Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
Background: Ear, Nose, and Throat (ENT) disorders are a frequent reason for consultation in district hospitals in low-resource settings. The performance of referral and counter-referral systems is a key determinant of continuity and quality of care. This study aimed to describe the organization and functionality of the ENT referral system in district hospitals of N’Djamena and to identify professional factors associated with referral practices. Methods: A cross-sectional analytical study was conducted from April to July 2023 among 157 non-specialist practitioners working in four district hospitals. Data were collected using a structured questionnaire. Associations were assessed using the Chi-square test and estimated by odds ratios (OR) with 95% confidence intervals (95% CI). Results: Referral was practiced by 52.9% of participants (n = 83/157). The main reasons for referral were lack of diagnostic resources (94.0%, n = 78/83) and perceived insufficient expertise (84.3%, n = 70/83). Counter-referral feedback was absent in 77.1% of cases (n = 64/83). Professional experience ≤10 years (OR = 9.60; 95% CI: 4.37–21.07) and practical ENT training (OR = 8.54; 95% CI: 2.44–29.91) were significantly associated with referral practice. Conclusion: The ENT referral system appears partially functional but marked by weak informational continuity. Strengthening formal counter-referral mechanisms and professional training represents a key organizational priority.
Abbreviations
ENT: Ear, Nose, and Throat; OR: Odds Ratio; CI: Confidence Interval; 95% CI: 95% Confidence Interval; WHO: World Health Organization; SPSS: Statistical Package for the Social Sciences.
Introduction
Ear, Nose, and Throat (ENT) disorders represent a frequent reason for consultation in primary and secondary healthcare facilities, particularly in low- and middle- income countries [1, 2, 3]. Although often perceived as benign conditions, these disorders may progress to preventable complications in the absence of appropriate management, leading to significant morbidity and impairment of quality of life [2, 3].
The quality of ENT care does not rely solely on individual clinical skills or the availability of diagnostic resources. It also depends on the organization of the referral and counter- referral system, which plays a central role in ensuring continuity and coordination of care [4, 5]. An appropriate referral enables access to specialized expertise when local capacities are exceeded, whereas counter-referral ensures feedback and follow-up at the peripheral level, thereby contributing to improved professional practice [5].
In many resource-limited settings, referral systems remain insufficiently structured. The World Health Organization (WHO) emphasizes that weaknesses in referral mechanisms result in diagnostic delays, overburdening of tertiary facilities, and fragmentation of care pathways [6]. In sub-Saharan Africa, referral circuits are often informal, and counter-referral mechanisms remain poorly functional [7, 8].
In the field of ENT, these challenges are further amplified by the scarcity of specialists and their concentration in university hospital centers [9]. District hospitals therefore play a strategic role in patient orientation. However, professional determinants that may influence referral practices—such as years of experience or specific ENT training—remain poorly documented in this context.
In Chad, district hospitals constitute the second level of the national healthcare system and manage a substantial proportion of ENT consultations. Nevertheless, data describing the organization and functionality of referral and counter-referral mechanisms in this setting remain limited.
The objective of this study was to describe the organization and functionality of the ENT referral and counter-referral system in district hospitals of N’Djamena and to identify sociodemographic and professional factors associated with referral practices.
Materials and Methods
Study Design
This was a cross-sectional analytical study conducted to describe the organization and functionality of the referral and counter-referral system for ENT disorders and to identify factors associated with referral practices among healthcare practitioners.
Study Setting
The study was carried out in four district hospitals in N’Djamena, Chad, representing the second level of the national healthcare system:
- Sultan Cherif Kasser District Hospital
- Union District Hospital
- Farcha Peace Hospital
- Gozator District Hospital These facilities provide secondary-level healthcare services and serve as key referral points for patients requiring higher-level management. At the time of the study, none of the included hospitals had a dedicated ENT department or a full-time ENT specialist. Data collection was conducted from April to July 2023.
Study Population
The study population consisted of non-specialist healthcare practitioners involved in the management of ENT conditions within the selected district hospitals.
Inclusion Criteria
- Non-specialist practitioners practicing in the selected hospitals
- Involvement in the management of patients with ENT disorders
- Present during the study period
- Provided informed consent
Exclusion Criteria
- ENT specialists
- Practitioners not involved in ENT patient management
- Refusal to participate A total of 157 practitioners were included using an exhaustive sampling approach.
