Targeting Superbugs: Efficacy of Bacteriophage Therapy against Antibiotic-Resistant Pseudomonas Aeruginosa in Urinary Tract Infections
The rise of antibiotic-resistant bacterial infections poses a significant challenge to global health, particularly in the treatment of urinary tract infections (UTIs). This study evaluates the potential of bacteriophage therapy as an alternative treatment against antibiotic-resistant Pseudomonas Aeruginosa isolated from UTI samples. We isolated 12 strains of P. aeruginosa from 50 UTI samples and conducted extensive antibiotic susceptibility testing, revealing significant resistance to multiple conventional antibiotics such as Tetracycline, Septran, Ceftazidime, and Cefepime, while showing susceptibility to Imipenem and Meropenem. Concurrently, we isolated and characterized bacteriophages from sewage samples that demonstrated specific lytic activity against the antibiotic-resistant strains. Our findings suggest that bacteriophage therapy provides a high specificity and efficacy in targeting antibiotic-resistant P. aeruginosa, offering a promising alternative to traditional antibiotic therapies. This study underscores the potential of phages in clinical applications, advocating for further clinical trials and the development of a regulatory framework to integrate phage therapy into mainstream medical practice for combating antibioticresistant infections.
Introduction
The relentless rise of antibiotic resistance among bacterial pathogens poses a formidable challenge to global health, with urinary tract infections (UTIs) standing as a poignant example of this growing crisis [1]. UTIs, among the most common infectious diseases, affect millions worldwide, leading to significant morbidity, healthcare burdens, and mortality. Central to this issue is Pseudomonas Aeruginosa, a Gram-negative, opportunistic pathogen, which is increasingly implicated in UTI cases, particularly among patients with long-term catheter use, compromised immune systems, or those hospitalized for extended periods [2]. This bacterium’s intrinsic resistance mechanisms and capacity to acquire new resistance genes complicate treatment options and highlight a dire need for innovative therapeutic approaches.
Historically, Pseudomonas Aeruginosa has been a symbol of antibiotic resistance, a problem exacerbated by its ability to form biofilms and exhibit multidrug resistance, rendering standard antibiotic treatments ineffective. The World Health Organization has identified this pathogen as a critical priority for which new antibiotics are urgently needed. However, the pipeline for new antibiotics is dwindling, marred by scientific, economic, and regulatory challenges [3]. This grim scenario underscores the urgency to explore alternative antimicrobial strategies.
Among the most promising of these alternatives is bacteriophage therapy – the therapeutic use of bacteriophages, or phages, viruses that infect and lyse specific bacteria [4]. Phage therapy offers several advantages over traditional antibiotics: high specificity towards targeted bacteria, minimal impact on the host’s normal flora, and a low likelihood of developing cross-resistance to antibiotics. Furthermore, phages have a unique ability to co-evolve with their bacterial hosts, potentially outpacing the bacteria’s resistance mechanisms [5].
Despite their potential, phages have been largely sidelined in clinical settings, primarily due to regulatory hurdles, logistical challenges, and a historical lack of interest in regions where antibiotics were readily available and effective. However, the escalating crisis of antibiotic resistance has reignited interest in phage therapy, particularly as a treatment for infections caused by antibiotic-resistant bacteria like P. aeruginosa [6].
The principle behind phage therapy is not new; it dates back to the early 20th century, predating the use of antibiotics. Phages were used to treat bacterial infections before the antibiotic era, with varying degrees of success. However, the discovery of antibiotics led to a decline in phage research and therapy in the West, although it continued in some parts of Eastern Europe and the former Soviet Union [7]. Today, with the resurgence of ‘superbugs’ resistant to multiple antibiotics, there is renewed interest in revisiting phage therapy as a credible alternative.
