Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
Introduction: We report a rare case of facial metastasis from a gastrointestinal stromal tumor (GIST). Case report: A 70-year-old patient was admitted to the ENT-HN department of CNHU-HKM in 2018 for a recurring tumor on the right side of his face. His medical history includes right mandible surgery in 2015 and 2017. The pathological examination of the second surgical specimen identified a schwannoma. Postoperatively, a mass appeared at the expense of the parotid gland. A total parotidectomy in 2018 confirmed the same histological type. Two months later, the evolution was marked by the appearance of subcutaneous nodules in line with the surgical scar and in the parotid lodge. The pathological examination, complemented by immunohistochemistry of the extracted nodules in 2019, revealed metastatic lesions with an intestinal origin. The patient was put on Imatinib 100 (GLIVEC® 100) and experienced an improvement in his clinical condition, followed by a gradual deterioration. The search for the primary focus isolated a rectal tumor with neighboring metastatic foci. The patient passed away in 2021. Conclusion: Mandibular and parotid metastases from a gastrointestinal stromal tumor (GIST) are rare. Immunohistochemistry, complementary to pathology, is necessary. Survival is better appreciated when the diagnosis is early, and treatment is based on targeted therapies.
Lawson Afouda S¹*, Avakoudjo F², Adjadohoun S³, Médji S¹, Takin R⁴, Gnangnon F⁵, Baglo T⁶ and Adjibabi W¹
Abbreviations
Introduction
Craniofacial metastases from colorectal cancers are poorly documented due to their rarity [1]. Mandible metastases generally arise from the development of GIST adenocarcinoma.
The incidence of GIST is 10 to 15 cases per million population worldwide, with approximately 5,000 cases per year in the United States [2]. However, they remain the most common sarcomas in humans [3]. They derive from Cajal cells with dual muscle and nerve contingency and preferentially develop from the stomach or small intestine in 60% and 25% of cases respectively [4]. But the GIST can also originate in the esophagus, colon, rectum and duodenum in ascending order [4]. It is a soft tissue sarcoma that expresses the oncogene KIT(CD117) and is characterized by a frequency of activating mutations of the “Kinase Inhibitor Thyrosin” (KIT) genes or the alpha-type platelet-derived growth factor receptor alpaha (PDGFRA) found in 85% of cases [5]. The gastrointestinal stromal tumor (GIST) is often asymptomatic in the early phase and signs appear when it develops. The GIST can be benign or malignant and, in this case, it has a local destructive potential but, it can also develop away from the abdomen; we talk about metastatic GIST.
The areas of dissemination, although rare, are the lungs and bones. At the stage of metastasis, a drug treatment is admitted which is long-term by the use of targeted therapies including Thyrosine Kinase inhibitors. We report a case of rare metastatic localization of a GIST discovered by immunohistochemistry.
Case Report
Mr. Syl. A., a 70-year-old retired warehouse worker from the oil mills of Benin, was received in November 2018 in the ENT-CCF department of CNHU-HKM for the surgical management of a recurrent tumor of the right half of the face. He has a history of two surgeries performed outside of Benin; in 2015, for an unspecified right mandibular tumor and in 2017, an interruptive surgery of the right hemi mandible with reconstruction by a screwed plate (Figure 1 and 2).
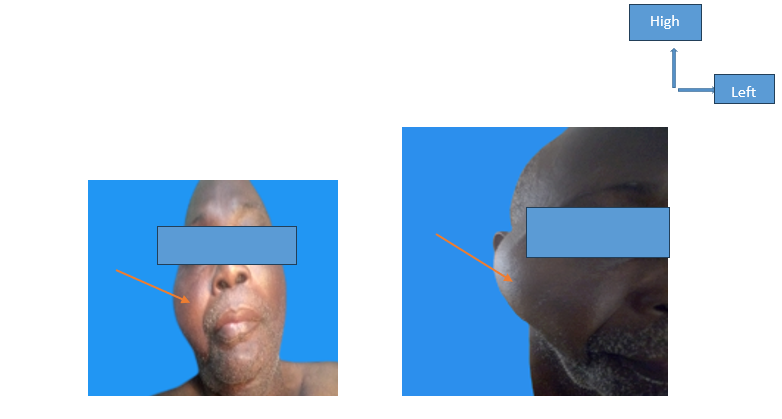
Figure 1(a) Figure 1(b) Figure 1: Tumoral mass deforming the right half of the face.
