4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
Objective: To describe the clinical presentation, diagnostic challenges, and surgical management of a rare fourth branchial sinus anomaly in a two-year-old child presenting with recurrent thyroid abscess. Methods: A 2-year-old child presented with fever and anterior neck swelling. Imaging revealed recurrent left-sided thyroid abscess. Incision and drainage were performed twice. Further evaluation with direct laryngoscopy and MRI suggested a fourth branchial cleft sinus anomaly. Definitive management consisted of left hemithyroidectomy with excision of the sinus tract and electrocauterization of the pyriform fossa opening. Results: The child had an uneventful recovery, with resolution of symptoms and no recurrence at 1 year follow-up. Histopathology confirmed a branchial sinus tract coursing through the thyroid lobe. Conclusion: Fourth branchial cleft sinus anomalies are rare congenital defects that should be considered in children with recurrent thyroid abscesses. A combination of imaging and endoscopic evaluation facilitates diagnosis. Definitive surgical excision with closure of the pyriform sinus opening prevents recurrence.
Bhatt H¹*, Kurup B¹, Periera C¹, Prabhat D¹, Joshi R², Gala F³, Karkera P⁴ and Naik P¹
Introduction
Fourth branchial anomalies characteristically present in close association with the thyroid gland, with a tract ascending to the pyriform sinus [1]. Clinical presentation includes recurrent anterior neck abscesses, thyroiditis and thyroid abscess. Diagnosis is based on imaging and direct laryngoscopy. Management options include endoscopic approaches, open transcervical approaches and a combination of both.
Clinical Presentation
A 2-year-old child presented with recurrent left-sided thyroid abscesses associated with fever, neck swelling, leukocytosis, elevated erythrocyte sedimentation rate, and elevated C-reactive protein, with normal thyroid function tests. The child underwent incision and drainage at ages 1 year 8 months and 2 years 6 months.
Diagnostic Workup
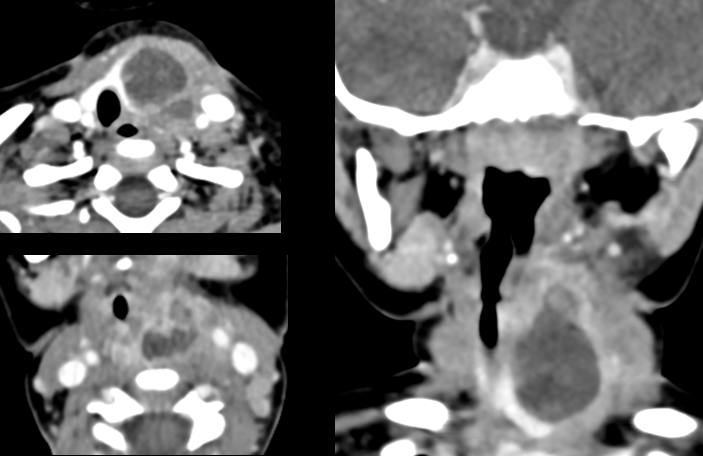
Initial diagnostic workup included an Ultrasonography and CECT of the neck that demonstrated a left thyroid abscess extending toward the pyriform sinus (Figure 1).
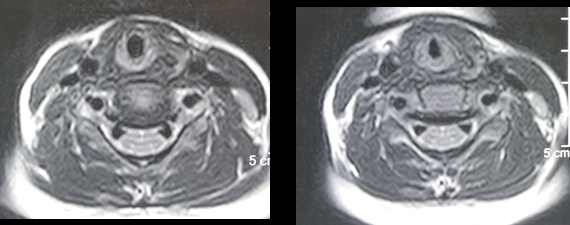
MRI done post the resolution of acute inflammation showed a small T2 hyperintense focal signal in the upper pole of the left thyroid lobe with a suspicious tract extending superiorly to the posterior pharyngeal wall (Figure 2).
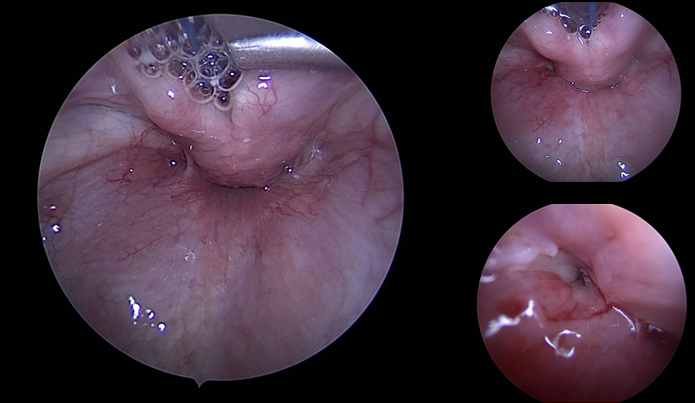
Direct laryngoscopy revealed an opening in the left pyriform fossa, raising suspicion of a fourth branchial cleft sinus anomaly (Figure 3).