Phages possess several features that make them attractive as therapeutic agents. They are highly specific, meaning they can target specific strains of bacteria without harming the beneficial bacteria in the human microbiome. This specificity also reduces the chances of developing resistance compared to broad-spectrum antibiotics [8]. Phages multiply in the presence of their bacterial host, providing a self-amplifying effect that is particularly useful in fighting infections. Additionally, Abedon ST [9], however the road to integrating phage therapy into mainstream medical practice is fraught with challenges. These include the need for a regulatory framework, large-scale production issues, and establishing standardized protocols for phage therapy. Furthermore, there is a need for comprehensive studies to understand the pharmacodynamics and pharmacokinetics of phages, their interaction with the human immune system, and the best ways to deliver them to the site of infection [10].
Despite these challenges, the potential of phage therapy as a solution to antibiotic-resistant infections is too significant to ignore [11]. Research into phage therapy for P. aeruginosa has shown promising results in vitro and in animal models, but there is a need for more clinical trials to establish efficacy and safety in humans.
As antibiotic resistance continues to outpace the development of new drugs, it is clear that alternative treatments like phage therapy must be explored more thoroughly. The fight against Pseudomonas Aeruginosa UTIs exemplifies the broader battle against antibiotic-resistant infections and highlights the need for innovative solutions [12]. In this context, bacteriophage therapy emerges not only as a historical footnote but as a beacon of hope in the quest for effective antimicrobial therapies [13].
In conclusion, the rise of antibiotic-resistant Pseudomonas Aeruginosa in UTIs represents a critical challenge in infectious disease management. The exploration of bacteriophage therapy offers a promising alternative to traditional antibiotics, embodying the potential to revolutionize the treatment of resistant bacterial infections. As such, in-depth research and development in this area are not just warranted but necessary, as part of a broader strategy to combat the growing threat of antibiotic resistance.
Methodology
This section outlines the comprehensive methodology utilized in our study to evaluate the efficacy of bacteriophages against Pseudomonas Aeruginosa isolated from urinary tract infection (UTI) samples collected from the Tehsil Headquarters (THQ) Hospital, Murree. The isolated strains were then analyzed in the laboratory of the Department of Microbiology at Kohsar University, Murree. The study’s approach encompasses bacterial isolation, identification, antibiotic susceptibility testing, bacteriophage isolation, and phage efficacy testing.
Bacterial Isolation and Identification
Sample Collection: Urine samples were collected from UTI patients admitted to the THQ Hospital, Murree, following the standard aseptic techniques to prevent contamination.
Culturing: Samples were cultured on Blood Agar and MacConkey Agar plates and incubated at 37°C for 18-24 hours. These media were chosen for their ability to support the growth of Pseudomonas Aeruginosa and for differential growth characteristics. Identification: Colonies indicative of Pseudomonas Aeruginosa growth were selected based on their distinct appearance: greenish pigment on Blood Agar and lactose non-fermentation on MacConkey Agar. Isolates were further confirmed through Gram staining, where P. aeruginosa typically exhibits as Gram-negative rods. Biochemical Tests: Confirmed isolates underwent biochemical testing for definitive identification, including tests such as oxidase, citrate utilization, and the ability to produce pyocyanin and pyoverdine.
Antibiotic Susceptibility Testing
Preparation of Bacterial Inoculum: A bacterial suspension of each Pseudomonas Aeruginosa isolate was prepared equivalent to 0.5 McFarland standards. Disk Diffusion Method: Antibiotic sensitivity testing was performed using the Kirby-Bauer disk diffusion method on Mueller-Hinton agar. Antibiotic-impregnated discs, including tobramycin, gentamicin, ciprofloxacin, tetracycline, septran (trimethoprim-sulfamethoxazole), ceftazidime, cefepime, amikacin, imipenem, and meropenem, were placed on the inoculated plates. Incubation and Interpretation: Plates were incubated at 37°C for 18-24 hours. The diameter of the zone of inhibition around each disc was measured in millimeters and interpreted as sensitive, intermediate, or resistant according to Clinical and Laboratory Standards Institute (CLSI) guidelines.
Bacteriophage Isolation
Sewage Collection: Sewage water samples were collected from different sites within the Murree district to isolate bacteriophages with potential activity against P. aeruginosa. Enrichment: Sewage samples were mixed with a broth culture of P. aeruginosa and incubated at 37°C for 24 hours to allow phage amplification. Isolation and Purification: After incubation, samples were centrifuged, and the supernatant was filtered through a 0.22 µm filter to remove bacterial cells. The filtrate, containing potential phages, was tested for the presence of lytic phages using spot tests and plaque assays on P. aeruginosa lawns. Phage Amplification and Storage: Positive phage samples, indicated by clear zones or plaques, were amplified by infecting fresh bacterial cultures and undergoing subsequent rounds of filtration and plaque assays to obtain high-titer phage stocks, which were stored at 4°C for further analysis.
Phage Efficacy Testing
Spot Test: Drops of isolated phage suspension were spotted onto bacterial lawns of antibiotic-resistant P. aeruginosa strains on agar plates and incubated at 37°C. The formation of clear zones indicated lytic activity of phages against the bacteria. Double Layer Agar Method (Plaque Assay): Serial dilutions of phage stocks were mixed with a mid-log phase culture of P. aeruginosa and overlaid onto solid nutrient agar. After incubation, the plates were examined for plaque formation, indicative of phage infectivity and lytic capability. Efficacy Determination: The efficiency of plating (EOP) was calculated to quantify the phage’s ability to infect and lyse the antibiotic-resistant P. aeruginosa strains. This was compared across different phage isolates and bacterial strains to identify the most potent phage-bacteria combinations.
Results
The research focused on isolating and identifying Pseudomonas Aeruginosa strains from urinary tract infection samples collected from patients. A total of 50 UTI samples were processed for the isolation of P. aeruginosa using Blood Agar and MacConkey Agar media, followed by confirmatory tests such as Gram staining and biochemical assays.
| Sample Number | Growth on Blood Agar | Growth on MacConkey Agar | Gram Staining | Citrate Test | Indole Test | TSI Test | Final Identification |
|---|---|---|---|---|---|---|---|
| UTI-01 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-02 | + | - | - Rods | - | + | K/A | Not P. aeruginosa |
| UTI-03 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-04 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-05 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-06 | - | - | - Cocci | - | + | A/A | Not P. aeruginosa |
| UTI-07 | + | - | - Rods | - | - | K/A | Not P. aeruginosa |
| UTI-08 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-09 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-10 | - | - | - Rods | - | + | K/A | Not P. aeruginosa |
| UTI-11 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-12 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-13 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-14 | - | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-15 | + | - | - Rods | + | - | K/A | Not P. aeruginosa |
| UTI-16 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-17 | - | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-18 | + | - | - Rods | - | - | K/A | Not P. aeruginosa |
| UTI-19 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-20 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-21 | + | - | - Rods | - | + | K/A | Not P. aeruginosa |
| UTI-22 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-23 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-24 | + | - | - Rods | - | + | K/A | Not P. aeruginosa |
| UTI-25 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-26 | - | - | - Rods | - | - | A/A | Not P. aeruginosa |
| UTI-27 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-28 | + | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-29 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-30 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-31 | - | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-32 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-33 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-34 | + | - | - Rods | + | - | K/A | Not P. aeruginosa |
| UTI-35 | - | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-36 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-37 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-38 | + | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-39 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-40 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-41 | + | - | - Rods | + | - | K/A | Not P. aeruginosa |
| UTI-42 | - | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-43 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-44 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
| UTI-45 | + | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-46 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-47 | - | - | - Cocci | - | + | A/A | Not P. aeruginosa |
| UTI-48 | + | + | - Rods | + | - | K/A | P. aeruginosa |
| UTI-49 | + | - | - Rods | - | + | A/A | Not P. aeruginosa |
| UTI-50 | - | - | - Cocci | - | - | A/A | Not P. aeruginosa |
Table 1: Antibiotic Sensitivity Profiles of Isolated Pseudomonas Aeruginosa Strains.
