Isolation, Identification and Comparative Analysis of Oral Microbial Communities in Smokers and Non-Smokers: A Scientific Investigation
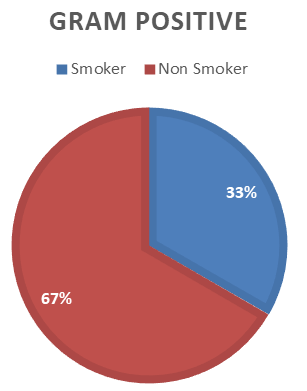
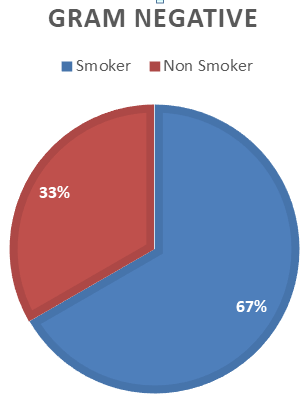
Smoking tobacco considerably changes the Gram-positive bacteria in saliva, including pathogens that may be involved in the development of tobacco-related illnesses such as periodontitis and peri-implantitis. A poor diet, poor oral hygiene, and other health problems can change the balance between these bacteria, allowing the dangerous bacteria to gain control. Pathogens can spread to distant places in the body if they overgrow in the mouth and blood vessels. Some bacteria have adapted to survive in the oral cavity by surviving within our bodies' defense mechanisms. Smokers are more likely to experience issues following gum and oral surgery, gum disease, tooth loss, decay on the roots of teeth, and oral cancer of the mouth. It has been reported that smoking has an impact on the oral microbiota, which has been connected to a number of human disorders. This study was designed for the isolation of bacteria from smokers and non-smokers. Oral health can be impacted by smoking. Smokers are more likely to experience issues following gum and oral surgery, gum disease, tooth loss, decay on the roots of teeth, and oral cancer of the mouth. The bacterial were isolated from the samples collected from non- smokers and smokers. The culture technique was used to grow bacteria. For further identification Gram staining, microscopy and biochemical tests were performed. Gram positive and gram negative bacteria were isolated from both smokers and non-smokers. The prevalence of gram positive bacteria was high in smokers and the prevalence of gram negative bacteria among smokers was high. Total 33% of gram positive bacteria were isolated from non-smokers and 67% from smokers. The gram positive species isolated were S. aureus and S. pneumoniae and 33% of gram negative bacteria were isolated from non-smokers and 67% from smokers. The gram negative species isolated were E.coli and K. pneumoniae.
Introduction
Microorganisms
Any living entity that is too small to be seen with the naked eye is referred to as a “micro-organism.” It starts with the earliest living creatures on our planet and includes an astounding variety of life forms [1].
Microscopically small, single-celled creatures called bacteria are abundant both inside and outside the human body. Some bacteria are dangerous and can infect people with a wide range of illnesses [2].
The three most prevalent microorganisms in the human body are viruses, fungus, and bacteria. They may be both beneficial and detrimental. While some microbes can cause harmful algae blooms, others can help with digestion, soil regrowth, and even oil spill cleanup [3].
Microbiome
The term “microbiome” refers to a group of microbes, including bacteria, viruses, fungus, and protozoa, as well as their genes and genomes, that live in a certain habitat. The gastrointestinal microbiome is the most complicated echo-system with 10-100 trillion microorganisms, with bacteria accounting for the majority of that population. Fungi and viruses came in second and third, respectively [4].
In addition to performing tasks for the host that it cannot do on its own, the microbes also give the host a favorable environment for the growth and development of its own bacteria. These host variables can influence the microbiome in a favorable way, increasing species variety and balance, leading to a symbiotic state and the lack of pathology. A dysbiotic state, in which the balance tips toward a deleterious relationship between the host and its microbiome, can be caused by other host variables, which can have a negative impact on the composition of the oral microbiome [5].
As a component of the human body, microorganisms colonize a variety of locations, with the mouth cavity being one of the densest populated environments. The oral cavity contains a variety of environments, the characteristics of which dictate the types of microbes that colonize the area, and the metabolic activities of these microbes later change the environmental characteristics. When in balance, these microorganisms promote health, but any change to the flora allow the harmful bacteria to proliferate and lead to oral diseases [6].
Oral Microflora
Microbes are everywhere in human existence and have an impact on every element of it. There are numerous diverse habitats in the human oral cavity. Variable oral bacteria work together and synergistically to protect the human body from outside stimuli. However, an imbalance in the microbial flora is a factor in both systemic and oral disorders. Oral microbiomes are crucial to the health of humans and the human microbial community [7].
Humans and their oral microbiota have a lifelong relationship that starts soon after birth [8]. After the gut, the oral cavity’s microbiome is the second-largest and most diverse microbiota, with approximately 700 different bacterial species as well as fungus, viruses, and protozoa. The oral cavity is an extremely complex ecology with a variety of niches where various bacteria preferentially inhabit distinct environments [9].
The oral microorganisms, which are dispersed in many niches including the dorsum of the tongue, mucosal surfaces, teeth, and saliva, have a diverse and distinct ecological habitat thanks to the heterogeneous nature of the oral tissues and structures. The only body region where mineralized hard tissues (the teeth) are naturally exposed to the outside environment is the mouth, which adds to the complexity of the oral microbiota. This resident bacterial flora actively contributes to the host defences that inhibit the colonisation of the host by exogenous microorganisms, which has a significant impact on the physiology of the host [7].
