Burden of Disease in Turkey, 2002-2019
Global Burden of Disease (GBD) was first introduced in the early nineties and has since played important roles in health care and public health planning for international communities as well as NGO’s (Non-governmental Organizations). Despite the significant importance of the conceptual framework surrounding GBD, it has recently come to attention that the type of public health and statistical language utilized in the description of GBD projects can provide a barrier of conceptual understanding for policy makers and non-health care providers. Therefore this paper attempts to provide a conceptual framework of the GBD analysis as well as its impact along with advantages and disadvantages found during the implementation and utilization of the data presented by Turkish Burden of Disease Studies (TBoD) in the year 2002-2013 as well as 2017 and 2019 GBD estimates.
Introduction
The GBD project was an improvement in quantifying the burden of specific diseases from the initial studies by and others (1986), who previously attempted to gather the same information. Hakulinen T, et al. [1] identified burdens of disease by grouping similar disease processes together. The data gathered and analyzed from the GBD 1990 study provided a framework by which public health and governmental entities can better focus and exercise their resources to implement the most effective and efficient improvement in population health. In addition, the GBD project was able to address the contribution of fatal and non-fatal effects of diseases, injuries, and risk factors on health outcomes for the first time. The non-fatal, or disability outcomes were determined to address the morbidity factors of disease. This analysis further provided an understanding of how disability secondary to disease can also negatively affect one’s well-being. The GBD was first measured by combining the mortality and morbidity data into a novel term entitled Disability Adjusted Life Years (DALY). This unique unit-DALY-measures health status using only one numerical value by combining number of deaths with the consequence of premature deaths and disability [2]. The DALY is a health gap measure that extends the concept of potential years of life lost (YLL) due to premature death to include equivalent years of health life lost by virtue of individuals being in states of poor health or disability (Years Lived with Disability-YLD) [3].
Murray CJL, et al. [4] were able to improve this methodology by dissecting the various groups (such as infectious diseases) into more specific subheadings (such as TB, HIV/AIDS, diarrheal diseases, meningitis, malaria, etc.) providing a clearer correlation between a specific disease etiology and the burden that disease (instead of a group of diseases) has had on the health of the population [3, 1].
The 1990 and 2000 GBD analyzed the burden of 135 major diseases and the 500 resultant sequelae [4]. In 2017 and 2019 GBD studies, those estimates, incidence, prevalence, mortality, years of life lost (YLLs), years lived with disability (YLDs), and disability-adjusted life-years (DALYs) for 369 diseases and injuries, for two sexes, and for 204 countries and territories [5].
Methodology
The methodology applied to develop the GBD framework is based on the following key pieces which all ultimately result in non-health well-being and/or death: distal socioeconomic and environmental cause’s àrisk factors àdisease and injuries impairment functional limitations and disability [6]. In the understanding and application of the aforementioned flow chart, which composes critical factors that influence the calculation of the DALY, GBD Turkish researchers for the first Turkish Burden of Disease Study (TBoD) first collected data on all-cause mortality based on population estimates. After having briefly analyzed the population structure of Turkey from the 2000 population census, age, sex and cause specific deaths from Turkish Demography and Health Surveys, death statistics from Turkish Standardization Institute, maternal deaths mortality reports, all related surveys performed in research areas about infant and child mortality etc., life tables and age sex and cause specific death rates have been developed in the light of the available data. The researchers also carried out a national verbal autopsy survey in order to be able to estimate the age, sex and cause specific death rates for the country accurately [7]. For YLD calculations, data was firstly obtained from records of public institutions that collect regular data, surveys at the national level, population censuses, burial licenses and published and unpublished national and international studies at the academic level, proceedings of various conferences, unpublished theses, and reports on Turkey’s regions prepared by national and international institutions. Another data source is the household survey conducted under the coverage of the first national BoD study [8, 9, 10, 11].