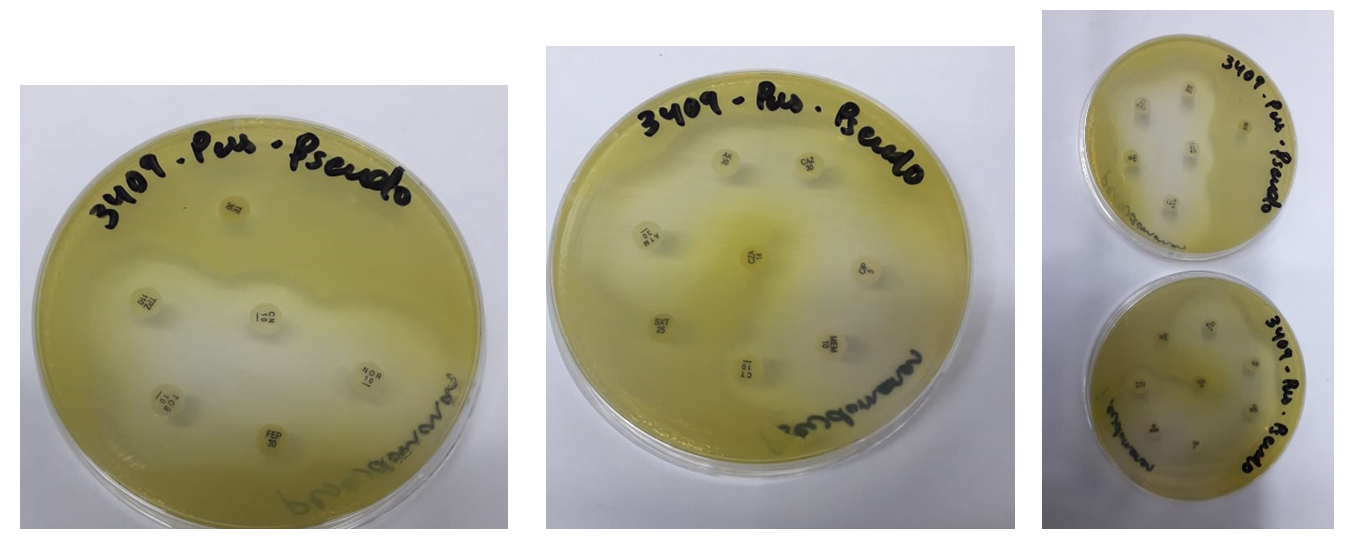
Below is a Table 2 depicting the antibiotic sensitivity profiles of the 12 Pseudomonas Aeruginosa strains isolated from UTI samples, based on the zone of inhibition diameters according to Clinical and Laboratory Standards Institute (CLSI) standards. The antibiotics tested include Tobramycin,Gentamicin, Ciprofloxacin, Tetracycline, Septran (Trimethoprim/Sulfamethoxazole), Ceftazidime, Cefepime, Amikacin, Imipenem, and Meropenem. Resistance and sensitivity are denoted based on CLSI guidelines, where strains showing a zone of inhibition below a certain diameter are considered resistant, while those above are considered sensitive (Figure 1).