The tongue, soft and hard palate, teeth, buccal mucosa, and other separate, small microbial habitats all contribute to the complexity of the oral cavity, which is home to a diverse ecosystem with a high diversity of species [10].
The reasons behind the oral microbiome’s stability as one of the body’s most consistent ecosystems remain a mystery. Because the mouth has so many different niches, in addition to being steady, it is also much diversified [11].
A healthy adult’s mouth cavity is habitat to more than 400 types of commensal microorganisms. An abnormality in this ecology brought on by dietary practices, poor dental hygiene, or systemic causes increases the presence of cancer- causing microorganisms [12].
All people share the same core microbiome, yet each person has a different variable microbiome based on their lifestyle and physiological makeup. The hard and soft tissues of teeth and the oral mucosa, respectively, are two surfaces in the oral cavity where bacteria can invade.
The oral microflora host gains immunity to infections via prevention of pathogenic microbe colonization, development of both the innate and adaptive host immune systems, and fine-tuning of its reaction patterns to establish a balance between pro-inflammatory and anti-inflammatory reactions. The microbiome of the digestive system is extremely important for the host’s metabolism, as it makes it easier to obtain nutrients and energy from food, offers nutrients and auxiliary growth factors (such as vitamin K), and controls hormone and fat storage levels in the host. The balance between the microbiome and the host is necessary for the human microbiome to have positive effects. Asthma and atopic diseases, inflammatory bowel diseases, autoimmune diseases, obesity and metabolic syndrome, colon cancer, peripheral vascular disease and hypertension, aberrant drug reactions, depression, and autism are just a few of the systemic disorders that imbalance, or dysbiosis, is linked to. Many of these have been linked to drastically altered microbiome composition, but causal connections have not yet been shown [13].
There is mounting evidence linking human systemic diseases with the oral microbiota. Many oral bacteria have the potential to affect the inflammatory microenvironment, which may explain this connection. Even after excluding adverse variables like physical activity, poor oral health is tightly associated with an unhealthy body mass index [14].
Effect of Cigarette Smoking on Oral Microflora
Aspects of modern living, such as general dietary habits, sugar consumption, cigarette use, dental hygiene, use of antibiotics and other antimicrobials, and vaccinations, have an impact on the relative proportions of microbiome members.
An issue with public health is cigarette smoking. It causes an increase in harmful bacteria by reducing the commensal population of healthy flora in the mouth cavity. It has negative health effects such as halitosis, periodontitis, colour changes to the teeth, and oral cancer [15]. In the mouth, oral microbiota can generate metabolites that can influence the emergence of a variety of oral disorders [10].
Oral cancer is linked to the use of tobacco, alcohol, and areca nuts. Salivary microbiota has been sequenced by researchers to assess the effects of eating betel nut. Chewers of areca nuts were shown to have less bacterial diversity [16]. Smoking changes the oral cavity’s microbial composition by reducing the commensal microbial species and boosting the range of undesirable bacteria [17].
Cigarette smoking is a public health issue. It is the major cause of oral cancer, periodontitis, color change on the teeth, halitosis, and other health implications. It brings about a drastic decrease in the commensal population of normal flora in the oral cavity leading to an increase of pathogenic microbes [8].
Although there have long been recognised health disparities based on racial/ethnicity, socioeconomic position (SES), gender, and other sociodemographic characteristics, their underlying mechanisms are still not fully understood. Disparities in oral health outcomes have frequently been found to be racial/ethnic and socioeconomic [18]. The oral mucosa is affected by the carcinogens, creating a region that is vulnerable to developing cancer, or “field cancerization [19].” Esophageal adenocarcinoma (EAC) and esophageal squamous cell carcinoma (ESCC), the two primary forms, have very different incidence, geographic distributions, and etiologies. As incidence rates continue to climb, ESCC, the most prevalent kind globally, has taken over in industrialised countries, whereas EAC has replaced it. For both EAC and ESCC, known risk factors include alcohol use, low fruit and vegetable intake, and smoking, as well as gastroesophageal reflux disease (GERD), obesity, and smoking [20].
Nicotine exposure and cigarette smoking encourage the development of cariogenic oral bacteria and a caries-prone environment [21]. The oral cavity is significantly harmed by ingesting nicotine found in cigarette products. Periodontitis progresses more quickly as a result, with milder clinical signs and symptoms linked to treatment resistance. Additionally, smoking alters the microbiota of the oral cavity, bringing on more dangerous bacteria and infectious fungus [22].
According to estimates from the World Health Organization, tobacco use yearly kills about 6.4 million people and costs the global economy thousands of billions of dollars. It has long been known that smoking has a direct link to the growth of oral cancer. Cigarettes are typically produced from a variety of materials, including more than 60 carcinogens and cancer-promoting compounds that can enter the body’s numerous systems. The main carcinogens in tobacco are some of the flavorings that some tobacco businesses use to enhance the appeal of their products. The most frequent additives are the aromatic hydrocarbon benz-pyrene and the tobacco-specific nitrosamines (TSNs), particularly 4-(Nitrosomethylamino)-1-(3-pyridyl)-1- butanone (NNK) and N’-nitrosonornicotine (NNN) [23].
One of the most prevalent types of malignancies worldwide is oral cancer. It is a very complex illness, and lifestyle choices, particularly quitting smoking and consuming alcohol in moderation, can have a significant negative impact. Hypo salivation has multiple etiological factors and may have an impact on dental health as well as other facets of quality of life [24].
Materials and Methods
Patient Enrollment
Permission was taken from the individuals before collection of sample from oral cavity. Samples were taken from 36 individuals, from the students of Kohsar University Murree belonging to different regions.