Secondary data concerning TBoD list were also collected from wide ranging published and unpublished surveys. 20,000 articles, dissertation theses, congress documents and reports have been evaluated and around 1100 articles were selected as relevant to the objectives of the study After having gathered all available data for each disease, the DISMOD program was used to check the consistency of variables on prevalence, incidence, remission, case-fatality, duration, mortality, and relative risk of mortality, and to estimate missing parameters specific for the diseases listed above [9, 10]. An expert panel was also convened in order to reach a consensus on parameters to be used in DISMOD in addition to disease categories and sequel which were developed within the framework of the disease models In addition, the panel was asked about some of the missing information from the search of secondary data The BoD study was repeated in the year 2013 after 10 years of the first study by using all the available data sources as explained above.
The 2017 and 2019 GBD trends for Turkey, 2017 and 2019 estimates for Turkey have been used which were published by Global Health Metrics to show the changes between the years. For GBD 2017, 2019 estimates, for DALY calculations, data was obtained from censuses, household surveys, census records and vital statistics, disease records, healthcare use, air pollution monitors, satellite imaging, disease notifications, and other sources in GBD 2017-2019 study [5]. As for GBD 2019 methodology, GBD 2019 Diseases and Injuries Collaborators analyzed the age-specific death rates per region based on cause. Cause-specific death rates and cause fractions were calculated using the Cause of Death Ensemble model and spatiotemporal Gaussian process regression. Cause- specific deaths were adjusted to match the total all-cause deaths calculated as part of the GBD population, fertility, and mortality estimates. Deaths were multiplied by standard life expectancy at each age to calculate YLLs. This resulted in the first component of the DALY calculation .In order to make the YLD measurement, data was collected in a variety of forms. The disease registry provided researchers with the incidence and prevalence of various diseases. Population surveys were further completed by individuals throughout the region and evaluated to better appreciate the impact and disability various diseases/injuries have on individuals. Longitudinal studies of the natural history of the disease process (including incidence, prevalence, duration, and complications) were conducted and gathered through epidemiological studies. DisMod- MR 2.1, a Bayesian meta-regression modeling tool, was used to ensure consistency between incidence, prevalence, remission, excess mortality, and cause-specific mortality for most causes. Prevalence estimates were multiplied by disability weights for mutually exclusive disease and injury squeal to calculate YLDs. Diseases and Injuries Collaborators also evaluated the results in the context of the Socio-demographic Index (SDI), a composite indicator of per capita income, years of education, and fertility rate for women younger than 25 years. The paper will identify advantages and disadvantages found during the implementation and utilization of the data from the Turkish Burden of Disease Studies for the years 2002-2013, 2017 and 2019 GBD estimates [5, 9, 10, 11]
Results
It is important to understand the changes in the disease profile between the first Global Burden of disease study in 2002, the figures from the 2013 study and the latest figures available from the 2017 and 2019 studies. In the Figure 1, the changes in the number of DALYs between the years are plotted.
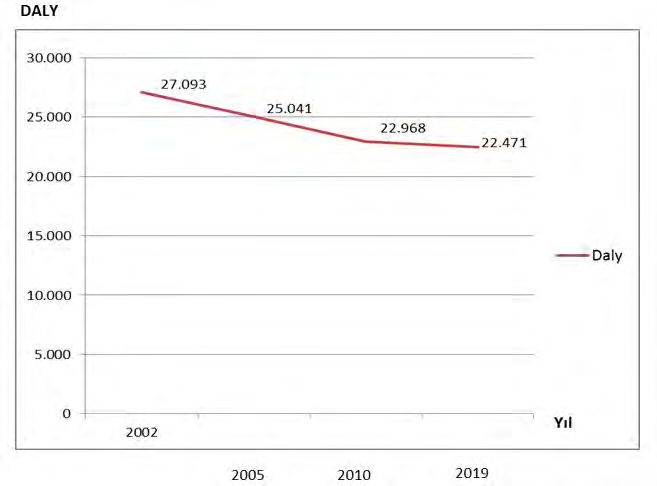
As seen in Figure 1, the number of DALY was determined as 27.093 (in million) in 2000 Turkish Burden of Disease Study but it dropped to 22.918 million in 2013 study then was estimated as 22.471 in the year 2019 which shows overall improvement of Burden of Diseases in Turkey.