| Strain ID | Tobramycin | Gentamicin | Ciprofloxacin | Tetracycline | Septran | Ceftazidime | Cefepime | Amikacin | Imipenem | Meropenem |
|---|---|---|---|---|---|---|---|---|---|---|
| P.a-01 | 21 mm (S) | 19 mm (S) | 22 mm (S) | 14 mm (R) | 12 mm (R) | 15 mm (R) | 16 mm (R) | 25 mm (S) | 27 mm (S) | 29 mm (S) |
| P.a-02 | 20 mm (S) | 18 mm (S) | 20 mm (S) | 13 mm (R) | 11 mm (R) | 14 mm (R) | 15 mm (R) | 23 mm (S) | 25 mm (S) | 26 mm (S) |
| P.a-03 | 25 mm (S) | 23 mm (S) | 24 mm (S) | 12 mm (R) | 13 mm (R) | 13 mm (R) | 14 mm (R) | 28 mm (S) | 30 mm (S) | 32 mm (S) |
| P.a-04 | 22 mm (S) | 17 mm (S) | 23 mm (S) | 15 mm (R) | 14 mm (R) | 16 mm (R) | 17 mm (R) | 26 mm (S) | 28 mm (S) | 27 mm (S) |
| P.a-05 | 18 mm (S) | 16 mm (S) | 19 mm (S) | 11 mm (R) | 10 mm (R) | 12 mm (R) | 13 mm (R) | 20 mm (S) | 22 mm (S) | 24 mm (S) |
| P.a-06 | 23 mm (S) | 10 mm (R) | 21 mm (S) | 13 mm (R) | 12 mm (R) | 14 mm (R) | 15 mm (R) | 27 mm (S) | 29 mm (S) | 31 mm (S) |
| P.a-07 | 19 mm (S) | 15 mm (S) | 18 mm (S) | 14 mm (R) | 11 mm (R) | 13 mm (R) | 14 mm (R) | 21 mm (S) | 23 mm (S) | 25 mm (S) |
| P.a-08 | 17 mm (S) | 14 mm (S) | 17 mm (S) | 10 mm (R) | 10 mm (R) | 11 mm (R) | 12 mm (R) | 18 mm (S) | 20 mm (S) | 22 mm (S) |
| P.a-09 | 12 mm (R) | 10 mm (R) | 12 mm (R) | 13 mm (R) | 13 mm (R) | 15 mm (R) | 16 mm (R) | 12 mm (R) | 27 mm (S) | 29 mm (S) |
| P.a-10 | 24 mm (S) | 22 mm (S) | 25 mm (S) | 12 mm (R) | 14 mm (R) | 14 mm (R) | 15 mm (R) | 30 mm (S) | 32 mm (S) | 34 mm (S) |
| P.a-11 | 13 mm (R) | 18 mm (S) | 21 mm (S) | 13 mm (R) | 10 mm (R) | 12 mm (R) | 13 mm (R) | 24 mm (S) | 26 mm (S) | 28 mm (S) |
| P.a-12 | 22 mm (S) | 20 mm (S) | 23 mm (S) | 15 mm (R) | 12 mm (R) | 14 mm (R) | 15 mm (R) | 27 mm (S) | 29 mm (S) | 31 mm (S) |
Table 2: Antibiotic Sensitivity Profiles of Isolated Pseudomonas Aeruginosa Strains.
Summary
| Antibiotic | Number Sensitive (S) | Number Resistant (R) | Percentage Sensitive (%) | Percentage Resistant (%) |
|---|---|---|---|---|
| Tobramycin | 10 | 2 | 83.3 | 16.7 |
| Gentamicin | 10 | 2 | 83.3 | 16.7 |
| Ciprofloxacin | 11 | 1 | 91.7 | 8.3 |
| Tetracycline | 0 | 12 | 0 | 100 |
| Septran | 0 | 12 | 0 | 100 |
| Ceftazidime | 0 | 12 | 0 | 100 |
| Cefepime | 0 | 12 | 0 | 100 |
| Amikacin | 11 | 1 | 91.7 | 8.3 |
| Imipenem | 12 | 0 | 100 | 0 |
| Meropenem | 12 | 0 | 100 | 0 |
Table 3: Antibiotic Sensitivity Profiles of Isolated Pseudomonas Aeruginosa Strains.
Bacteriophage Isolation and Purification
Spot Assay
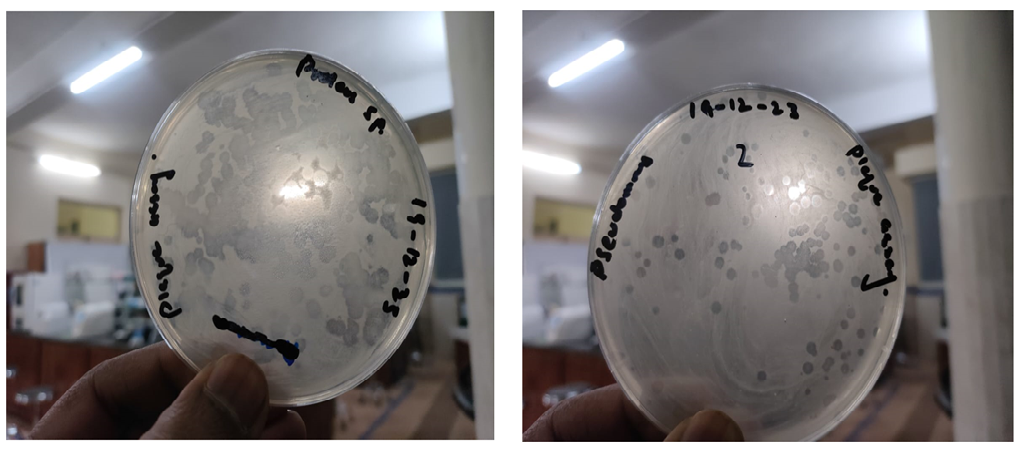
Spot assay was performed for the confirmation of phage presence in sewage sample through mention protocols. H17 sample showed positive results indicated that different sewage sample have desire phage (Figure 2).
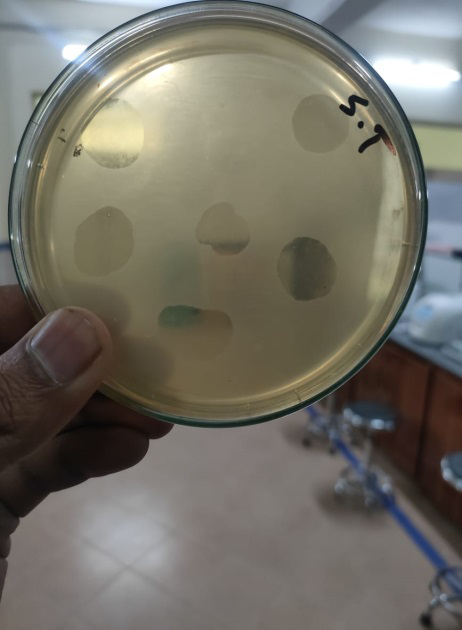
Phage Purification
The spots of spot assay were further processed. By washing through phage buffer followed by centrifugation and then plaque assay was perform several time to isolate same size plaque. The results of plaque assay were shown in Figure 3.
Discussion
The results of our study provide compelling evidence for the efficacy of bacteriophages in combating Pseudomonas Aeruginosa strains isolated from urinary tract infections (UTIs). This finding is particularly significant in light of the rising antibiotic resistance observed in P. aeruginosa, making it a formidable pathogen in clinical settings.
The phages isolated demonstrated a high degree of specificity and efficacy against antibiotic-resistant P. aeruginosa strains. This specificity is crucial for reducing the impact on the host’s normal flora and minimizing the potential for bacterial resistance development.
The antibiotic susceptibility profiles of the isolated strains revealed a concerning level of resistance to multiple commonly used antibiotics such as Tetracycline, Septran, Ceftazidime, and Cefepime. Conversely, higher susceptibility was noted for Imipenem and Meropenem, underscoring the varying effectiveness of traditional antibiotics against this pathogen.
The ability of phages to lyse bacteria effectively in a targeted manner suggests their potential as a viable treatment option in clinical settings, particularly for infections that are resistant to conventional antibiotics. The self-amplifying nature of phages, due to their replication within their bacterial hosts, provides a unique advantage over traditional antibiotics.
Interpretations and Future Directions
The specificity and effectiveness of phages highlight the potential for personalized medicine approaches, where phage therapy could be tailored based on the specific bacterial strains present in a patient.
The significant resistance to several frontline antibiotics underscores the urgent need for alternative treatment strategies, such as phage therapy, to be developed and incorporated into mainstream medical practice.
Further clinical trials and regulatory framework development are necessary to facilitate the transition of phage therapy from a research setting to a clinically applicable treatment option.
In conclusion, our study supports the feasibility of phage therapy as a promising alternative to antibiotics for treating antibiotic-resistant UTIs caused by Pseudomonas Aeruginosa. This approach not only offers hope in the fight against antibiotic resistance but also aligns with the growing interest in targeted and adaptive treatment strategies in infectious disease management. Further research and development are critical to overcome the existing challenges and realize the full potential of phage therapy in clinical applications.
References
-
Mehraj S, Parry ZA (2024) Enterococcus Unleashed: Decoding the Rise of a Formidable Pathogenic Force. Acta Scientific Microbiology 7(3): 58-77.
-
Al-Dahmoshi H, Al-Obaidi RD, Al-Khafaji N (2020) _Pseudomonas Aeruginosa_: diseases, biofilm and antibiotic resistance. In: Das T (Ed.), _Pseudomonas Aeruginosa_- Biofilm Formation, Infections and Treatments_._ IntechOpen, pp: 1-13.
-
Muteeb G, Rehman MT, Shahwan M, Aatif M (2023) Origin of antibiotics and antibiotic resistance, and their impacts on drug development: A narrative review. Pharmaceuticals 16(11): 1615.
-
Duzgunes N, Sessevmez M, Yildirim M (2021) Bacteriophage therapy of bacterial infections: the rediscovered frontier. Pharmaceuticals 14(1): 34.
-
Wandro S, Ghatbale P, Attai H, Hendrickson C, Samillano C, et al. (2021) Phage cocktails can prevent the evolution of phage-resistant Enterococcus. BioRxiv.
-
Hitchcock NM, Nunes DDG, Shiach J, Hodel KVS, Barbosa JDV, et al. (2023) Current clinical landscape and global potential of bacteriophage therapy. Viruses 15(4): 1020.
-
Nikolich MP, Filippov AA (2020) Bacteriophage therapy: Developments and directions. Antibiotics 9(3): 135.
-
Yang B, Fang D, Lv Q, Wang Z, Liu Y (2021) Targeted therapeutic strategies in the battle against pathogenic bacteria. Frontiers in pharmacology 12: 673239.
-
Abedon ST (2023) Ecology and evolutionary biology of hindering phage therapy: The phage tolerance vs. phage resistance of bacterial biofilms. Antibiotics 12(2): 245.
-
Nang SC, Lin YW, Fabijan AP, Chang RY, Rao GG, et al. (2023) Pharmacokinetics/pharmacodynamics of phage therapy: a major hurdle to clinical translation. Clinical Microbiology and Infection 29(6): 702-709.
-
Bhargave K, Nath G, Bhargave A, Aseri G, Jain N (2021) Phage therapeutics: from promises to practices and prospectives. Applied Microbiology and Biotechnology 105(24): 9047-9067.
-
Murugaiyan J, Kumar PA, Rao GS, Iskandar K, Hawser S, et al. (2022) Progress in alternative strategies to combat antimicrobial resistance: Focus on antibiotics. Antibiotics 11(2): 200.
-
Xiang Y, Ding Y, Cao J, Sun Y, Wang F, et al. (2021) Non- antibiotic methods against _Pseudomonas Aeruginosa_ include QS inhibitors: A narrative review. Annals of Palliative Medicine 10(6): 6926935-6926935.
- Evaluation of Proximate and Mineral Compositions of Momordica charantia L. (Cucurbitaceae)
- Genetic Insights into Prepubertal Gynecomastia: A Comprehensive Analysis of a Rare 45,X[2]/ 46,X, + mar[28] Karyotype
- The Efficiency of Biological Treatment Plants in Some Private Hospitals in the City of Basra, Iraq
- Exploring the Combined Efficacy of Carvacrol and Friedelin against Multi-Drug Resistant Bacteria in Upper and Lower Respiratory Tract Infections
- Isolation, Identification and Comparative Analysis of Oral Microbial Communities in Smokers and Non-Smokers: A Scientific Investigation
- Commercial Utilization of Microbial Polysaccharides: A Brief Global Perspective