Sample Collection
Collection of samples were done in sterile environment. 18 samples were collected from non-smokers and 18 from regular smokers. The sample was collected in sterile transport swabs to avoid any contamination. The samples were moved to the Kohsar University Murree for further processing and analysis.
Culture Media Preparation
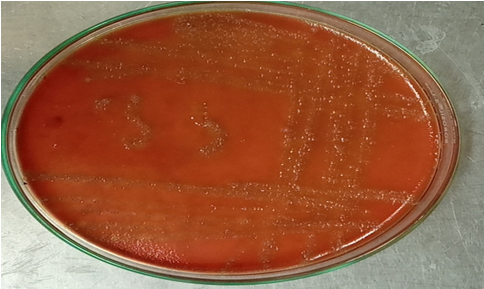
Nutrient Agar: Nutrient agar media is used for the growth of variety of non-fastidious microorganisms. In our study we use the nutrient agar for the growth of oral microbiota such as S. aureus, E.coli, Streptococcus species. To prepare this 40gm of nutrient agar was dissolved in 1000 ml of distilled water in a flask. The flask was then sealed with cotton and aluminum foil. It was autoclaved at 121°C for 15 minutes (Table 1).
| S. No | Ingredients | Gram/liter |
|---|---|---|
| 1 | Peptone | 5 |
| 2 | Yeast extract | 1.5 |
| 3 | Beef extract | 1.5 |
| 4 | Sodium chloride | 5 |
| 5 | Agar | 15 |
Table 3: Composition of Nutrient Agar. Final pH at (25℃): 7.4 ± 0.2
Tryptic Soy Agar: Tryptic soy agar is a non-selective media used for the cultivation of microorganisms. For the growth of S. aureus tryptic soy agar was used. To prepare this 40 gm of nutrient agar was dissolved in 1000 mL of distilled water in a flask. The flask was then sealed with cotton and aluminum foil. It was autoclaved at 121°C for 15 minutes (Table 2).
| S. No | Ingredients | Gram/liter |
|---|---|---|
| 1 | Pancreatic digest of casein | 17 |
Table 5: Composition of Tryptic soy Agar. Final pH (25℃): 7.3± 0.2
| 2 | Papaic digest of soybean meal | 3 |
|---|---|---|
| 3 | Sodium chloride | 5 |
| 4 | Dextrose (glucose) | 2.5 |
| 5 | Dipotassium hydrogen phosphate | 2.5 |
| 6 | Agar | 15 |
Table 1: Composition of Tryptic soy Agar. Final pH (25℃): 7.3± 0.2
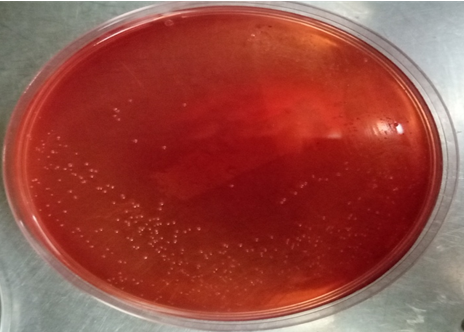
Blood Agar: For the growth of hemolytic specie such as Streptococcus species blood agar was used. To prepare this 40 gm of nutrient agar was dissolved in 1000 ml of distilled water in a flask. The flask was then sealed with cotton and aluminum foil. It was autoclaved at 121c for 15 minutes (Table 3).
| S. No | Ingredients | Gram/liter |
|---|---|---|
| 1 | Lab-lemco powder | 10 |
| 2 | Peptone neutralized | 10 |
| 3 | Sodium chloride | 5 |
| 4 | Agar | 15 |
Table 2: Composition of Blood Agar. Final pH (25℃): 7.2±0.2
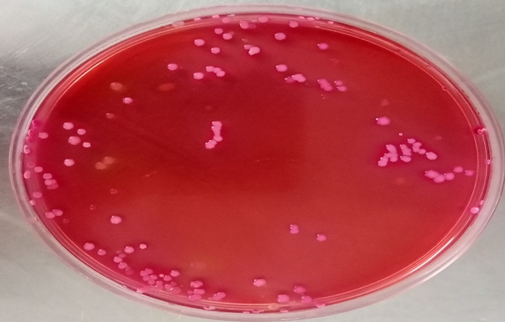
MacConkey Agar: MacConkey agar is a selective media used for the isolation of gram negative enteric Bacteria. For the growth of E. coli MacConkey agar was used. To prepare this 51.5gm of nutrient agar was dissolved in 1000 ml of distilled water in a flask. The flask was then sealed with cotton and aluminum foil. It was autoclaved at 121c for 15 minutes (Table 4).
| S. No | Ingredients | Gram/liter |
|---|---|---|
| 1 | Peptone | 20 |
| 2 | Lactose | 10 |
| 3 | Sodium chloride | 5 |
| 4 | Bile salts No. 3 | 1.5 |
| 5 | Crystal violet | 0.001 |
| 6 | Agar | 15 |
Table 4: Composition of MacConkey Agar. Final pH (25℃): 7.1± 0.2
Pouring of Media
The media was poured in sterile petri plates after autoclaving the media at 121°C for 15 minutes inside the biosafety cabinet.
Culturing
Samples were spread using sterile transport swabs on the nutrient agar plates. Samples were incubated for 24 hours at 37°C. After 24 hours growth of bacteria was examined.