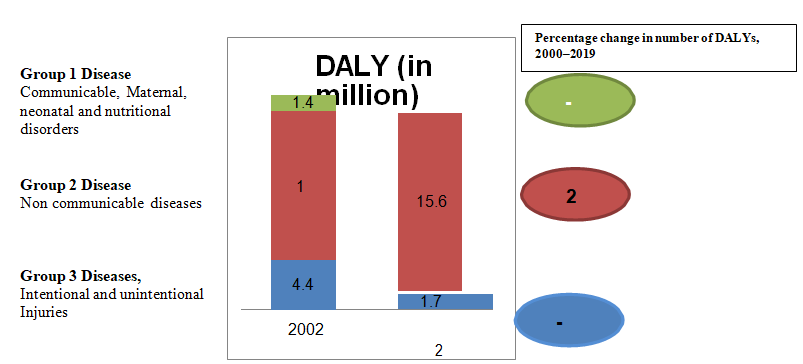
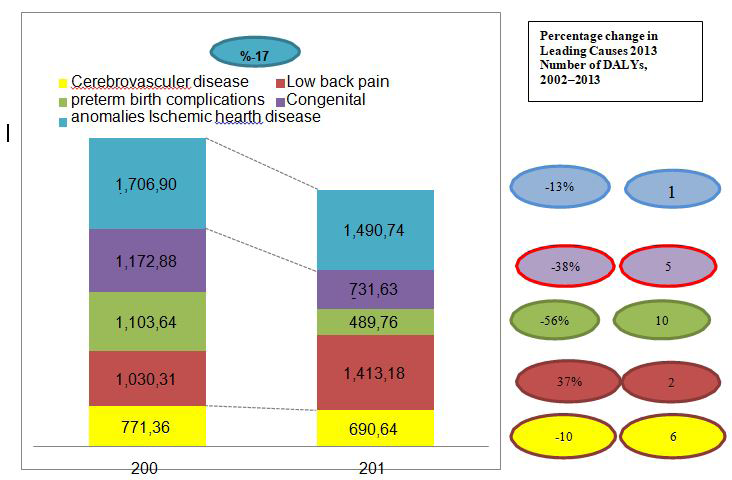
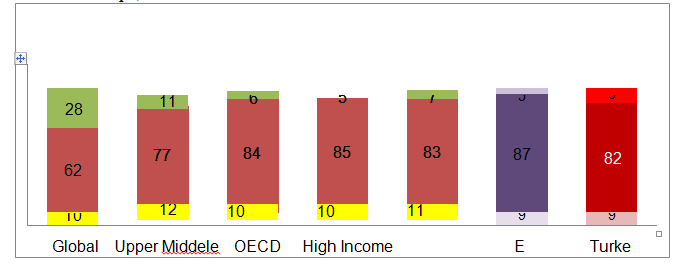
Figure 2 shows the distribution of DALY numbers (million) according to 3 groups of diseases between the years 2000 and 2019. While there was a 6.1% decrease in the Group 1 diseases (Communicable, Maternal, neonatal and nutritional disorders), an increase of 20% is observed in the Group 2, non-communicable diseases in 2019. There is also a 14% decrease in the third group diseases (Intentional and unintentional Injuries) during this period.