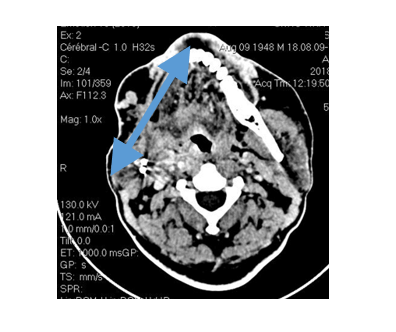
Right anterior hemi-mandibulectomy Sequelae performing a bone amputation Figure 2: Computed tomography of the facial mass (axial section).
The Surgical Specimen Consisted of a Schwannoma on Pathological Examination. The patient returned to Benin with a satisfactory general condition. It was in 2018, ie, 1 year later, that he came to consult in our center for a non-painful right parotid mass that appeared in a context of weight loss and lack of appetite, prompting a CT scan of the facial mass (Figure 3).
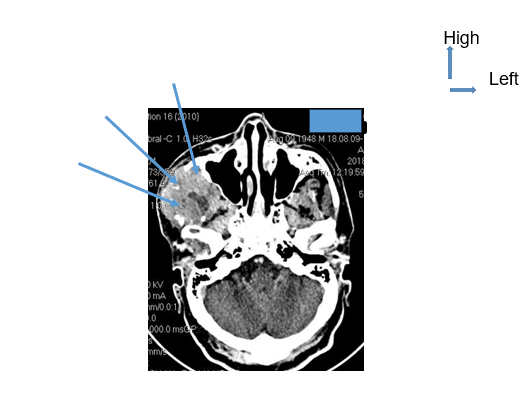
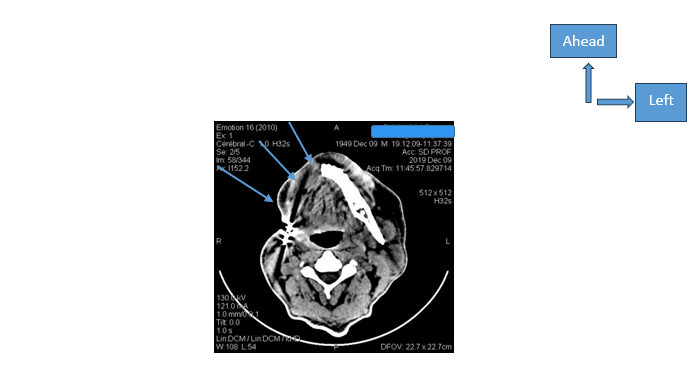
Tissue-like tumoral mass developed at the expense of the right masticatory muscles. Figure 3: Computed tomography of the facial mass (axial section).
This suggests a tumoral process of the right half of the face by objectifying a hyperdense tissue aspect with hypodense areas, calcifications, and lymphadenopathies of sectors I and II on the right. He underwent a total parotidectomy with preservation of the facial nerve at the end 2018 (Figure 4).
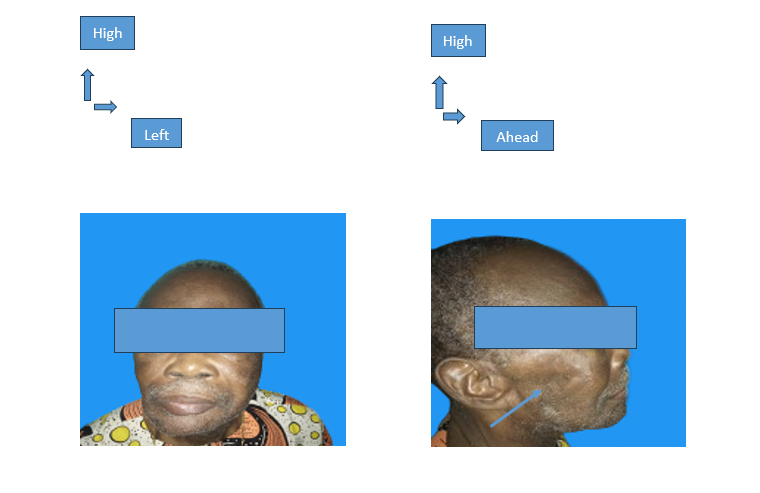
Figure 4(a): Face Figure 4(b): Profile Figure 4: Result at 6 months post-operatively of a tumor mass with sequelae of excavation lesion on the right side on the profile image.
