study that showed use of tamsulosin as a spasmolytic drug during renal colic due to juxtavesical calculi increased the stone expulsion rate and decrease expulsion time [8]. Another study also concluded that showed alpha-blockers inhibit basal smooth muscle tone and hyper-peristaltic uncoordinated frequency and likelihood of spontaneous passage of ureteric stone as they lower ureteric muscle stone [9, 10, 11, 12, 13, 14, 15, 16] Table 2 & Figure 2.
| Generic drugs | Frequency | Percentage (%) |
|---|---|---|
| Paracetamol + Orphenadrine | 44 | 22 |
| Diclofenac Sodium + Misoprostol | 48 | 24 |
| Omeprazole | 125 | 62.5 |
| Al(OH)3, Mg(OH)2, Simethicone | 112 | 56 |
| Oxybutynine | 55 | 27.5 |
| Tamsulosin | 192 | 96 |
| Diclofenac Sodium | 152 | 76 |
| Citro Soda | 180 | 90 |
| Ciprofloxacin | 72 | 36 |
| Cetirizine | 5 | 2.5 |
| Montelukast | 20 | 10 |
| Lactulose | 25 | 12.5 |
| Levofloxacin | 62 | 31 |
| Nimesulide | 22 | 11 |
| Metronidazole | 24 | 12 |
| Esomeprazole | 46 | 23 |
| Allopurinol | 4 | 2 |
| Paracetamol | 18 | 9 |
| Nalbuphine | 10 | 5 |
| Chymotrypsin + Trypsin | 88 | 44 |
| Furosemide | 22 | 11 |
| Hydrochlorothiazide | 12 | 6 |
Table 2: Prevalence of medicine prescribed in ureterolithiasis (N=200).
Conclusion
Majority of ureteric calculi were composed of calcium oxalate dehydrate and calcium oxalate monohydrate. Tamsulosin was much more prescribed medicine of treatment of ureteric calculi.
Authors’ Contributions
Faiza Naeem proposed the idea of this project and designed the study. Muhammad hammad-Ur-Rehman and Azizullah Mukhtar performed the survey for data collection. Saqlain Khalid and Muhammad Jawad Khalid compiled the data. Faiza Naeem supervised and analyzed the data. All authors equally contributed, wrote the manuscript and coordinated the project preparation of the final version of the manuscript.
Acknowledgment
The study was conducted by the Islam College of Pharmacy, Sialkot.
References
-
Rabah DM, AlOmar M, Binsaleh S, Arafa MA (2011) Health related quality of life in ureteral stone patients: post-ureterolithiasis. Urological research 39(5): 385- 388.
-
Grases F, Costa-Bauza A, Prieto RM (2006) Renal lithiasis and nutrition. Nutrition journa 5(1): 1-7.
-
Wimpissinger F, Türk C, Kheyfets O, Stackl W (2007) The silence of the stones: asymptomatic ureteral calculi. The Journal of urology 178(4): 1341-1344.
-
Glazer K, Brea IJ, Vaitla P (2021) Ureterolithiasis. StatPearls Publishing; Treasure, Island.
-
Goldfarb DS (2009) Nephrolithiasis. Annals of internal medicine 151(3): ITC2-ITC1.
-
Hughes P (2007) Kidney stones epidemiology. Nephrology 12(1): S26.
-
Wang W, Fan J, Huang G, Li J, Zhu X, et al. (2017) Prevalence of kidney stones in mainland China: A systematic review. Scientific reports 7: 41630.
-
Hirvonen T, Pietinen P, Virtanen M, Albanes D, Virtamo J (1999) Nutrient intake and use of beverages and the risk of kidney stones among male smokers. American Journal of epidemiology 150(2): 187-194.
-
Ljunghall S, Hedstrand H (1975) Epidemiology of renal stones in a middle‐aged male population. Acta Medica Scandinavica 197(1‐6): 439-445.
-
Hoe Kim H, Jo MK, Kwak C, Park SK, Yoo KY, et al. (2002) Prevalence and epidemiologic characteristics of urolithiasis in Seoul, Korea. Urology 59(4): 517-521.
-
Worcester EM, Coe FL (2010) Clinical practice Calcium kidney stones. New England Journal of Medicine 363(10): 954-963.
-
Sowers MR, Jannausch M, Wood C, Pope SK, Lachance LL (1998) Prevalence of renal stones in a population-based study with dietary calcium, oxalate, and medication exposures. American journal of epidemiology 147(10): 914-920.
-
Nicoletta JA, Lande MB (2006) Medical evaluation and treatment of urolithiasis. Pediatric Clinics 53(3): 479- 491.
-
Passerotti C, Chow JS, Silva A, Schoettler CL, Rosoklija I (2009) Ultrasound versus computerized tomography for evaluating urolithiasis. The Journal of urology 182(4S): 1829-1834.
-
Dellabella M, Milanese G, Muzzonigro G (2003) Efficacy of tamsulosin in the medical management of juxtavesical ureteral stones. The Journal of urology 170(6 Pt 1): 2202-2205.
-
Aldaqadossi HA, Shaker H, Saifelnasr M, Gaber M (2015) Efficacy and safety of tamsulosin as a medical expulsive therapy for stones in children. Arab journal of urology 13(2): 107-111.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report