Surgical Management
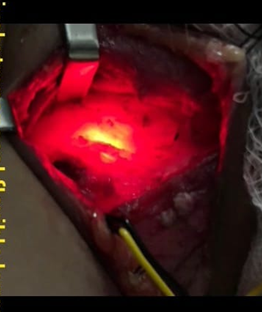
A left hemithyroidectomy was performed with excision of the sinus tract. Electrocauterization of the sinus opening in the left pyriform fossa was done. Intraoperative neuromonitoring was used to preserve the recurrent laryngeal nerve. Identification of the sinus tract near the superior pole of the thyroid was confirmed by transillumination using a flexible fiberoptic scope placed in the pyriform fossa. The specimen was excised and sent for histopathological evaluation (Figure 4).
Outcome
Postoperative recovery was uneventful. The child remained symptom-free with no recurrence at 1 year follow- up. Histopathology confirmed the presence of a sinus tract traversing the thyroid lobe, consistent with a fourth branchial sinus anomaly (Figure 5).

Discussion
Branchial cleft anomalies occur in 1 of 3 forms: cysts, sinuses, or fistulae. Cysts are epithelial-lined structures that do not have external openings that connect to the skin or pharynx. Sinus tracts connect either the skin or the pharynx to a blind pouch. Sinus tracts communicate either externally with skin as a visible punctum or internally with the pharynx or larynx, where the punctum opening will only be visible on endoscopy. Branchial cleft fistulae are true communications connecting the pharynx or larynx with the external skin [2]. Second branchial cleft anomalies are most common accounting for up to 90% of branchial anomalies with the remaining 10% are 1st, 3rd, 4th branchial anomalies of which fourth branchial anomalies are rarest [3].
A fourth branchial arch anomaly most commonly presents as a sinus tract that courses from the apex of the pyriform fossa to the upper lobe of the left thyroid. Fourth branchial arch anomalies are remnants of an embryological tract which arises from the pyriform sinus. The tract descends from the pyriform fossa along the tracheoesophageal groove, posterior to the internal and common carotid arteries [4]. Fourth branchial cleft fistula presents as recurrent neck abscesses, thyroiditis and thyroid abscess.
Diagnostic tests usually combine imaging tests and direct laryngoscopy. Direct laryngoscopy can be performed during an acute infection and if a sinus tract is identified it confirms the diagnosis. Direct laryngoscopy aids in identification of the sinus tract during neck exploration by insertion of various probes, catheters contrast fluids or by transillumination of the tract. Definitive treatment with cauterization of opening of the sinus tract can be done [5].
Although the sinus or fistula tract cannot be seen easily on imaging, the combination of an infected neck cyst with adjacent thyroid inflammation and inflammation of tissues along the expected tract is pathognomonic [1]. In patients presenting with acute suppurative thyroiditis or neck infection with thyroid gland involvement, the presence of T2 high signal behind the cricothyroid joint on MRI is highly suggestive of the diagnosis of congenital pyriform sinus fistula [6]. Contrast swallow studies can be useful after acute inflammation has subsided as contrast can pool in the pyriform fossa sinus and proximal tract. Barium swallow examination may however, fail to demonstrate the sinus tract, even after the Valsalva maneuver because they require a quiescence of inflammation of the tract for the entry of the barium contrast into the sinus [7]. Ingested contrast with CT can also aid the surgeon in complete removal by delineating the tract and its relationship to surrounding structures in the setting of prior infection and surgical manipulation [8].
Management options include complete surgical excision, a combined treatment involving external surgery with internal cauterization of the mucosal communication to eradicate the disease process [9], or solely endoscopic approaches.
Endoscopic options include electrocauterization of sinus opening, coblation treatment of the sinus opening [10], obliteration of the opening using fibrin glue [11], trichloroacetic acid cauterization [12].
These solely endoscopic approaches via direct laryngoscopy allow for management of the underlying pathology and at the same time reduce the risks associated with transcervical, open approaches. However, the endoscopic approaches do not address any persistent abnormality within the thyroid gland and may not fully treat the source if residual abnormality persists [13].
Hemithyroidectomy as well as partial resection of the ipsilateral posterior thyroid ala should be considered as usually as there is a history of suppurative thyroiditis or the tract is noted to run through the thyroid itself [1]. In the series reported by Sihag A, et al. [14] hemithyroidectomy was combined with complete sinus tract excision in only 36% of cases where the sinus tract was very closely adhered to the left thyroid lobe due to repeated suppurative thyroiditis in past. Hemithyroidectomy may not always be necessary if the sinus tract can be adequately exposed to thyroid lobe without damaging the recurrent laryngeal nerve. In the series by Arunachalam P, et al. [9], all the patients underwent combined electrocauterization of the internal opening with neck exploration and excision of anomalous tract. Cannulation of the tract under direct visualization with a small catheter aided complete and safe dissection. In one of their cases, the fibrous tract involved the thyroid lobe and hemithyroidectomy was done. As per Nicoucar K, et al. [5] complete excision of the entire fistula tract during a quiescent period, together with a partial thyroidectomy, appears to be the treatment of choice. However, they suggest that open surgery should be reserved for patients older than age 8 years to minimize complications. In children less than 8 years, they recommend medical management with endoscopic cauterization as an effective alternative strategy.
In our case we combined electrocauterization of the pyriform sinus opening, with hemithyroidectomy and excision of the tract. Intraoperative neuromonitoring and use of transillumination of tract through pyriform fossa using flexible fiberoptic scope aided in avoiding the complication of recurrent laryngeal nerve injury and aided complete excision with no recurrence at 1 year follow up. Histopathology demonstrated the tract coursing through the thyroid gland.
Conclusion
Fourth branchial arch anomalies should be suspected in children with recurrent anterior neck abscesses and thyroid abscesses. Imaging and direct laryngoscopy are used for diagnosis. A sinus opening in the pyriform fossa identified on direct laryngoscopy confirms the diagnosis. Management includes cauterization of the sinus opening and transcervical excision of the tract, with ipsilateral hemithyroidectomy. Intraoperative neuromonitoring and fiberoptic transillumination can be useful to prevent complications and recurrence.
References
-
Doody J, Sobin L (2017) Fourth branchial pouch or cleft anomalies. Oper Tech Otolayngol Head Neck Surg 28 (3): 167-72.
-
Holt AC, Lofgren DH, Shermetaro C (2025) Branchial Cleft Anomalies. StatPearls Publishing, USA.
-
Koeller KK, Alamo L, Adair CF, Smirniotopoulos JG (1999) From the Archives of the AFIP: Congenital cystic masses of the neck: Radiologic-pathologic correlation. Radiographics 19 (1): 121-146.
-
Adnan SH, Nobecourt P, Tran S, Radhakrishnan RS, Bowen-Jallow KA (2019) Fourth branchial cleft cyst and congenital absence of the contralateral thyroid lobe. J Pediatr Surg Case Rep 47: 101245.
-
Nicoucar K, Giger R, Pope HG Jr, Jaecklin T, Dulguerov P (2009) Management of congenital fourth branchial arch anomalies: a review and analysis of published cases. J Pediatr Surg 44 (7): 1432-1439.
-
Han Z, Tai J, Gao J, Wang S, Yu T, et al. (2021) MRI in Children With Pyriform Sinus Fistula. J Magn Reson Imaging JMRI 53 (1): 85-95.
-
Pal I, Kumar S, Mukherjee A, Mondal B, Babu AS (2018) Fourth branchial pouch sinus: A report of 7 cases and review of the literature. Ear Nose Throat J 97 (8): 236- 242.
-
Stone ME, Link DT, Egelhoff JC, Myer CM (2000) A new role for computed tomography in the diagnosis and treatment of pyriform sinus fistula. Am J Otolaryngol 21 (5): 323-325.
-
Arunachalam P, Vaidyanathan V, Sengottan P (2015) Open and Endoscopic Management of Fourth Branchial Pouch Sinus - Our Experience. Int Arch Otorhinolaryngol 19 (4): 309-313.
-
Chen W, Chen J, Chen F, Wu J, Zhao L, et al. (2021) Endoscopic coblation treatment for congenital pyriform sinus fistula in children. Medicine, US, 100 (19): e25942.
-
Cigliano B, Cipolletta L, Baltogiannis N, Esposito C, Settimi A (2004) Endoscopic fibrin sealing of congenital pyriform sinus fistula. Surg Endosc 18 (3): 554-556.
-
Stenquist M, Juhlin C, Åström G, Friberg U (2003) Fourth Branchial Pouch Sinus with Recurrent Deep Cervical Abscesses Successfully Treated with Trichloroacetic Acid Cauterization. Acta Otolaryngol, Sweden 123 (7): 879-882.
-
Orobello NC, Insalaco LF, Roby BB (2020) Fourth branchial cleft sinus with foreign material within thyroid gland. Int J Pediatr Otorhinolaryngol 132: 109948.
-
Sihag A, Sundararajan L, Thirunavukkarasu S (2025) Third and Fourth Branchial Arch Anomalies in Children: Insights from a Tertiary Care Center. J Indian Assoc Pediatr Surg 30 (3): 296-301.
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?
- Allergic Rhinitis in Senegal: Epidemiological, Clinical and Therapeutic Aspects