The pathological examination found a parotid schwannoma without signs of malignancy. The evolution was marked nine (09) months later by the occurrence of multiple nodules on the right half of the face located in the buccal mucosa and the buccal commissure, in the temporal and digastric muscles. The patient benefited from nodulectomies 2019. Intraoperatively, the nodules were adherent-based and had a serpiginous extension difficult to dissect, making us suspect a malignant process. A second pathological examination complemented by immunohistochemistry of the nodules in the same laboratory revealed metastases from a gastrointestinal stromal tumor (GIST).
The search for the primary site requires the performance of additional examinations. The esophago-gastro duodenal endoscopy was normal. The abdomino-vesico-prostatic ultrasound allowed to appreciate hepatic lesions considered secondary to a digestive neoplasia; similarly, the multinodular prostate had a suspicious appearance. A thoraco-abdomino- pelvic CT scan was performed with the aim of confirming and better understanding the extension of the suspected lesions. The existence of a subpleural micronodule on the left, the presence of emphysematous bullae in the right upper lobe, heterogeneous hypodense lesions of the liver, axial and peripheral lyses of vertebrae T8, T10 to T12, L2-L3. Moreover, the CT scan assessment of the rectosigmoid wall suggested a malignant tumor. A colonoscopy with biopsy of the rectal mucosa associated with a pathological examination for the confirmation of this diagnosis could not be performed due to lack of financial means. We concluded the diagnosis of malignant gastrointestinal stromal tumor (GIST), starting from the rectum extended to the pelvis, the thoraco-lumbar spine with pulmonary and mandibular metastases. The patient was put on Imatinib tab 400 mg/day (GLIVEC ®). The treatment started with a preserved general condition, a weight of 55kg (height=1.67m), at the Blood Count (NFS) a Hb rate = 9.9 g/L, leukocytes at 8500 per liter with 19% blasts. Regular follow-up in the hematology and ENT-CCF departments of the same hospital center was observed. The evolution was marked 7 months after the start of treatment by a better clinical state with a weight gain (67Kg) and an instability of the leukocyte formula; at the 10th month, a good clinical evolution and a normal NFS were noted. At the 14th month, a deterioration of the general state set in with fatigue and a weight loss to 58 Kg (Figure 5).
16 months postoperative of the tumoral Mass. No local recurrence Figure 5: Computed tomography of the facial mass (axial section).
Clinical signs of hemolysis could be noted with sub-icteric bulbar mucous membranes, conjunctival anemia, “Coca-Cola” urine; digestive disorders made of vomiting and constipation existed but went unnoticed. The patient died at home in 15 months after the start of drug treatment in a picture of renal function disturbance (uremia=0.39, creatinine=21mg/L) and hepatic function (ASAT=65, ALAT=40).
Discussion
Xu in China reported a male predominance with a mean age of 50.2 years; emphasizing that after age 50 the risk of sarcoma occurrence is 2.63 times higher [6]. In the present observation, the symptomatology would have started at the age of 65 and was confirmed at 70.
Gastrointestinal stromal tumors (GISTs) are little symptomatic, or they manifest themselves by common signs that do not attract attention. Initially, the patient will present general signs such as asthenia and weight loss; they can be put down to a lack of appetite. The latter is accompanied by digestive signs in occurrence of nausea and vomiting or even constipation. These signs will last over time and gradually increase without orienting towards a GIST. The patient in this observation was followed outside our center and has already been operated on twice for a tumor of the mandible; it is indeed the persistence of signs and the reappearance of facial swelling that motivated his return home. This facial localization of the GIST does not a priori suggest a secondary localization. This diagnosis was suspected in our center in front of a second tumor recurrence. The schwannoma reported as an anatomopathological result after the second and then the third surgical intervention was discordant with the patient’s clinical condition more worrying than the manifestation of a benign tumor. GISTs have long been confused with Leiomyoma and schwannoma. In this medical observation, it is immunohistochemistry associated with the anatomopathological examination that concluded a GIST with cutaneous, mandibular and vertebral bone, hepatic and prostatic metastases. Immunohistochemistry is therefore necessary. It allows to isolate the specific antibodies of the proteins KIT and DOG found in 90% or even 95% of cases [7, 8, 9].
