Genetic Insights into Prepubertal Gynecomastia: A Comprehensive Analysis of a Rare 45,X[2]/ 46,X, + mar[28] Karyotype
Introduction: This case study delves into the genetic underpinnings of prepubertal gynecomastia by conducting an exhaustive analysis of a rare 45,X[2]/46,X,+mar[28] karyotype. Enlargement of male breast tissue, known as Gynecomastia, is generally considered a natural occurrence during adolescence but requires comprehensive assessment in severe cases. Prepubertal gynecomastia is exceedingly uncommon, and the sparse literature results in a lack of comprehensive understanding regarding its causes and management. Case Presentation: This study focuses on a male child aged eight years and six months who presented with bilateral gynecomastia before reaching puberty and also had short stature. The analysis of the patient's karyotype unveiled an unusual chromosomal arrangement of 45,X[2]/46,X,+mar[28], with the extra marker chromosome stemming from the Y chromosome, revealing Yq microdeletions. The clinical evolution, chromosomal examination, and molecular discoveries concerning the patient are detailed, emphasizing the pivotal importance of karyotyping in instances of prepubertal gynecomastia. Conclusion: Karyotyping plays a pivotal role in identifying potential chromosomal anomalies contributing to prepubertal gynecomastia. Specifically, cases involving Yq deletion warrant vigilant monitoring, particularly concerning short stature.
Introduction
Gynecomastia denotes the enlargement of breast tissue in males, manifesting either unilaterally or bilaterally. While pubertal gynecomastia is typically bilateral and considered a normal physiological occurrence in most cases, instances, where breast enlargement exceeds grade 3, necessitate thorough endocrine and oncologic evaluation to rule out underlying pathological conditions. In contrast to pubertal gynecomastia, prepubertal gynecomastia is a rarity in medical literature, with only a few documented case reports available, resulting in a scarcity of data regarding its etiology and management strategies [1–3].
The age distribution of gynecomastia exhibits three distinct peaks. The first peak occurs during the neonatal period, affecting 60% to 90% of newborns, and is attributed to the transfer of estrogens across the placenta. The second peak occurs during puberty, characterized by a hormonal imbalance between androgens and estrogens in breast tissue. The final peak is observed in the adult male population, particularly prevalent among males aged 50 to 80 [2]. In contrast to gynecomastia in adolescents and adults, prepubertal gynecomastia is uncommon and often categorized as idiopathic, with a specific etiology rarely identified. Thus, further research into its underlying causes is warranted, particularly to mitigate potential endocrine or neoplastic concerns. Gynecomastia can result from various endocrinopathies, primarily stemming from an elevation in the ratio of circulating estrogens to androgens [3].
Herein, we present an uncommon instance of a young male diagnosed with prepubertal bilateral gynecomastia and diminished stature. The individual exhibits a karyotype of 45,X[2]/46,X,+mar[28]. Intriguingly, analysis revealed that the additional marker chromosome stemmed from the Y chromosome, unveiling Yq microdeletions
Case Presentation
An eight-and-a-half-year-old male child was admitted to the endocrinology department upon the onset of pubic hair development. He measured 128.2 cm tall, placing him within the 25-50 percentile range, with his weight percentage at an optimal 111%. Upon initial examination, his testicular volume was recorded at 2 ml/2 ml, and his pubic hair was classified as Tanner III, with no axillary hair observed. The first set of laboratory tests revealed his TSH levels at 3.12 mU/L, sT4 at 1.21 ng/dL, total testosterone at 0.14 ng/dL, DHEAS at 70 µg/dL, 11-deoxycorticosterone (11DOC) at 2.7 ng/dL, 17-hydroxy progesterone (17 OHP) at 0.98 ng/dL, cortisol at 24.4, and adrenocorticotropic hormone (ACTH) at 23.9 pg/mL.
