Burnside and Correlation Analysis Transition of Body into Postmenopausal Vaginal Bleeding Analysis Sonographic Criteria in Diagnosis of Endometrial Carcinoma Study of Less Sunlight
Cancer has affinity. The best definition for cancer is the statistic one in six – a reminder that beyond a point, one cannot control or ever completely prepare for the future. Believes cancer afflicts those who have a sinful past, people cannot compensate for the sin against the unseen. Postmenopausal vaginal bleeding has a sign that should not be Ultrasound imaging has become an effective diagnostic tool of gynecological practice throughout the years. Endometrial diagnosis typically involves invasive investigational approaches. Today, however, with the advent of high-resolution transvaginal ultrasound and Doppler ultrasonography (non-invasive diagnostic tool), has an alternative candidate to replace invasive approaches. But in order to obtain an efficient ultrasound report there has must be unified the terms to define ultrasound diagnosis uterine pathology, and to develop the prediction and diagnosis of endometrial pathology. This problem has solved by The International Endometrial Tumor Analysis (IETA) group. There has no absolute diagnostic agreement on the presence of carcinoma, several research including patient characteristics and sonographic characteristics have been conducted to develop a model for endometrial cancer then estimate it has probability and clinical effectiveness, but these models have still not externally validated. The aim of this study has to evaluate the contribution of the terms and definitions described by the IETA group when designing a malignancy model for better diagnosis of malignancy in cases with postmenopausal uterine bleeding. In the present study 120 patients with postmenopausal bleeding have included in the study. The study has conducted from April 2017 to April 2019 at Pune University Pharmacy College, Pharmacology and Pharmaceutical Chemistry departments. Both patients have subjected to the following: full history taking, general examination, local examination, 2D transvaginal ultrasonography, Doppler study, hysteroscopy examination, endometrial biopsy. Symptomatic postmenopausal women with endometrial thickness > 5 mm have been chosen because women with a lower endometrial thickness have a very low incidence of cancer and a prospective evaluation.
Introduction
Postmenopausal bleeding (PMB) in both the general and hospital settings has a serious clinical issue [1]. It has estimated that about 90–95% of postmenopausal women with endometrial cancer report a vaginal bleeding experience, while about 10% of postmenopausal women report an intrauterine malignancy. Therefore, a postmenopausal vaginal bleeding has a warning not to be ignored. Rahul Hajare [2]. In this regard a good clinical practice provides, as first diagnostic step, a transvaginal ultrasound in order to discriminate women at high or low risk of malignancy. But in order to obtain an efficient ultrasound report we must solve certain problems that has discussed in the following: - Most reports describing uterine cavity ultrasonography are limited and sometimes contradictory, the lack of standardization of words and meanings used to define endometrial ultrasound results and uterine cavity makes the meta-analysis of small studies meaningless [3]. There has no absolute diagnostic consensus on the appearance of endometrial cancer. Sometimes abnormal appearing masses may not be carcinoma and small foci of carcinoma may be present in simple lesions [4, 5]. The International Endometrial Tumor Analysis (IETA) group, established in Chicago in 2008, has created a common consensus to agree on terms and definitions to identify ultrasound findings in the uterine cavity and to establish guidelines to promote the prediction and diagnosis of endometrial disease. Several studies try to use variables other than endometrial thickness e.g. the gray-scale ultrasound morphology of the endometrium, the vascularization of the endometrium as assessed by Doppler ultrasound and clinical variables, in order to discriminate between benign and malignant endometrium in women with postmenopausal bleeding and improve the diagnostic performance of the procedures. Finally, trials including patient characteristics and sonographic characteristics were conducted to design a model for endometrial cancer and then to estimate its risk and clinical usefulness. Some authors are using, as study participants, all postmenopausal women with vaginal bleeding, whereas other authors included only symptomatic postmenopausal women with an endometrial thickness at risk of intrauterine malignancy, the majority of these studies showed fair outcomes with an improvement of diagnostic performance in detecting endometrial cancers. However, up to date, these models are not yet validated externally.
Results
In this study (patient characters): mean values of the clinical variables (Table 1) were: age 56.7, BMI 29.4, Duration since menopause 4.3. 66.8% of patients have no medical disease while, the most frequent medical disorder recorded in diseased patients was hypertension (16.6%) as in Table 2.
| Range | Mean ±SD | |
|---|---|---|
| Age (years) | (47-72) | 56.7 ± 5.7 |
| BMI | (23-42) | 29.4 ± 3.4 |
| Duration since menopause (years) | (2-10) | 4.3 ± 3.3 |
| Parity | No | Percentage % |
| Nuli para | 6 | -5% |
| Multi para | 114 | -95% |
Table 1: Descriptive analysis for demographic and clinical variables of studied group. Total No. = 120.
| Medical disease | No of patients | Percentage % | |
|---|---|---|---|
| Non diseased | 80 | 66.8 | |
| DM | Diseased | 4 | 3.3 |
| HTN | 20 | 16.6 | |
| Hepatic | 4 | 3.3 | |
| Combined disease | 12 | 10 |
Table 2: Medical history of studied group (N=120):
The most common lesions were benign in nature (specially the endometrial hyperplasia with highest frequency about 33%) while the endometrial carcinoma was only 16.7%) (Table 3).
| Lesion | Frequency | Frequency |
|---|---|---|
| Endometrial carcinoma | 20 | 20 |
| Endometrial hyperplasia | 40 | 40 |
| Atrophic endometrium | 22 | 22 |
| Endometrial polyp | 18 | 18 |
| Submucous fibroid polyp | 6 | 6 |
| Non-significant finding | 14 | 14 |
| e.g. (Hormonal effect, | ||
| Ch. Endometritis) |
Table 3: Lesions detected by histopathology in the studied group (N= 120):
Including clinical variables (Age, Parity, BMI, HPN and Diabetes) shows a statistically significant difference between benign and malignant cases. While (duration since menopause, hepatic disease and combined disease) the table shows statistically non-significant differences (Table 4). The mean endometrial thickness in malignancy cases (18.6 ± 7.5).
| variables | Malignant | Benign | Statistical test | P value | |
|---|---|---|---|---|---|
| Range | Age(year) | (55-70) | (47-72) | ||
| Mean ±SD | Age(year) | 61.1±5.4 | 55.7±5.3 | 2.87* | 0.005 |
| Mean (years) ±SD | Duration since menopause | 4.1±3.2 | 5.6±3.7 | 1.174* | 0.246 |
| Nulli n (%) | Parity | 3(30) | 0(0) | 10.11* | |
| Para n (%) | Parity | 7(70) | 50(100) | 10.11* | 0.0014 |
| Range | BMI | 29-42 | 23-33 | 6.5* | |
| Mean ±SD | BMI | 34.3±3.6 | 28.5±2.3 | 6.5* | <0.001 |
| Yes n (%) | HPN | 2(10) | 80(80) | ||
| No n (%) | HPN | 18(90) | 20(20) | 15.77* | <0.001 |
| Yes n (%) | Diabetic | 10(50) | 92(92) | ||
| No n (%) | Diabetic | 10(50) | 8(8) | 8.47* | 0.003 |
| Yes n (%) | Hepatic | 2(10) | 2(2) | ||
| No n (%) | Hepatic | 18(90) | 98(98) | 9.4* | 0.09 |
| Yes n (%) | Combined | 10(50) | 2(2) | ||
| No n (%) | disease | 10(50) | 98(98) | 8.4* | 0.06 |
Table 4: Univariate analysis for comparing clinical variables between endometrial cancer cases (N = 20) and benign cases (N = 100
The most frequently identified sonographic variables with malignancy were endo-heterogenous. Echogenicity, and endo irregularity. Midline, the endo is poorly defined. end.
myo. System, Doppler score > 2, multiple vessel patterns and all show a significant difference between table of benign and malignant cases (Table 5).
| variables | Malignant | Benign | Statistical test | P value | |
|---|---|---|---|---|---|
| Range (mm) | Endo.thick | (9-32) | (5-15) | 5.9* | <0.001 |
| Mean ±SD | 18.6 ± 7.5 | 9.9± 3.2 | |||
| Hetero. n (%) | Endo. Echogenicity | 18 (90) | 8(8) | 28.38* | <0.001 |
| Homo. n (%) | 2 (10) | 92(92) | |||
| Ill-defined n (%) | Endo. Midline | 0 (0) | 4(4) | ||
| Linear n (%) | 2 (20) | 66(66) | 8.86* | 0.011 | |
| Irregular n (%) | 16 (80) | 30(30) | |||
| Regular n (%) | Endo. Myomet. Interface | 4 (20) | 92 (98) | 33.8* | <0.001 |
| Ill-defined n (%) | 16 (80) | 4 (2) | |||
| No flow (1) n (%) | Doppler score | 4 (20) | 26 (26) | ||
| Min. (2) n (%) | 0 (0) | 66 (66) | 33.1* | <0.001 | |
| Mod. (3) n (%) | 8 (40) | 8 (8) | |||
| Sever (4) n (%) | 8 (40) | 0 (0) | |||
| No n (%) | Vascular pattern | 4(20) | 64(23) | ||
| Single n (%) | 0(0) | 20(20) | 25.28* | <0.001 | |
| Multiple n (%) | 14(70) | 66) | |||
| Scattered n (%) | 2(10) | 34(43) | |||
| Circular n (%) | 0(0) | 8(8) |
- 100).
- Endo.
- Endo.
- Power.
- (1.2 cm), endometrium heterogeneous, irregular. Endo. Endo. Midline, endo is illdefined. Myo. myo. Browser (Table 6).
- Score cut off (≥10) had the largest area under receiver operator curve and had the best accuracy for detection of malignancy Area under curve (AUC) =0.94 (Table 7).
- Score cut off
- Sensitivity specificity
- PPV
- NPV
- LR
- LR
- Accuracy
- +v
- −v
- <5
- 10
- 8.6
- 2.3
- 30.7
- 0.1
- 10.4
- 8.9
- ≥5
- 90
- 93
- 75
- 97.7
- 12.8
- 0.1
- 92.8
- ≥10
- 80
- 97.8
- 88.8
- 95.7
- 36.3
- 0.1
- 94.6
Table 6: Validity of model of risk scoring for study group.
| variables | Cut off | AUC | Sensitivity | Specificity | LR +v | LR -v | P* |
|---|---|---|---|---|---|---|---|
| (%) | (%) | ||||||
| Age (year) | 60 | 0.47 | 27.3 | 85.7 | 1.9 | 0.8 | 0.37 |
| Nulli para | - | - | 30 | 100 | 0 | 0.7 | 0.15 |
| BMI | 30 | 0.73 | 90 | 60 | 1.5 | 1.4 | 0.06 |
| HPN | - | - | 10 | 100 | 0 | 0.9 | 0.091 |
| DM | - | - | 50 | 92 | 6.2 | 0.5 | 0.25 |
| Endo.thick. (mm) | 12 | 0.8 | 90 | 78.3 | 4.1 | 0.1 | <0.01 |
| Heterogeneous | - | - | 90 | 92 | 11.2 | 0.1 | <0.001 |
| Endometrium | |||||||
| Irreg.Endo.Midline | - | - | 80 | 70 | 2.6 | 0.2 | <0.001 |
| Ill-defined Endo. Myo. Inter- face | - | - | 80 | 98 | 40 | 0.2 | <0.001 |
| Doppler Score | >2 | - | 80 | 92 | 10 | 0.2 | <0.001 |
| Vas.Pattern (Multiple) | - | - | 70 | 94 | 0.75 | 0.73 | 0.07 |
- 100).
- Endo.
- Endo.
- Power.
- (1.2 cm), endometrium heterogeneous, irregular. Endo. Endo. Midline, endo is illdefined. Myo. myo. Browser (Table 6).
- Score cut off (≥10) had the largest area under receiver operator curve and had the best accuracy for detection of malignancy Area under curve (AUC) =0.94 (Table 7).
- Score cut off
- Sensitivity specificity
- PPV
- NPV
- LR
- LR
- Accuracy
- +v
- −v
- <5
- 10
- 8.6
- 2.3
- 30.7
- 0.1
- 10.4
- 8.9
- ≥5
- 90
- 93
- 75
- 97.7
- 12.8
- 0.1
- 92.8
- ≥10
- 80
- 97.8
- 88.8
- 95.7
- 36.3
- 0.1
- 94.6
Table 6: Validity of model of risk scoring for study group.
Score cut off (≥10) had the largest area under receiver operator curve and had the best accuracy for detection of malignancy.