For about fifteen years and in developed countries, targeted therapies have a preponderant place in the treatment of solid cancers as in hemopathies. Their use in our country started in 2002 thanks to a program to promote and make accessible these new therapies still expensive for our developing countries. In this context, Imatinib 100 mg (GLIVEC®), at a rate of 400 mg per day was administered in 1st line in this study. According to the recommendations of the FNCLCC 2006 reference [10], this therapy is indicated in case of non-respectable tumor or for metastatic tumors. This patient was operated on a total of 4 times, because in progressive pursuit with bone and pulmonary metastases.
In these cases, and according to the recommendations of the FNCLCC 2006, there are other protocols than those of the 1st line. They are not available in our country, these are the 2nd line molecules such as Sunitinib (SUTENT®) and those of the 3rd line, Regorafenib (STIVARGA®). According to the recommendations of ESMO 2022 and NCCN 2023, the same consensus has been validated regarding the first-line medical treatment of GIST metastases and second-line in the event of resistance [11, 12]. As for surgery, it should be reserved for local complications such as gastrointestinal perforations, not found in this case study [10]. On the other hand, it was performed on cutaneous, parotid and mandibular metastatic lesions for diagnostic purposes and to overcome the aesthetic problem related to the facial deformation presented. The 2-year survival under targeted therapies is 45 to 75%. The patient died at home 15 months after the start of first-line targeted therapies.
Conflict of Interest: The authors stated that there is no conflict of interest.
Funding Statement: The authors received no specific funding for this work.
Conclusion
Metastatic Gastrointestinal Stromal Tumor (GIST) is rare. A source of diagnostic wandering, it can manifest itself with banal digestive symptoms with a secondary tumor location to different organs and distant from the initial site. Recurrence after complete surgical tumor excision should prompt the performance of a complementary immunohistochemical examination to pathology. The medical treatment of GIST is based on targeted therapies. The 2-year survival was appreciable in this medical observation in the patient who presented a GIST with a cutaneous, parotid and mandibular facial metastasis.
References
-
Samlali H, Bouchbika Z, Bennani Z, Taleb A, Benchekroune N et al. (2017) Cranial metastasis of rectal adenocarcinoma: a case report with literature review. Pan Afr Med J 26: 58.
-
Khan J, Ullah AA, Waheed A, Karki NR, Adhikari N and al. (2022) Gastrointestinal Stromal Tumors (GIST): A Population-Based Study Using the SEER Database, including Management and Recent Advances in Targeted Therapy. Cancers 14(15): 3689.
-
Gbessi G, Gnangnon F, Seidou F, Adanzounnon M, Chigblo S et al. (2020) Epidemiological and histopathological aspects of sarcomas in Cotonou (Benin) from 2010 to 2020. Med Trop Sante Int 2(1).
-
Kim Y, Lee SH (2024) Pathologic diagnosis and molecular features of gastrointestinal stromal tumors: a mini- review. Front Oncol 14: 148-467.
-
Vallilas C, Sarantis P, Kyriazoglou A, Koustas E, Theocharis S et al. (2021) Gastrointestinal Stromal Tumors (GISTs): Novel Therapeutic Strategies with Immunotherapy and Small Molecules. International Journal of Molecular Sciences 22(2): 493.
-
Xu L, Ma Y, Shengfeng W, Feng J, Liu L and al. (2021) Incidence of gastrointestinal stromal tumor in Chinese urban population: A national population-based study. Cancer Medicine 10(2): 737-744.
-
Ibrahim A, Chopra S (2020) Succinate Dehydrogenase– Deficient Gastrointestinal Stromal Tumors. Arch Pathol Lab Med 144 (5): 655-660.
-
Venkataraman V, George S, Cote G (2023) Molecular Advances in the Treatment of Advanced Gastrointestinal Stromal Tumor. The Oncologist 28(8):671-681.
-
Ammoura I, Montgomery E (2024) Gastrointestinal Stromal Tumors: Variants and Some Pitfalls That They Create. Advances In Anatomic Pathology 31(6): 354-363.
-
Casali PG, Blay JY (2010) Consensus Panel of Experts Gastrointestinal stromal tumors: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 21 (Suppl 5): v98-102.
-
Casali PG, Blay JY, Abecassis N, Bajpai J, Bauer S et al. (2022) Gastrointestinal stromal tumors: ESMO- EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology 33(1): 20-33.
-
Von Mehren M, Kane III JM, Riedel RF, Sicklick JK, Pollack SM. (2022) Gastrointestinal Stromal Tumors. Official Journal of National Comprehensive Cancer Network 20(11): 1204-1214.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?
- Allergic Rhinitis in Senegal: Epidemiological, Clinical and Therapeutic Aspects