Sub Culturing of Bacteria on Differential Media: Different colonies were examined after incubation. For the identification of the grown species biochemical tests, gram staining was performed and the bacteria were sub cultured on differential media using streak plate method to obtain pure cultures.
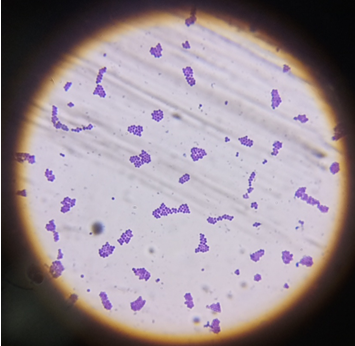
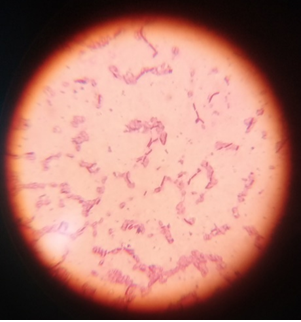
Gram Staining
Microscopy was established to identify the shape of bacteria. From the pure culture, single and separate colony was taken by using sterile loop and then a thin smear of isolate was prepared. The heat was used to fix the slide by passing on flame. The procedure of gram staining is given below.
- First, the crystal violet was applied to the smear for approximately 1 min. After 1 min slide was washed with tap water.
- After that, the smear was then treated with Gram’s iodine for 1 min and then washed rapidly using tap water.
- A drop of decolorizer was then poured on the slide and washed after 30sec using tap water.
- In the last Gram’s safranin was then applied on slide for 1 min and then slide was washed with the tap water. After staining, slide was kept at room temperature to air dry and then observed under microscope.
Biochemical Tests
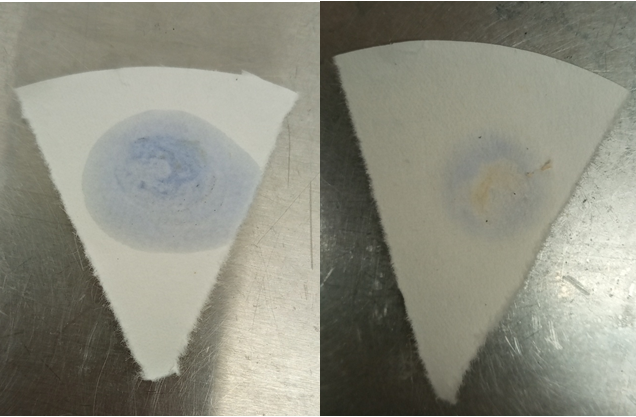
Catalase Test: A test that is performed to differentiate among the organisms that can produce enzyme catalase and those cannot. The test was performed by taking the small single colony from pure culture and was then mixed with 2 to 3 drops of 3% H2O2 or hydrogen peroxide on a slide. The bacteria that can produce catalase reduce hydrogen peroxide and generate or produce bubbles. The test was performed inside biosafety cabinet Oxidase Test: Oxidase test was performed to identity whether the bacteria had the oxidase enzyme. Oxidase solution was prepared by adding 0.1g of oxidase reagent in 10ml of distilled water. Add drop of oxidase reagent on filter paper. Add loop full of bacteria on the filter paper, it col0r changed to purple color within 5-10 seconds the bacteria were oxidase positive. If n0 color changing occurs, then it was oxidase negative.
Antibiotic Sensitivity and Resistance
For detection and analysis of resistance and susceptibility pattern of different pathogenic aerobic and anaerobic bacteria, Kirby Bauru disc diffusion method was applied.
Muller Hinton Agar: Muller Hinton agar is a media, which is mostly used for antibiotic susceptibility testing. Muller Hinton has properties that make it excellent for antibiotic use. It is a non-selective non differential media that promote the growth of all bacteria (Table 5).
| S. No | Ingredients | Gram/liter |
|---|---|---|
| 1 | Beef extract | 2 |
| 2 | Acid hydrolysate of casein | 17.5 |
| 3 | Starch | 1.5 |
| 4 | Agar | 17 |
Table 6: Composition of Muller Hinton Agar. Final pH at (25℃): 7.3 ± 0.1
Making of PBS Solution: PBS solution was prepared by adding 1 tablet of PBS in 100 mL distilled water. The solution was autoclaved at 121°C for 15 minutes to sterile the solution.