Over the subsequent 12 years and 11 months of monitoring, the patient exhibited weight gain and a decline in height percentile, measuring 146.2 cm tall (3-10 percentile; -1.46 standard deviations) with an ideal weight percentage of 138%. His growth rate was noted at 3.2 cm/year. Further examination revealed that his testicular volume remained stable at 2 ml/2 ml, his pubic hair advanced to Tanner IV, and bilateral gynecomastia emerged (right breast Tanner II, left breast Tanner II). Lab results indicated alpha-fetoprotein (AFP) levels below 1.7 ng/mL, estradiol (E2) levels below 11.8 ng/dL, beta-hCG levels below 2, prolactin at 21.9 ng/mL, follicle-stimulating hormone (FSH) at 1.26 IU/L, luteinizing hormone (LH) at 0.36 IU/L, total testosterone at 17.11 ng/ dL, DHEAS at 135 µg/dL, 11 DOC at 0.58 ng/dL, 17OHP at 0.69 ng/dL, TSH at 2.4 mU/L, sT4 at 1.19 ng/dL, cortisol at 30.9, and ACTH at 7.12 pg/mL. Breast ultrasound revealed fibroglandular tissue measuring 38x15 mm on the left and 15x4 mm on the right. Chromosome analysis was conducted due to the presence of prepubertal gynecomastia.
Chromosomal Analysis
Upon completing the Fluorescence In Situ Hybridization (FISH) analysis, it was revealed that a small fraction of the interphases, specifically 5 out of 50, exhibited a distinctive pattern of genetic signals, characterized by DXZ1 x 1, Yp11.31 x 0, and DYZ1 x 0. Conversely, the majority of interphases, totaling 45 out of 50, displayed a different signal pattern, showing DXZ1 x 1, Yp11.31 x 1, and DYZ1 x 0. Intriguingly, none of the analyzed cells exhibited a signal for the Yq11.31 region, indicating a notable genetic anomaly.
Moreover, subsequent family screening yielded normal results, suggesting that the observed genetic aberration was unique to the individual and not inherited from familial genetic predispositions. Delving deeper into the molecular examination of the Y chromosome, deletions were identified in the AZFb and AZFc regions, further complicating the genetic landscape.
As a result of these findings, an extensive chromosomal analysis was conducted to unravel the intricate genetic composition. The karyotype was ultimately identified as 45,X[2]/46,X,+der(Y)del(Y)(q11.22q11.23)[28], providing crucial insights into the genetic makeup of the individual. This comprehensive analysis, depicted in Figure 1, sheds light on the intricate genetic variations underlying the observed phenotype and underscores the importance of molecular techniques in deciphering complex chromosomal abnormalities.
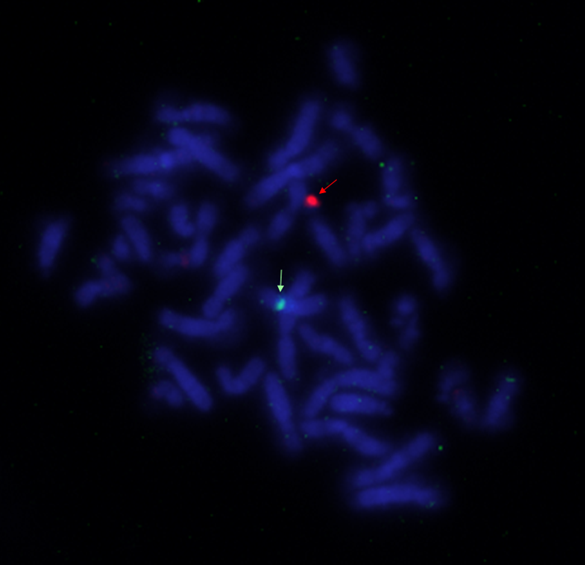
The identification of the +mar[28] anomaly on chromosome 45,X[2] was achieved through examination under a fluorescence microscope following the Fluorescence In Situ Hybridization (FISH) technique.
The identification of the +mar[28] anomaly on chromosome 46,X was accomplished through observation under a fluorescence microscope subsequent to employing the Fluorescence In Situ Hybridization (FISH) technique.
At the final follow-up appointment, conducted when the patient reached 14 years and 2 months of age, his stature was measured at 153 cm, placing him within the 3-10 percentile range, with a corresponding standard deviation of -1.54. Despite this, his weight was found to be optimal, representing 121% of the expected value for his age and height. Upon physical examination, the patient’s testicular volume was noted to be 8 ml/8 ml, indicative of normal development, while his pubic hair had progressed to Tanner stage IV, signifying advanced pubertal maturation. Additionally, bilateral gynecomastia was observed, with the right breast classified as Tanner stage III and the left breast also at Tanner stage III.
Laboratory investigations, as detailed in Table 1, revealed lower-than-expected growth hormone levels in response to Growth Hormone Provocation tests. Specifically, the L-DOPA peak growth hormone value was recorded at 2.76 ng/mL, and the clonidine peak growth hormone value was slightly higher at 3.08 ng/mL. In light of these findings, the medical team recommended the initiation of growth hormone (GH) treatment to address the observed deficiency and promote optimal growth and development. This decision underscores the importance of proactive intervention to address endocrine imbalances and ensure the patient’s overall well- being and future health outcomes.
| 8 Years 6 Months | 12 Years 11 Months | 14 Years 2 Months | Normal Range | |
|---|---|---|---|---|
| FSH (IU/L) | 1.26 | 1.59 | 1.2-19.2 | |
| LH(IU/L) | 0.36 | 2.84 | 1.24-8.62 | |
| Estradiol (pg/mL) | <11,8 | <10 | ||
| Testosterone (ng/mL) | 0.14 | 17.11 | 134.6 | <0.2 |
| ACTH(pg/mL) | 23.9 | 7.12 | 7.08 | |
| Cortisol(μg/ dL) | 24.4 | 30.9 | 16 | 6.7-22.6 |
| Prolactin(ng/mL) | 21.9 | 16.68 | 4.79-23.3 | |
| FT4(ng/dL) | 1.21 | 1.19 | 0.92 | 0.6-1.12 |
| TSH (mU/L) | 3.12 | 2.4 | 1.46 | 0.5-5 |
| Alfa-fetoprotein (ng/mL) | <1,7 | 0.5-5.5 | ||
| BetaHcg (mIU/mL) | <2 | <2 | ||
| 170HP (ng/mL) | 0.98 | 0.69 | 0-0.63 | |
| 11DOC (ng/dL) | 2.72 | 0.58 | 0-3.44 | |
| DHEAS(μg/ dL) | 70.5 | 135 | 80-560 | |
| SHBG(nmol/L) | 22.9 | Oct-57 | ||
| IGF-BP3(μg/ mL) | 5.3 | |||
| Somatomedin-C (ng/mL) | 311 | |||
| L-DOPA peak GH (ng/mL) | 2.76 | |||
| Clonidine peak GH (ng/mL) | 3.08 |
Table 1: Hormonal evaluation of the patient.
Discussion
In this unique case, the male genetic blueprint 46,X,+mar showcases an uncommon irregularity wherein the testes lack the usual structural Y chromosome in their non-mosaic genetic makeup. A genetic anomaly that defies detection through conventional cytogenetic karyotype analysis is referred to as a marker chromosome (mar). The importance of a marker chromosome lies in its intact genetic material and information. Deletions in the Yq region carry implications for growth patterns, skeletal development, spermatogenesis, and fertility. Thus, the utilization of cytogenetic molecular techniques becomes imperative to unravel the genetic and clinical attributes of the marker chromosome [4, 5, 6].
Increased aromatase activity in adipose tissue among obese individuals can lead to the conversion of androgens into estrogens, potentially triggering the development of gynecomastia [2]. Einav-Bachar and colleagues discovered that 31% of individuals diagnosed with prepubertal gynecomastia exhibited obesity [1]. Prepubertal gynecomastia in young individuals can arise from contact with drugs and chemical compounds possessing estrogenic or antiandrogenic attributes, whether through systemic, autocrine, or paracrine means. This excludes systemic ailments like tumors that produce estrogen or androgen, liver malfunction, hyperthyroidism, and others, which can either elevate estrogen synthesis or impede its breakdown [2, 7, 8].
Felner and White observed three prepubertal boys who developed bilateral gynecomastia as a consequence of their mothers’ application of topical estrogen cream, acting as an indirect means of estrogen exposure [9]. In all three patients, gynecomastia resurfaced after their mothers discontinued the use of the lotion. Likewise, Henley and colleagues documented three prepubertal boys who experienced bilateral gynecomastia subsequent to the application of lavender oil [7]. The condition ameliorated following cessation of the triggering substance. In our investigation, the participant had no prior contact with chemicals or any record of systemic illness.
Usually, teenagers aged 13 or 14 are susceptible to encountering pubertal gynecomastia, marked by either unilateral or bilateral, temporarily discomforting, resilient, or solid masses confined to a specific region. The majority of patients witness a reappearance within one to two years. As per findings from a cohort investigation, an endocrine assessment should be entertained if the ailment persists beyond two years and displays significant severity, escalating to grade B3 [10]. Increased aromatase function, tumors in the adrenal or testicular areas, partial insensitivity to androgens, and conditions linked to disorders in sex differentiation (DSD), such as 46,XX testicular (SRY+)-related hypogonadism, and Klinefelter syndrome, are some of the elements that contribute to enduring and notable instances of gynecomastia [11]. Hence, chromosomal analysis was performed in this particular case due to clinical indications suggestive of DSD.
Intriguingly, the karyotype unveiled 45,X[2]/46,X, +mar[28]. Fluorescence In Situ Hybridization (FISH) assessment revealed nucish (DXZ1 x 1, Yp11.31 x 0, DYZ1 x 0)[5/50] / (DXZ1 x 1, Yp11.31 x 1, DYZ1 x 0)[45/50]. Signals originating from the DXZ1 and SRY regions were identified in 45 out of 50 interphase nuclei, while no signal was observed with the probe targeting the Yq11.31 region in these cells. In the remaining 5 cells, a solitary signal from the DXZ1 region was detected.
The current case, characterized by 46,X,+mar, presents with obesity and short stature, aligning with similar clinical manifestations documented in previous studies (Table 2). It is noteworthy that 46,X,del(Yq) is associated with concurrent conditions such as gynecomastia, diminished stature, intellectual disability, as well as spermatogenic maturation arrest, small testes with testicular lesions, sertoli cell- only syndrome, tubular hyalinization, and spermatogenic maturation arrest [12].
| Age | Karyotype | Comorbidities | Conclusion | |
|---|---|---|---|---|
| Hayashi et al. | 1 yr | 46,X,+mar | Abnormal external genitalia, hypospadias | SRY+, 46,X,der(9p) |
| Calzolari et al. | 11 yr | 46,X,+mar | Obesity, short stature(<10p),bilateral cryptorchidism, coarctation of the aorta | SRY+, 46,X,del(Y)(p11.3-q11.21) |
| Graham and Bacino | 10yr 10 months | 46,X,+mar | Short stature(<5p), developmental delay, bilateral cryptorchidism, bilateral hearing loss, webbed neck, low posterior hairline, mild brachydactyly, short 4th,and 5th metatarsals, murmur | SRY+, 46,X,der(Y)del(Y)(p11.23) del(Y) (q11.23) |
| Ki Eun Kim et al. | 15 yr | 46,X,+mar | Short stature, mild intellectual disability, a small fallus, , a knuckle-dimple sign, the fourth toe of left foot, short 4th and 5th metacarpal and 4th metatrsal bones | 46,X,der(Y)del(Y)(q11.21q11.222) del(Y) (q11.23qter) |
| Presenting case | 12 yr, 11 mo | 45,X[2]/46,X,+mar[28] | Short stature, prepubertal bilateral gynecomastia | 45,X[2]/46,X,+der(Y)del(Y) (q11.22q11.23)[28] |
Table 2: Summary of previos reports of non-mosaic 46,X,+mar in boys.
Short stature has been linked to the Yq11 region, renowned for its anti-Turner effect, regulating growth control, tooth development, and fertility, particularly via Y-specific growth control regions [13]. Intriguingly, in certain instances, microdeletions of the Yq chromosome have been associated with various combinations of phenotypes, including cubitus valgus, diminished height, a webbed neck, shorter fourth and fifth metacarpals, pigmented nevi, a low posterior hairline, and gynecomastia [5, 6].
Conclusion
In summary, karyotyping serves as a crucial component in assessing prepubertal gynecomastia. Furthermore, when conventional banding methodologies reveal a marker chromosome instead of the typical sex chromosome, comprehensive endocrine evaluations, integrating cytogenetic and DNA molecular analyses, become essential. These assessments are conducted to validate the existence of a sex chromosome or SRY and to identify any structural irregularities or breakpoints within the marker chromosome.
Declarations
Acknowledgements
None
Funding
None
Conflict of interest
The authors declare no conflicts of interest.
Patient consent statement
Consent for the inclusion of this patient and their family in this report has been obtained.
Ethical Approval
Not applicable
Availability of data
Data can be requested directly from the authors.
References
-
Einav-Bachar R, Phillip M, Aurbach-Klipper Y, Lazar L (2004) Prepubertal gynaecomastia: aetiology, course and outcome. Clin Endocrinol 61(1): 55-60.
-
Binder G, Iliev DI, Dufke A, Wabitsch M, Schweizer R, et al. (2005) Dominant transmission of prepubertal gynecomastia due to serum estrone excess: hormonal, biochemical, and genetic analysis in a large kindred. J Clin Endocrinol Metab 90(1): 484-492.
-
Hoevenaren IA, Schott DA, Otten BJ, Kroese-Deutman HC (2011) Prepubertal unilateral gynecomastia: a report of two cases. Eur J Plast Surg 34: 395-398.
-
Hayashi Y, Tsugaya M, Sasaki S, Mogami T, Tozawa K, et al. (1996) Detection of sex-determining region in a male with chromosomal abnormality (46,X+mar) and hypospadias. Urol Int 56(2): 122-124.
-
Calzolari E, Patracchini P, Palazzi P, Aiello V, Ferlini A (1993) Characterization of a deleted Y chromosome in a male with Turner stigmata. Clin Genet 43(1): 16-22.
-
Graham BH, Bacino CA (2003) Male patient with non- mosaic deleted Y-chromosome and clinical features of Turner syndrome. Am J Med Genet A 119A92): 234-237.
-
Henley DV, Lipson N, Korach KS, Bloch CA (2007) Prepubertal gynecomastia linked to lavender and tea tree oils. N Engl J Med 356(5): 479-485.
-
Edidin DV, Levitsky LL (1982) Prepubertal gynecomastia associated with estrogen-containing hair cream. Am J Dis Child 136(7): 587-588.
-
Felner EI, White PC (2000) Prepubertal gynecomastia: indirect exposure to estrogen cream. Pediatrics 105(4): e55.
-
Paris F, Gaspari L, Mbou F, Philibert P, Audran F, et al. (2016) Endocrine and molecular investigations in a cohort of 25 adolescent males with prominent/ persistent pubertal gynecomastia. Andrology 4: 263- 269.
-
Kim MS, Hwang PH, Lee D-Y (2015) A 46,XX Male Adolescent Presenting with a Chief Complaint of Gynecomastia. Pediatr Neonatol 56(5): 357-359.
-
Kim KE, Kim YJ, Jung MK, Chae H-W, Kwon AR, et al. (2017) A boy with 46,X,+mar presenting gynecomastia and short stature. Ann Pediatr Endocrinol Metab 22(4): 266-271.
-
Kirsch S, Weiss B, Rosa MD, Ogata T, Lombardi G, et al. (2000) FISH deletion mapping defines a single location for the Y chromosome stature gene, GCY. J Med Genet 37(8): 593-599.
- Evaluation of Proximate and Mineral Compositions of Momordica charantia L. (Cucurbitaceae)
- Targeting Superbugs: Efficacy of Bacteriophage Therapy against Antibiotic-Resistant Pseudomonas Aeruginosa in Urinary Tract Infections
- The Efficiency of Biological Treatment Plants in Some Private Hospitals in the City of Basra, Iraq
- Exploring the Combined Efficacy of Carvacrol and Friedelin against Multi-Drug Resistant Bacteria in Upper and Lower Respiratory Tract Infections
- Isolation, Identification and Comparative Analysis of Oral Microbial Communities in Smokers and Non-Smokers: A Scientific Investigation
- Commercial Utilization of Microbial Polysaccharides: A Brief Global Perspective