Confidence interval (95%)
Discussion
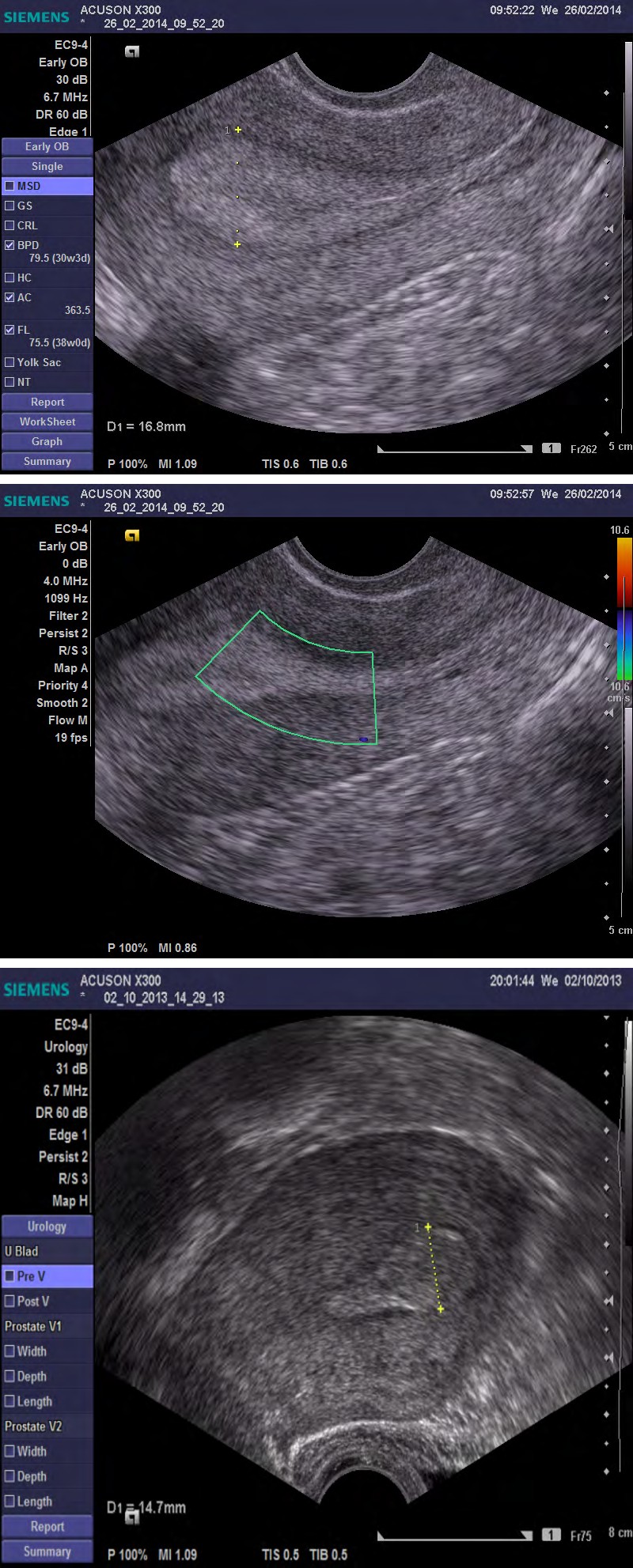
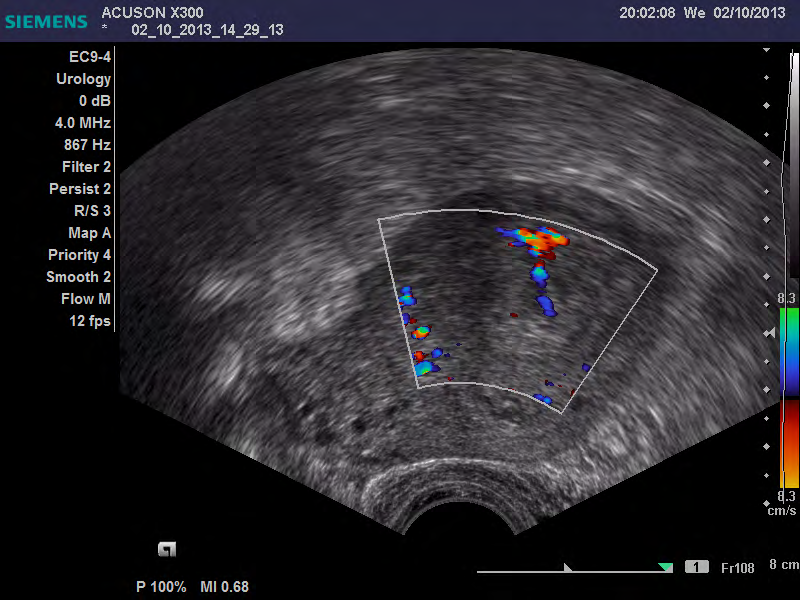
In this study (patient characters): mean values of the clinical variables have age 56.7, BMI 29.4, Duration since menopause 4.3. Also, medical history of the patients showed 66.8% of patients have no medical disease while, the most frequent medical disorder recorded in diseased patients has hypertension (16.6%). In the univariate analysis clinical variables including age, parity, BMI, cases demonstrated a statistically significant difference between hypertension and hyperglycemia. Conversely, Friedenreich C, Rosato V reported that there has no significant value for presence of hypertension in prediction of intrauterine malignancy. It has found that, in univariate analysis between women with and without cancer, there has no disparity in BMI and diabetes. Although found that there have no significant differences in patient characteristics regarding menarche age, menopause age, BMI, parity, diabetes, use of tamoxifen, use of anticoagulants, and history of breast cancer. In this study, histopathological examination revealed endometrial atrophy in 22 patients (18.3% ), endometrial hyperplasia in 40 patients (33.3%), endometrial carcinoma in 20 patients (16.7%), endometrial polyp in 18 patients (15%) and submucous fibroid in 6 patients(5%) and a non-significant finding 14 patients (11.7%). Thus, the commonest cause of postmenopausal bleeding has in this study has endometrial hyperplasia. Conversely, Good found that the mean pathological finding in patients complaining of abnormal uterine bleeding have endometrial polyp and submucous myoma. Lee found that the commonest lesion causing postmenopausal bleeding has endometrial atrophy. In this study (IETA sonographic variables): the mean endometrial thickness has 13.6 ± 5.6 mm, the most frequent sonographic variables (in general) have homogenus endo. echogenicity, linear endo. midline, regular