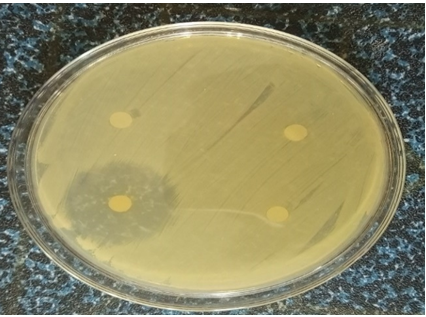
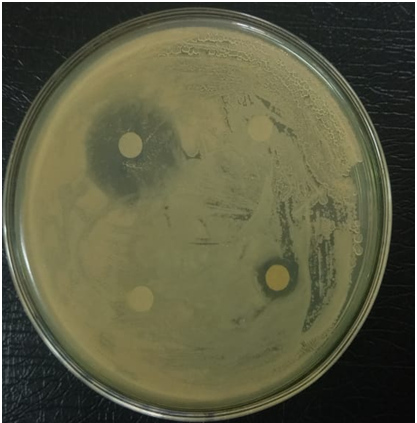
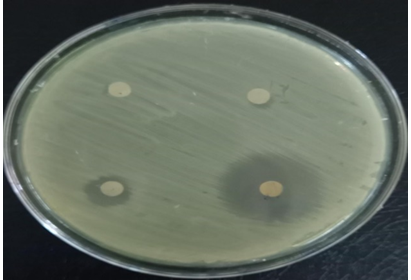
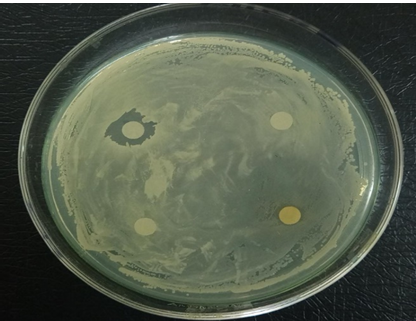
Application of Antibiotic discs: PBS solution and Mueller Hinton Agar was prepared and autoclaved. PBS was poured in the falcon tubes and colonies from the specific strains of bacteria were added in it. Mueller Hinton Agar was poured onto the petri plates and bacteria were grown on the Mueller Hinton agar. In the PBS solution cotton swab was dipped and streaked the swab all over the surface of media to form bacteria lawn. Antibiotic discs were placed on the media at equal distance with the help of sterile forceps. Ceftriaxone, Cefoxime and Azithromycin antibiotic discs were used to analyze the resistance and susceptibility of pathogens. After 24 hours measured the zone of inhibition with the help of ruler.
Reading of Plates: The plates were examined after incubation for 24 hrs. The zones observed were measured using ruler and the results were compared to CLSI.
Results
Total 36 samples were collected from oral cavity out of which 18 individuals are regular smokers and 18 individuals are non-smokers. The samples were collected from the students of University of Haripur belonging to different regions of Pakistan. Bacterial species which were isolated from non-smokers were consist of 67% of gram positive bacteria and 33% of gram negative bacteria. Bacterial species isolated from smokers consist of 33% of gram positive bacteria and 67% of gram negative bacteria (Figures 1 & 2).
Isolated species
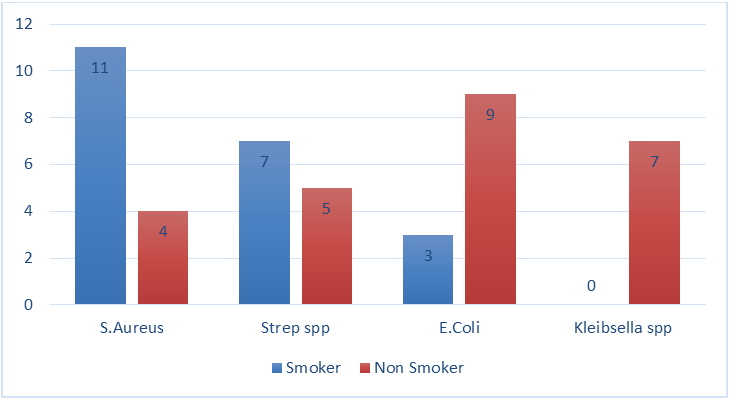
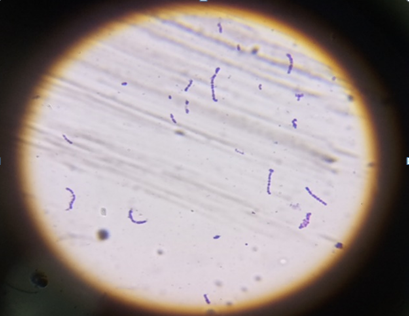
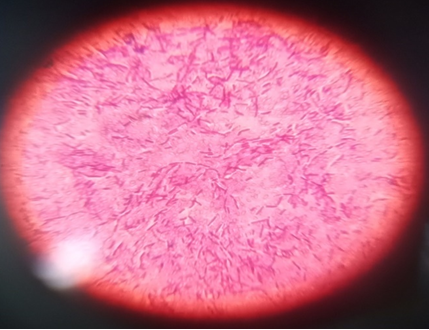
Various species of gram positive and gram negative bacteria were isolated from the samples of smokers and non-smokers. Among non-smokers the gram positive S. aureus and Streptococcus spp. were isolated. Gram negative E. coli was also isolated from the non-smoker. Gram positive S. aureus and Streptococcus spp. were also isolated from smokers. Gram negative Kleibsella spp. and E.coli were also isolated from smokers (Figures 4-21). S. aureus was found in high rates in non-smokers than smokers. Strep s and E. coli were found in high rates in smokers than non-smokers.
Kleibsella spp. were isolated from smokers only (Figure 3). Biochemical tests such as catalase test and oxidase test were performed and results are given in tables 6-8.
| Sample | Shape | Surface | Color | Gram Staining | Microscopy | Catalase | Oxidase |
|---|---|---|---|---|---|---|---|
| 1 | Round | Smooth | Golden yellow colonies | + | Cocci | - | - |
| Raised | |||||||
| 2 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 3 | Round | Smooth | Golden yellow colonies | + | Cocci | - | - |
| Raised | |||||||
| 4 | Large thick and convex | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 5 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 6 | Round and convex | Smooth | Golden | + | Cocci | + | - |
| Raised | Yellow colonies | ||||||
| 6 | Round | Smooth | Golden yellow colonies | + | Cocci | + | - |
| Raised | |||||||
| 7 | Round | Smooth | Golden yellow colonies | + | Cocci | + | - |
| 8 | Round and convex | Smooth and raised | Golden yellow colonies | + | Cocci | + | - |
| 9 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 10 | Large thick and convex | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 11 | Large thick and convex | Shiny and Smooth | Greyish | - | Rods | + | - |
| Colonies | |||||||
| 12 | Round | Smooth and raised | Golden yellow colonies | + | Cocci | + | - |
| 13 | Round and convex | Smooth | Golden yellow colonies | + | Cocci | + | - |
| 14 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 15 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 16 | Round | Smooth | Golden yellow colonies | + | Cocci | + | - |
| 17 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 18 | Round and convex | Smooth and raised | Golden yellow colonies | + | Cocci | + | - |
| 19 | Round | Smooth and raised | Golden yellow colonies | + | Cocci | + | - |
| 20 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 21 | Round | Smooth and raised | Golden yellow colonies | + | Cocci | + | - |
| 22 | Large thick and convex | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 23 | Large thick and convex | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 24 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
| 25 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 26 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
| 27 | Round | Smooth and Raised | Golden yellow colonies | + | Cocci | + | - |
| 28 | Large thick and convex | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 29 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 30 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
| 31 | Large thick and convex | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 32 | Round | Smooth and Raised | Golden yellow colonies | + | Cocci | + | - |
| 33 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
| 34 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 35 | Large thick and convex | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 36 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
| 37 | Round | Smooth | Golden yellow colonies | + | Cocci | + | - |
| 38 | Large and thick | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 39 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
| 40 | Round | Smooth | Golden yellow colonies | + | Cocci | + | - |
| 41 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 42 | Large and thick | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 43 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
| 44 | Round and small | Smooth | Greyish colonies | + | Cocci | - | - |
| 45 | Large and thick | Shiny and Smooth | Greyish colonies | - | Rods | + | - |
| 46 | Round | Smooth | Golden yellow colonies | + | Cocci | + | - |
| 47 | Large and thick | Shiny and smooth | Greyish colonies | - | Rods | + | - |
| 48 | Large and Round | Mucoid and opaque | Yellow or cream colonies | - | Rods | + | - |
Table 7: Features of Bacterial Species Isolated from Samples.


| Antibiotics | Conc. | Resistance | Intermediate | Susceptibility |
|---|---|---|---|---|
| Cefotaxime | 30mg | ³ 23 | 15–22 | £ 14 |
| Ceftriaxone | 30mg | ³ 21 | 14–20 | £ 13 |
| Ceftriaxone | 15mg | ³ 21 | 15–20 | ≤ 8 |
| Azithromycin | 15mg | ³ 18 | 14–17 | £ 13 |
Table 8: Antibiotic Zone Diameters Breakpoints.
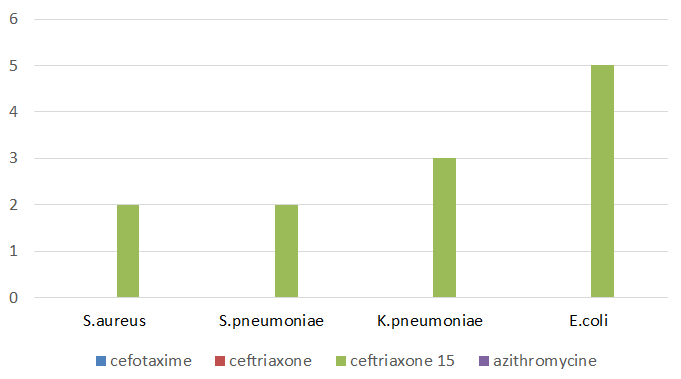
| Strains | Cefotaxime | Ceftriaxone | Ceftriaxone | Azithromycin |
|---|---|---|---|---|
| S. aureus | 28mm | 12mm | 0mm | 0mm |
| S. aureus | 10mm | 0mm | 0mm | 11mm |
| E. coli | 11mm | 0mm | 0mm | 0mm |
| K. pneumoniae | 13mm | 0mm | 0mm | 0mm |
| S. pneumoniae | 0mm | 0mm | 0mm | 11mm |
Table 9: Zone of Inhibition.
Discussion
In current study, total 4 bacterial species were isolated from 36 samples of smokers and non-smokers. Species were isolated based on morphology. Biochemical tests were performed including catalase and oxidase. Identification was done based on catalase positive or catalase negative, oxidase positive or oxidase negative. Different species of gram positive and gram-negative bacteria were isolated from the samples of smokers and non-smokers. Among non-smokers, the gram-positive S. aureus and Streptococcus spp. were isolated. Gram negative E. coli was also isolated from the non- smoker. Gram positive S. aureus and S. pneumoniae were also isolated from smokers. Gram negative K. pneumoniae and E. coli were also isolated from smokers. S. aureus was found in high rates in non-smokers than smokers. S. pneumoniae and E. coli were found in high rates in smokers than non- smokers. Klebsiella spp. Were isolated from smokers only. Total 33% of gram positive bacteria were isolated from non- smokers and 67% from smokers. The gram positive species isolated were S. aureus and S. pneumoniae and 33% of gram negative bacteria were isolated from non-smokers and 67% from smokers. The gram negative species isolated were E. coli and K. pneumoniae.
The results indicates the overall change among the oral microbiota of smokers and non-smokers. So, it’s obvious that the smoking has adverse effects and can play its role in the shift of oral microbiota and can hinder the overall stability and can cause many diseases by allowing the colonization of external pathogenic bacteria by inhibiting the normal flora.
Alghamdi [25] in 2019 conducted a study on isolation of 15 different bacterial strains, of which 8 were gram positive and 7 were gram negative. Streptococcus pneumoniae (n = 26) dominated the gram positive strain species. Enterobacteriaceae (19.36%) and Streptococcaceae (13.83%) were the two most abundant families. Also isolated was one of the most cariogenic strains of Klebsiella pneumoniae (n = 14) [26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38].