Data Collection
Data were collected using a structured, pretested questionnaire administered through face-to-face interviews.
The questionnaire included sections on:
- Sociodemographic characteristics
- Professional qualification
- Years of professional experience
- Practical ENT training
- Referral practice (yes/no)
- Referral destinations
- Criteria guiding referral decisions
- Counter-referral practices
Variables
Dependent Variable
- Referral practice for ENT patients (yes/no) Independent Variables
- Sex
- Age group
- Professional qualification
- Place of practice
- Years of professional experience
- Practical ENT training For analytical purposes, years of professional experience were categorized into two groups: ≤10 years and >10 years.
Statistical Analysis
Descriptive analysis was performed using frequencies and percentages for categorical variables. Associations between referral practice and independent variables were assessed using the Chi-square test. The strength of association was estimated using odds ratios (OR) with 95% confidence intervals (95% CI). A p-value < 0.05 was considered statistically significant. Data were coded and analyzed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Ethical Consideration
The study was conducted in accordance with the principles of the Declaration of Helsinki and received approval from the relevant institutional ethics committee prior to data collection. Participation was voluntary. Written informed consent was obtained from all participants, and collected data were anonymized and handled with strict confidentiality.
Results
Sociodemographic and Professional Characteristics of Practitioners
A total of 157 non-specialist practitioners were included in the study.
Women accounted for 59.9% of participants (n = 94), whereas men represented 40.1% (n = 63). The most represented age group was 31–35 years, comprising 36.9% of practitioners (n = 58).
In terms of professional qualification, state-certified nurses constituted the largest group (53.5%, n = 84), followed by midwives (17.8%, n = 28) and general practitioners (16.6%, n = 26).
Regarding professional experience, 36.9% of practitioners (n = 58) reported having 6–10 years of experience. Only 15.9% of participants (n = 25) had received practical ENT training, whereas 84.1% (n = 132) had not received any specific training in ENT.
The detailed distribution of practitioners according to their characteristics and referral practice is presented in Table 1.
| Characteristics | Total n (%) | Referral Yes n (%) | Referral No n (%) |
|---|---|---|---|
| Sex | |||
| Male | 63 (40.1) | 35 (55.6) | 28 (44.4) |
| Female | 94 (59.9) | 48 (51.1) | 46 (48.9) |
| Age Group (years) | |||
| 25 – 30 | 26 (16.6) | 14 (53.8) | 12 (46.2) |
| 31 – 35 | 58 (36.9) | 31 (53.4) | 27 (46.6) |
| 36 – 40 | 34 (21.7) | 19 (55.9) | 15 (44.1) |
| 41 – 45 | 30 (19.1) | 15 (50.0) | 15 (50.0) |
| 46 – 50 | 7 (4.5) | 4 (57.1) | 3 (42.9) |
| 51 – 55 | 2 (1.3) | 0 (0.0) | 2 (100) |
| Professional Qualification | |||
| State-certified nurse | 84 (53.5) | 45 (53.6) | 39 (46.4) |
| Midwife | 28 (17.8) | 14 (50.0) | 14 (50.0) |
| General practitioner | 26 (16.6) | 18 (69.2) | 8 (30.8) |
| Senior health technician | 19 (12.1) | 6 (31.6) | 13 (68.4) |
| Place of Practice | |||
| Sultan Cherif Kasser Hospital | 37 (23.6) | 23 (62.2) | 14 (37.8) |
| Union Hospital | 41 (26.1) | 25 (61.0) | 16 (39.0) |
| Farcha Peace Hospital | 43 (27.4) | 18 (41.9) | 25 (58.1) |
| Gozator Hospital | 36 (22.9) | 17 (47.2) | 19 (52.8) |
| Years of Professional Experience | |||
| 0 – 5 | 44 (28.0) | 32 (72.7) | 12 (27.3) |
| 6 – 10 | 58 (36.9) | 40 (69.0) | 18 (31.0) |
| 11 – 15 | 35 (22.3) | 8 (22.9) | 27 (77.1) |
| 16 – 20 | 17 (10.8) | 3 (17.6) | 14 (82.4) |
| 21 – 25 | 3 (1.9) | 0 (0.0) | 3 (100) |
| Practical ENT Training | |||
| Yes | 25 (15.9) | 22 (88.0) | 3 (12.0) |
| No | 132 (84.1) | 61 (46.2) | 71 (53.8) |
Table 1: Association Between Sociodemographic and Professional Characteristics of Practitioners and Referral Practice for ENT Pat
Percentages in the “Referral Yes” and “Referral No” columns are calculated by row. Referral Practice for ENT Patients Among the 157 practitioners, 52.9% (n = 83) reported referring patients with ENT disorders to a higher-level healthcare facility, whereas 47.1% (n = 74) indicated that they did not practice referral.