As seen in Figure 3, the overall burden of disease has decreased by 17% between the years 2002 and 2013. The rank of diseases in terms of DALY has also changed over the years except Ischemic heart disease (IHD), which was in the first rank in 2000, and continued to be in the first place in 2013; however a decrease of 13 percent was observed within
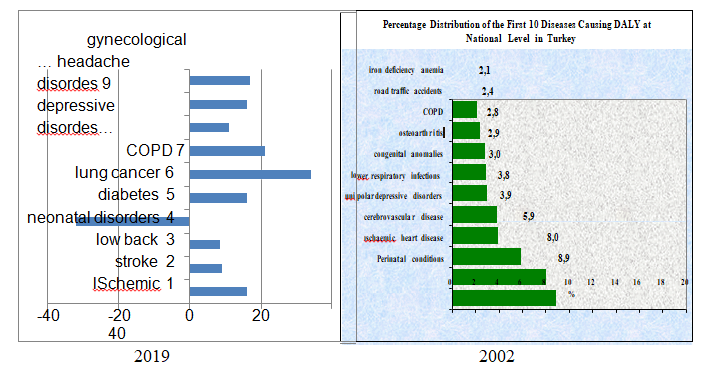
10 years. Congenital anomalies ranked 6th in the 2002 study, showed a 56% decrease in the 2013 study and fell to the 10th rank. On the other hand, low back pain, took second place with an increase of 37% in 2013. In Figure 4, the first ten burdens of disease in Turkey in 2002 and the changes in 2019 is given. As seen, ischemic heart disease occupies the first rank with cerebrovascular diseases and low back pain respectively in the year 2019. While it has been observed that neonatal disorders have decreased by 40% over the years, diabetes mellitus and lung cancer have increased which needs attention. It is significant that the distribution of major disease groups in Turkey is found to be very similar to EU figures. This is an important epidemiological trend which calls for appropriate policy changes in line with other countries in the region Figure 4.
Discussion
GBD came at an important time in public health history when more countries are under pressure (both externally and internally) to improve health conditions. Resource constraints are a major problem as governments are ―burdened‖ with how best to use the available resources effectively and most efficiently to promote population health. By providing a unique ―framework for integrating, validating, analyzing, and disseminating the fragmentary, and at times contradictory, information that is available on a population’s health, along with some understanding of how that population’s health is changing [8], the GBD framework provides information on how countries can most effectively allocate limited resources for gains in population health. The data gathered and analyzed from the GBD studies by the Institute for Health Metrics and Evaluations (IHME) could also provide a framework by which public health and government entities can better focus and exercise their resources to develop programs for improving population health [5]. Through the aforementioned analysis and cause of death estimates in Turkey, we observed that comparative analyses of the leading causes of death, and of premature death, form important evidence base to guide health development strategies [7, 8, 9, 10, 11]. The GBD approach for estimating mortality patterns is valuable because the methods adhere to epidemiological consistency across causes and preserve a sensible relationship between the level and cause of mortality [3, 4, 8]. However, we add that the strength and utility of GBD methodology depend on underlying data and this means that countries and policy makers have to improve current data collection systems. Furthermore, the sound and reliable structure of the GBD strategy encourages countries to improve their own data acquisition strategies which will provide evidence-base to their policy makers and public health officials to evolve appropriate policies and programs. Our examination also revealed the poor state of the data collection system in Turkey in the first TBoD study. Following difficulties in collecting mortality and morbidity data required for the first Burden of Disease project and the deficiencies observed in data collection systems, the Republic of Turkey and MoH improved mortality and morbidity data collection systems in the country and established country- wide computerized health information systems in each municipality and healthcare facilities. Therefore, with respect to Turkey, the GBD frameworks have been advantageous in the promotion of population health, as the available data show some important trends [7, 8, 9, 10, 11].
Global health has steadily improved over the past 30 years, as measured by changes in age-standardized DALY rates. While health has improved, after accounting for population growth and ageing, the absolute number of DALYs has remained stable and similar trends are also seen in Turkey (Figure 1) [12].