Conclusion
Smoking is a serious health problem, which is leading to many diseases. One of the serious cause is oral cancer. It is also altering the commensal microflora, which is leading to many gum and teeth diseases. The bacteria present in the oral cavity are becoming resistant to antibiotics, which is a life threat to human being.
Summary
Oral microflora, often known as the microflora of the oral cavity, is abundant and diverse. Biofilms adhered to the various soft and hard tissue surfaces of the oral cavity generally contain oral microorganisms. We benefit from oral microbiota, which is crucial to the healthy growth of physiology. Additionally, it aids in host defense, but it can also have serious negative consequences on general health. These microorganisms are part of a complex ecological community that has an impact on oral and systemic health. How the topic of how microorganisms impact their hosts’ physiology is approached in the study of the human microbiome has undergone a revolution. Salivary Gram-positive bacteria, including pathogens that may play a role in the emergence of tobacco-related diseases such periodontitis and peri- implantitis, are significantly altered by smoking tobacco. Poor diet, poor oral hygiene, and other health issues, allowing the hazardous bacteria to take control, can alter the balance of these bacteria. If pathogens get out of control in your mouth and blood vessels, they can move to distant parts of your body. Some bacteria have evolved to live in our bodies’ defense mechanisms in order to survive in the oral cavity. Smokers are more prone to encounter complications after oral and gum surgery, gum disease, tooth loss, root decay, and oral cancer. According to reports, smoking has an effect on the oral microbiota, which has been linked to a number of diseases in people.
This study was designed for the isolation of bacteria from smokers and non-smokers. Oral health can be impacted by smoking. Smokers are more likely to experience issues following gum and oral surgery, gum disease, tooth loss, decay on the roots of teeth, and oral cancer of the mouth. The bacterial were isolated from the samples collected from non- smokers and smokers. The culture technique was used to grow bacteria. For further identification Gram staining, microscopy and biochemical tests were performed. Gram positive and gram-negative bacteria were isolated from both smokers and non-smokers. The prevalence of gram-positive bacteria was high in smokers and the prevalence of gram negative bacteria among smokers was high.
Isolation of bacteria was done using culture technique. Bacterial species were identified based on morphology of colonies, gram staining, microscopy and biochemical tests. This study revealed that there is a difference in Microflora of healthy person and the person who smokes tobacco. The prevalence of gram-positive bacteria was observed high in non-smokers than smokers. The prevalence of gram-negative bacteria was high in smokers as compared to non-smokers.
The isolated bacteria from smokers showed high resistance towards antibiotics which shows that the pathogens can easily invade the defense system of human body causing various diseases.
References
-
Flint HJ (2020) Why Gut Microbes Matter. Springer, New york, US, pp: 1-8.
-
Nagendra L, Boro H, Mannar V (2022) Bacterial Infections in Diabetes. Endotext.
-
Tillman S (2018) The Good, the Bad, and the Microscopic. Microreviews in Cell and Molecular Biology 4(2).
-
Gill SR, Pop M, DeBoy RT, Eckburg PB, Turnbaugh PJ, et al. (2006) Metagenomic analysis of the human distal gut microbiome. science 312(5778): 1355-1359.
-
Ulloa PC, van der Veen MH, Krom BP (2019) Review: Modulation of the oral microbiome by the host to promote ecological balance. Odontology 107(4): 437- 448.
-
Hegde MN, Mrinalini (2018) Dysbiosis of Oral Microflora: A Review. Journal of Health and Allied Sciences NU, 8(4): 34-39.
-
Prakash GP, Sangeetha RP, Nidhi T, Gokul S (2018) Oral bacterial flora and oral cancer: The possible link?. Journal of oral and maxillofacial pathology 22(2): 234-238.
-
Ilankizhai RJ, Leelavathi L (2018) Comparison of oral microbiota among smokers and non-smokers-A pilot study. Drug Invention Today 10(1): 2669-2673.
-
Caselli E, Fabbri C, D’Accolti M, Soffritti I, Bassi C, et al. (2020) Defining the oral microbiome by whole-genome sequencing and resistome analysis: the complexity of the healthy picture. BMC microbiology 20(1): 1-19.
-
Lu M, Xuan S, Wang Z (2019) Oral microbiota: A new view of body health. Food Science and Human Wellness 8(1): 8-15.
-
Carpenter GH (2020) Salivary factors that maintain the normal oral commensal microflora. Journal of dental research 99(6): 644-649.
-
Jayashri P, John J, Arumugham IM, Kumar RP, Sakthi DS (2018) Comparing the effectiveness of probiotic, green tea, and chlorhexidine-and fluoride-containing dentifrices on oral microbial flora: A double-blind, randomized clinical trial. Contemporary clinical dentistry 9(4): 560-569.
-
Kilian M (2018) The oral microbiome–friend or foe? European journal of oral sciences 126 (Suppl 1): 5-12.
-
Peng X, Cheng L, You Y, Tang C, Ren B, et al. (2022) Oral microbiota in human systematic diseases. International Journal of Oral Science 14(1): 1-11.
-
Ogba OM, Ewa JJ, Olorode OA, Mbah M (2017) Effect of tobacco smoking on oral microbial flora and the relationship with oral health in Calabar, Nigeria. International Journal of Biomedical Laboratory Science 6(1&2): 1-5.