endo. myo. Interface and Doppler score 2 but scattered vascular pattern and no flow pattern with the same frequency. Regarding malignancy: the mean endometrial thickness in malignancy cases has 18.6 mm, the most frequent sonographic variables have heterogeneous endo. midline, ill-defined endo. myo. interface, score doppler> 2 and multiple vessel pattern. All the previous scoring systems tried to reach the best malignancy model with the highest validity in prediction of endometrial cancer but in more complicated fashion.
Conclusion
Words used to characterize endometrial sonographic characteristics identified by the (IETA group) has clinically useful and appropriate for endometrium evaluation using a standardized measuring technique. The implementation of a malignancy model for postmenopausal bleeding cases makes it easy to distinguish cases into low-risk cases with the ability to restrict the dangerous invasive procedure
Acknowledgment
I acknowledge for this important work with Honorable Respected Dr. R.S.Paranjape, World Renowned Scientist & Retired Director & Scientist ‘G High Grade Institute National AIDS Research Institute Pune. This has inspired & captured the imagination and attention of across the research and pure service.
References
-
Rahul H (2017) A2 Milk Fact not Fiction it has Contrast Medicine: Revise. Adv Complement Alt Med 1(1): 7.
-
Rahul Hajare (2018) New “Cancer Pill” Renders Chemo Obsolete IPSR 1(1): 1-3.
-
Rahul Hajare (2016) Characterization of novel 2-Indolinone derivatives as anticancer and cytotoxic activity. World j pharm pharm sci 5(1): 1995-1002.
-
Hajare R (2017) A1 Milk Needle in a Haystack. J Tradit Med Clin Natur 6: e133.
-
Rahul Hajare (2017) Response to a 2- Indolinones laboratory based regimen analogous in cancerous– infected cells. Innovations in Cancer Research and Regenerative Medicine, Sept 10th - 13th 2017 - Ho Chi Minh city, Vietnam, conference proceeding publication.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study