Of the deaths and DALYs worldwide, 30% are associated with Group I diseases, 60% with Group II and 10% with Group III. While lower respiratory infections, ischemic heart diseases, diarrhea, HIV/AIDS, prematurity and low birth weight are among the 10 most important causes of deaths in low-income countries, ischemic heart diseases, cerebrovascular diseases, respiratory system cancers, lower respiratory infections and chronic obstructive pulmonary diseases are prominent in high-income countries [5, 12, 13]. The ten most important diseases declining between 1990 and 2019 include Group 1 disease, which comprises nine diseases- lower respiratory infections, diarrheal diseases, neonatal disorders, measles, protein-energy malnutrition, congenital birth defects, drowning, tetanus, and malaria, as well as tuberculosis which largely affects adults. All these causes with declining burden also had substantial decreases in age-standardized DALY rates, ranging from 32-6%. It is also seen that major part of the causes of deaths of the people especially from the low-income group, observed in the youth age group are still associated with Group I diseases [5, 12, 13] However, compared to improvement gained against infectious agents, there has been insufficient progress in the prevention of diseases and controlling premature death from non-communicable diseases (NCD). An estimated 41 million people worldwide died of Group 2, Non Communicable Diseases in 2016, equivalent to 71% of all deaths. Four NCDs caused most of those deaths: cardiovascular diseases (17.9 million deaths), cancer (9.0 million deaths), chronic respiratory diseases (3.8 million deaths), and diabetes (1.6 million deaths) [12] Probability of dying from any of the four main Non communicable diseases between 30 and 70 years old decreased by 18% globally between 2000 and 2016. The highest decline is on chronic respiratory diseases (40% lower), followed by cardiovascular diseases and cancer (both 19% lower). However, diabetes increased by 5% leading to early death [14, 15].
According to Global Burden of Disease and Risk factor studies between the years 1990-2019, at least 80% of the early deaths and DALYs caused by heart diseases and stroke could be prevented through healthy nutrition, regular physical activity and prevention of tobacco smoking. The data show that a significant part of the deaths and DALYs worldwide are still associated with preventable reasons. Out of the ten most important diseases of increasing burden, ischemic heart disease, diabetes, stroke, chronic kidney disease, lung cancer, and age-related hearing loss largely affect older adults. The remaining four ie., HIV/AIDS, other musculoskeletal disorders, low back pain, and depressive disorders are common from teenage years into old age. Despite these ten conditions contributing the largest number of additional DALYs over the 30-year period, only HIV/AIDS, other musculoskeletal disorders, and diabetes saw large increases in age-standardized DALY rates, with an increase of 58·5% for HIV/AIDS, 30·7% for other musculoskeletal disorders, and 24·4% for diabetes [14, 15, 16]. This study shows that the distribution of risks affecting the DALYs observed in Turkey is rather similar to that of developed countries with low mortality. It can be assumed that this situation is based on the success gained during the last 50 years in preventing deaths of the below-five-years-old group, maternal deaths and deaths of young people. Although the priorities of the health system are changing, it is important to recognize the merging trends. This is because the Turkish health system has established its priorities on maternal and child health problems, communicable diseases, expansion of immunization and family planning services for many years. However, the data show that the priorities should be switched to non-communicable diseases such as cardiovascular and cerebrovascular diseases, cancers, obesity and diabetes.
The Ministry of Health initiated a Health Transformation Program in 2003, in which family physicians and primary health care services became the backbone of the health program. The program has been able to achieve some progress. However, we want to emphasize that the health profile of the country is still in the transition period and accessible and high quality health care is important for the development of a sustainable community. Therefore we need to put emphasis on primary health care services such as health centers, health houses, mother and infant health services and family medicine. As shown in the National Burden of Disease Study, the Turkish population is also becoming an aging population and in the coming years, this will be a dominant trend. It is therefore crucial that non- communicable diseases should be considered as important disease burdens in the near future. Family medicine and primary health should become the backbone of the health program to prevent such a disease trend as patients having chronic disease have to utilize health care facilities frequently and as a result, the demand will increase and so will the costs. Furthermore, these high-cost services create serious pressure on the social security systems and therefore family medicine and primary health care services can be involved in the follow-up of non-communicable disease which can help in the reduction of costs. even the vertical organization model that has previously provided significant contributions in the control of communicable diseases such as Tuberculosis and malaria may be an alternative in our agenda; e.g. Obesity clinics, diabetes clinics, etc... While the health personnel in these clinics provide monitoring and home care services, the required specialist support needed may be provided through the second- or tertiary care facilities. As previously stated, data collection was very difficult. It was also difficult to integrate the data as data dissemination and sharing are limited. It is also important to present the data in a user-friendly manner for the personnel and policy makers which will only enable them to utilize the essential data to improve health conditions. Regular interactions with medical professionals, policy makers, as well as the general public would help in improving the quality of data sets along with national and/or regional level follow- up meetings with policy.