-
Hernandez BY, Zhu X, Goodman MT, Gatewood R, Mendiola P, et al. (2017) Betel nut chewing, oral premalignant lesions, and the oral microbiome. PLOS One 12(2): e0172196.
-
Al-Zyoud W, Hajjo R, Abu-Siniyeh A, Hajjaj S, et al. (2020) Salivary microbiome and cigarette smoking: A first of its kind investigation in Jordan. International Journal of Environmental Research and Public Health 17(1): 256.
-
Renson A, Jones HE, Beghini F, Segata N, Zolnik CP, et al. (2019) Sociodemographic variation in the oral microbiome. Annals of epidemiology 35: 73-80.
-
Gholizadeh P, Eslami H, Yousefi M, Asgharzadeh M, Aghazadeh M, et al. (2016) Role of oral microbiome on oral cancers, a review. Biomedicine & Pharmacotherapy 84: 552-558.
-
Peters BA, Wu J, Pei Z, Yang L, Purdue MP, et al. (2017) Oral microbiome composition reflects prospective risk for esophageal cancers. Cancer research 77(23): 6777- 6787.
-
Wu J, Li M, Huang R (2019) The effect of smoking on caries-related microorganisms. Tobacco Induced Diseases 17: 32.
-
Trybek G, Aniko-Wlodarczyk M, Preuss O, Kuligowski P, Gabrysz-Trybek E, et al. (2018) The effect of nicotine on oral health. Baltic Journal of Health and Physical Activity 10(2): 7-13.
-
Kakabadze MZ, Paresishvili T, Karalashvili L, Chakhunashvili D, Kakabadze Z (2020) Oral microbiota and oral cancer: Review. Oncology Reviews 14(2): 476.
-
Lingstrom P, Mattsson CS (2020) Oral Conditions. In: Zohoori FV (Eds.), The Impact of Nutrition and Diet on Oral Health, Karger Publishers, Basel, Switzerland pp:14-21.
-
Alghamdi S (2022) Isolation and identification of the oral bacteria and their characterization for bacteriocin production in the oral cavity. Saudi Journal of Biological Sciences 29(1): 318-323.
-
Nimish DP, Revathi D (2019) Oral microbiome: Unveiling the fundamentals. Journal of oral and maxillofacial pathology 23(1): 122.
-
Ertel A, Eng R, Smith SM (1991) The differential effect of cigarette smoke on the growth of bacteria found in humans. Chest 100(3): 628-630.
-
Gopinath D, Wie CC, Banerjee M, Thangavelu L, Kumar RP, et al. (2022) Compositional profile of mucosal bacteriome of smokers and smokeless tobacco users. Clinical oral investigations 26(2): 1647-1656.
-
Grine G, Royer A, Terrer E, Diallo OO, Drancourt M, et al (2019) Tobacco smoking affects the salivary gram- positive bacterial population. Frontiers in Public Health 7: 196.
-
Jiang X, Jiang X, Wang Y, Huang R (2019) Correlation between tobacco smoking and dental caries: A systematic review and meta-analysis. Tobacco induced diseases 17(Suppl 1): A66.
-
Kauss AR, Antunes M, Zanetti F, Hankins M, Hoeng J (2022) Influence of tobacco smoking on the development of halitosis. Toxicology Reports 9: 316-322.
-
Martellacci L, Quaranta G, Fancello G, D’addona A, Sanguinetti M, et al. (2020) Characterizing peri-implant and sub-gingival microbiota through culturomics. first isolation of some species in the oral cavity. a pilot study. Pathogens 9(5): 365.
-
Nagarajan K, Geetha RV (2020) Comparative analysis of oral microbial flora of smokers and non-smokers with periodontitis. Drug Invention Today 14(7): 1206.
-
NorderGrusell E, Dahlen G, Ruth M, Ny L, Quiding‐ Jarbrink M, et al. (2013) Bacterial flora of the human oral cavity, and the upper and lower esophagus. Diseases of the Esophagus 26(1): 84-90.
-
Shakhatreh MAK, Khabour OF, Alzoubi KH, Masadeh MM, Hussein EI et al. (2018) Alterations in oral microbial flora induced by waterpipe tobacco smoking. International journal of general medicine 11: 47-54.
-
Srivastava A, Mishra S, Verma D (2021) Characterization of oral bacterial composition of adult smokeless tobacco users from healthy Indians using 16S rDNA analysis. Microbial ecology 82(4): 1061-1073.
-
Wu J, Peters BA, Dominianni C, Zhang Y, Pei Z, et al. (2016) Cigarette smoking and the oral microbiome in a large study of American adults. The ISME journal 10(10): 2435-2446.
-
Zhang Y, Wang X, Li H, Ni C, Du Z et al. (2018) Human oral microbiota and its modulation for oral health. Biomedicine & Pharmacotherapy 99: 883-893.
- Evaluation of Proximate and Mineral Compositions of Momordica charantia L. (Cucurbitaceae)
- Targeting Superbugs: Efficacy of Bacteriophage Therapy against Antibiotic-Resistant Pseudomonas Aeruginosa in Urinary Tract Infections
- Genetic Insights into Prepubertal Gynecomastia: A Comprehensive Analysis of a Rare 45,X[2]/ 46,X, + mar[28] Karyotype
- The Efficiency of Biological Treatment Plants in Some Private Hospitals in the City of Basra, Iraq
- Exploring the Combined Efficacy of Carvacrol and Friedelin against Multi-Drug Resistant Bacteria in Upper and Lower Respiratory Tract Infections
- Commercial Utilization of Microbial Polysaccharides: A Brief Global Perspective