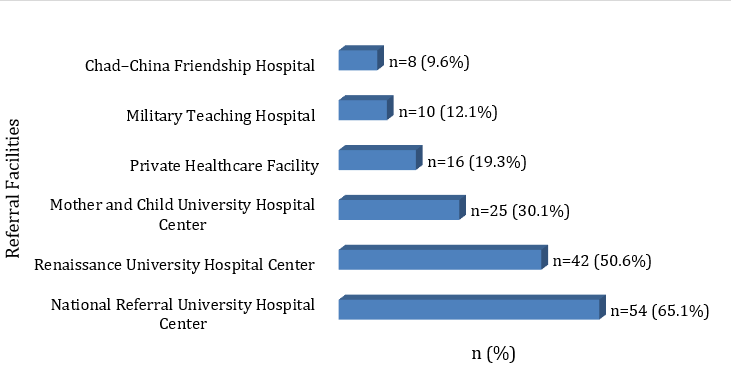
Among the 83 practitioners who reported referring patients, the most frequently cited referral destinations were the National Referral University Hospital Center (65.1%, n = 54) and the Renaissance University Hospital Center (50.6%, n = 42). The Mother and Child University Hospital Center was mentioned by 30.1% of practitioners (n = 25). Multiple responses were allowed. The distribution of referral facilities is presented in Figure 1.
Percentages were calculated among the 83 practitioners who reported referring patients. Multiple responses were allowed. The main criteria guiding referral decisions were lack of diagnostic resources (94.0%, n = 78) and perceived insufficient expertise (84.3%, n = 70). Therapeutic failure was reported by 41.0% of practitioners (n = 34). The criteria guiding referral decisions are illustrated in Figure 2.
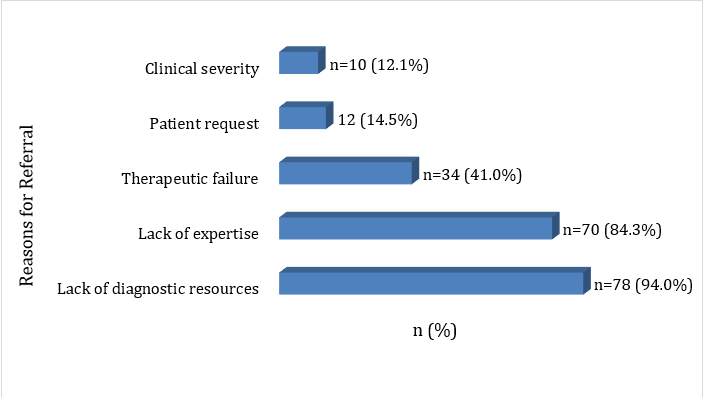
Percentages were calculated among practitioners who reported referring patients. Multiple criteria could be selected.
Counter-Referral Functionality
Among the 83 practitioners who reported referring patients with ENT disorders, 22.9% (n = 19) indicated that they received feedback following patient referral, whereas 77.1% (n = 64) reported receiving no feedback.
When counter-referral occurred, it was primarily verbal (16.9%, n = 14). Written reports were received by only 6.0% of practitioners (n = 5).
Factors Associated with Referral Practice
Bivariate analysis (Table 2) showed no statistically significant association between referral practice and sex (χ² = 0.15; p = 0.697), age group (χ² = 2.54; p = 0.771), professional qualification (χ² = 6.36; p = 0.095), or place of practice (χ² = 4.92; p = 0.178).
In contrast, professional experience was significantly associated with referral practice (χ² = 37.47; p < 0.001). After categorizing experience into two groups (≤10 years and >10 years), practitioners with ≤10 years of experience had significantly higher odds of referral compared with those with more than 10 years of experience. The strength of this association, detailed in Table 3, showed that these practitioners were 9.60 times more likely to refer patients (OR = 9.60; 95% CI: 4.37–21.07).
Practical ENT training was also significantly associated with referral practice (χ² = 13.10; p <0.001) (Table 2). As shown in Table 3, practitioners who had received ENT training had 8.54 times higher odds of referral compared with those without training (OR = 8.54; 95% CI: 2.44–29.91).
| Variable | χ² | p-value |
|---|---|---|
| Sex | 0.15 | 0.697 |
| Age group | 2.54 | 0.771 |
| Professional qualification | 6.36 | 0.095 |
| Place of practice | 4.92 | 0.178 |
| Years of professional experience | 37.47 | < 0.001 |
| Practical ENT training | 13.10 | < 0.001 |
Table 2: Association Between Practitioner Characteristics and Referral Practice for ENT Patients (n = 157) χ² = Pearson’s Chi-squ
| Variable | Compared Categories | OR | 95% CI | p-value |
|---|---|---|---|---|
| Years of professional experience | ≤10 years vs >10 years | 9.60 | 4.37– 21.07 | < 0.001 |
| Practical ENT training | Yes vs No | 8.54 | 2.44– 29.91 | < 0.001 |
Table 3: Factors Significantly Associated with Referral Practice for ENT Patients. OR = Odds Ratio; 95% CI = 95% Confidence Inter
Discussion
This study highlights a contrasted picture of the referral system for ENT disorders in district hospitals of N’Djamena. Among the practitioners surveyed, 52.9% reported referring patients to a higher level of care, whereas 47.1% indicated that they did not use referral. In addition, lack of feedback after referral was reported by 77.1% of referring practitioners. These findings suggest a partially operational referral system, characterized by patient transfer mechanisms but significant deficiencies in informational continuity.
Referral decisions were primarily driven by lack of diagnostic resources (94.0%) and perceived insufficient expertise (84.3%). These results reflect the structural constraints faced by district hospitals in a context marked by the scarcity of ENT specialists and their concentration in university hospital centers [9, 10, 11]. Referral therefore appears as an adaptive mechanism in response to limitations in technical infrastructure and human resources.
The fact that 47.1% of practitioners reported never referring patients requires careful interpretation. This situation may reflect substantial clinical autonomy or pragmatic adaptation to an environment where access to specialized facilities may be perceived as complex. Studies on referral practices in primary care show that such decisions depend not only on clinical criteria but also on organizational factors [5, 12]. Referral practice must therefore be understood within a broader systemic and contextual framework.
The limited functionality of counter-referral constitutes a central finding. The absence of feedback for 77.1% of practitioners indicates a disruption in continuity of care. Bidirectional information exchange is widely recognized as a key indicator of health system quality [4, 13]. Without structured reporting, patient follow-up becomes fragmented and opportunities for improving clinical practice are reduced. Similar observations have been reported in several sub- Saharan African settings [7, 8], suggesting that this challenge is structural rather than isolated.
The analysis of associated factors provides important insights. Professional experience was significantly associated with referral practice. Practitioners with ≤10 years of experience had significantly higher odds of referral compared with those with more than 10 years of experience (OR = 9.60; 95% CI: 4.37–21.07). This finding may reflect a more cautious approach among less experienced practitioners. Conversely, longer professional experience may favor greater autonomy in local management. While such autonomy represents a clinical asset, it may also reduce referral in certain situations. This observation underscores the importance of harmonized decision-making protocols regardless of years of experience.
Practical ENT training was the other factor significantly associated with referral practice. Practitioners who had received training had 8.54 times higher odds of referral compared with those without training (OR = 8.54; 95% CI: 2.44–29.91). This finding suggests that training enhances the ability to recognize cases requiring specialized evaluation. Improved competence does not appear to reduce referral but rather to enhance its appropriateness. Within the broader perspective of health system strengthening and universal health coverage [13, 14, 15], continuing professional development represents a strategic lever.
These results highlight the need for targeted organizational interventions. Formalizing referral pathways, introducing standardized communication tools, and establishing systematic counter-referral mechanisms could improve coordination between levels of care. In a context of limited specialized resources, optimizing interactions between healthcare structures appears to be a major determinant of system performance.
Several limitations should be acknowledged. The cross- sectional design does not allow causal inference. Because data were self-reported, social desirability bias cannot be excluded. Finally, the study was conducted exclusively in district hospitals of the capital city, which may limit generalizability at the national level.
Conclusion
This study demonstrates that the ENT referral system in district hospitals of N’Djamena is partially functional. Although referral practices are implemented by a substantial proportion of practitioners, counter-referral remains largely insufficient, indicating a disruption in informational continuity between levels of care.
Professional experience and practical ENT training emerged as significant determinants of referral decisions, highlighting the influence of competence and experience on patient care pathways. Specific training appears to promote earlier recognition of local management limits and more appropriate patient orientation.
In a context of limited specialized resources, strengthening coordination between healthcare facilities, formalizing referral pathways, and reinforcing continuing professional development constitute priority strategies to improve the quality and efficiency of ENT healthcare delivery in Chad.
Acknowledgments
The authors express their sincere gratitude to the administrative authorities of the district hospitals of N’Djamena for facilitating the conduct of this study. We also thank all practitioners who agreed to participate in the survey, as well as the collaborators who contributed to data collection and data entry.
Conflict of Interest
The authors declare that they have no conflicts of interest related to this study. No financial, institutional, or personal interests influenced the design, conduct, or reporting of this research.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request, in accordance with applicable ethical and confidentiality regulations.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki and received approval from the relevant institutional ethics committee prior to data collection. Participation was voluntary, written informed consent was obtained from all practitioners, and the collected data were anonymized and handled with strict confidentiality.
References
-
Marom T, Tan A, Wilkinson GS, Pierson KS, Freeman JL, et al. (2014) Trends in otitis media-related health care use in the United States 2001-2011. JAMA Pediatr 168(1): 68-75.
-
Schilder AG, Chonmaitree T, Cripps AW, Rosenfeld RM, Casselbrant ML, et al. (2016) Otitis media. Nat Rev Dis Primers 2(1): 16063.
-
Briggs DC, Ikenga VO, Oparaodu UA, Mbak E (2022) The pattern of paediatric otorhinolaryngological disorders seen at the Rivers State University Teaching Hospital, South-south Nigeria: a 3-year review. Pan Afr Med J 42: 94.
-
Kruk ME, Pate M, Mullan Z (2017) Introducing The Lancet Global Health Commission on High-Quality Health Systems in the SDG Era. Lancet Glob Health 5(5): e480-e481.
-
Mehrotra A, Forrest CB, Lin CY (2011) Dropping the baton: specialty referrals in the United States. Milbank Q 89(1): 39-68.
-
WHO (2018) Integrated referral systems: strengthening primary health care. World Health Organization, Geneva, Switerzland.
-
Kahabuka C, Moland KM, Kvåle G, Hinderaker SG (2012) Unfulfilled expectations to services offered at primary health care facilities: experiences of caretakers of underfive children in rural Tanzania. BMC Health Serv Res 12: 158.
-
Nakayuki M, Basaza AHD, Namatovu HK (2021) Challenges Affecting Health Referral Systems in Low- And Middle-Income Countries: A Systematic Literature Review. Eur J Health Sci 6(3): 33-44.
-
Fagan JJ, Jacobs M (2009) Survey of ENT services in Africa: need for a comprehensive intervention. Glob Health Action 2(1).
-
Mulwafu W, Ensink R, Kuper H, Fagan J (2017) Survey of ENT services in sub-Saharan Africa: little progress between 2009 and 2015. Glob Health Action 10(1): 1289736.
-
Fasunla AJ, Samdi M, Nwaorgu OG (2013) An audit of Ear,Nose and Throat diseases in a tertiary health institution in South-western Nigeria. Pan Afr Med J 14: 1.
-
Pittalis C, Brugha R, Gajewski J (2019) Surgical referral systems in low- and middle-income countries: A review of the evidence. PLoS One 14(9): e0223328.
-
Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, et al. (2018) High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Glob Health 6(11): e1196-e1252.
-
Give C, Ndima S, Steege R, Ormel H, McCollum R, et al. (2019) Strengthening referral systems in community health programs: a qualitative study in two rural districts of Maputo Province, Mozambique. BMC Health Serv Res 19(1): 263.
-
Blanchet K, Gordon I, Gilbert CE, Wormald R, Awan H (2012) How to achieve universal coverage of cataract surgical services in developing countries: lessons from systematic reviews of other services. Ophthalmic Epidemiol 19(6): 329-339.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?
- Allergic Rhinitis in Senegal: Epidemiological, Clinical and Therapeutic Aspects