Conclusion
The Turkish transition with respect to disease trends between 2002 and 2019 shows that the pattern is now similar to developed countries with the emerging Non- Communicable Disease (NCD) posing a major challenge for the health service system in the country. The analysis based on Global Burden of Disease framework attempted in this paper considerably helped in identifying the major shifts in the disease burden which necessitate a shift in the orientation of services. Given the demographic scenario and the aged population in the coming years and the high cost in the provision of care for Non Communicable Diseases, it is important to focus on a multi-level system with emphasis on primary and family care which can take care of follow-up activities. This will improve quality of care at the higher levels and by investing in primary health and related services, their quality and support systems can be considerably improved. Investment in rehabilitative and palliative services is also required given the pattern identified in our analysis. Accessibility and availability of data are a major problem that researchers face in many countries and this limitation was also felt in the present study. However, triangulation from multiple sources helped in filling the gaps which helped in identifying the trends presented in this paper. It is suggested that such analysis should be undertaken periodically to inform the policy process at the macro and micro levels.
References
-
Hakulinen T, Hansluwka H, Lopez AD, Nakada T (1986) Global and Regional Mortality Patterns by Cause of Death in 1980 Int J Epidemiol 15(2): 226-233.
-
Cole B, Kane C, Killeen M, Mohr W, Nield-Anderson L, et al. (2000) Responding to the Global Burden of Disease. ISPN White Paper.
-
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL (2006) Global Burden of Disease and Risk Factors. New York: Oxford University Press, pp: 29.
-
Murray CJL, Lopez AD (1996) The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and projected to 2020_._ Cambridge, Harvard University Press.
-
(2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A Systematic Analysis for The Global Burden of Disease Study 2019. Global Health Metrics 396(10258): 1204-1222.
-
Mathers CD, Stein C, Ma Fat D, Rao C, Inoue M, et al. (2002) The Global Burden of Disease 2000 Study (version 2): Methods and Results. Geneva: Global Program on Evidence for Health Policy. WHO, pp: 1-108.
-
Akgun S, Colak M, Bakar C (2012) Identifying and verifying causes of death in Turkey: National verbal autopsy survey. Public health 126(2): 150-158.
-
Akgun S (2004) Summary Measures of Health: Burden of Disease and Cost Effectiveness_,_ Ministry of Health Refik Saydam Hygiene Centre Presidency School of Public Health Baskent University: National Burden of Disease and Cost Effectiveness Project Household Survey Interim Report.
-
Akgun S, Chalapati R, Yardim N, Basara BB, Aydin O, et al. (2007) Estimating mortality and causes of death in Turkey: methods, results, and policy implications. Eur J Public Health 17(6): 593-599.
-
Baskent University (2005) Burden of Disease Final Report_._ Ankara, Turkey: Baskent University and the School of Public Health, Refik Saydam Hygiene Center, Ministry of Health.
-
(2004) Methodological Issues_-_A Case Study, Turkey. Submitted to World Bank, Ankara.
-
(2020) Monitoring health for the SDGs, sustainable development goals. World Health Organization.
-
Lopez AD, Mathers CD, Ezzati M, Jamison T, Christopher JL (2006) Measuring the Global Burden of Disease and Risk Factors, 1990-2001. Global Burden of Disease and Risk Factors, pp: 1-13.
-
(2018) Global Health Estimates: Deaths by Cause, Age, Sex, by country and by region, 2000-2016. Geneva, World Health Organization.
-
Mathers CD, Loncar D (2006) Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med 3(11): e442.
-
(2007) Institute for Health Metrics and Evaluation.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines