Patients with Chronic Constipation Experience Psychological Stress as Measured By the POMS2 Test and Salivary Stress Markers
Background: Psychological stress is known to lead to the pathogenesis and exacerbation of constipation. Therefore, it is important to understand the stress status in patients with constipation to treat constipation and prevent its exacerbation. Until now, the stress status of patients has been subjectively evaluated mainly by questionnaires, but in recent years it has become possible to objectively evaluate it by measuring stress markers in saliva. This study evaluated the stress status in patients with chronic constipation from both subjective and objective perspectives. Methods: Eighty-four adult females with chronic constipation and 20 healthy adult female volunteers as controls were enrolled in this study. All subjects were subjectively evaluated for their mood using the shortened Profile of Mood StatesSecond Edition (POMS2) and objectively evaluated by measuring salivary stress markers, such as cortisol, chromogen A, oxytocin, and secretory immunoglobulin A (s-IgA) using Enzyme-Linked Immuno Sorbent Assay. Results: In the POMS2 analysis, the T-scores of negative mood subscales, such as Anger–Hostility, Confusion–Bewilderment, Depression–Dejection, Fatigue–Inertia, and Tension–Anxiety were significantly higher in the constipation group than in the control group. In contrast, positive mood subscale scores, such as Vigor–Activity and Friendliness were not significantly different between the two groups. These results significantly increased the total mood disorder score, which comprehensively reflects a negative mood in the constipation group compared to the control group. In the stress marker analyses, cortisol, chromogranin A, and s-IgA concentrations in the constipation group were significantly higher than those in the control group. In contrast, the oxytocin concentration in the constipation group tended to be lower than in the control group. Conclusion: These results suggest that patients with constipation have more stressful negative emotions, such as anxiety, depression, tension, and fatigue than healthy individuals. This study will be important and useful when considering the treatment, exacerbation, or prevention of constipation.
Introduction
Constipation is a condition in which a sufficient amount of feces is not comfortably excreted from the body because of infrequent or difficult passage [1]. The Japanese Society of Gastroenterology defines it as a condition in which no defecation for three days or more is observed, or when there is a feeling of an incomplete bowel movement, even if the defection is performed every day.
According to the 2016 Comprehensive Survey of Living Conditions conducted by the Japanese Ministry of Health, Labor and Welfare, the prevalence of constipation in Japan is reported to be 2%-5%, and it tends to be higher in women (4.6%) than in men (2.5%) and to increase with age in both men and women [2]. The prevalence in Western countries is approximately 15% (2%-28%), and as in Japan, women are more likely to complain of constipation than men and the prevalence increases with age in both men and women [3].
Constipation can be acute or chronic, but what is generally referred to as “constipation” is chronic constipation, which includes functional constipation, drug-induced constipation, organic constipation, and symptomatic constipation. The most common type of constipation is functional constipation, including flaccid constipation, spasmodic constipation, and rectal constipation [4]. However, constipation causes a variety of symptoms, such as abdominal pain, abdomen enlarged feeling (or abdominal distension), nausea, loss of appetite, and malnutrition, resulting in a significantly decrease in the quality of life and labor productivity [1].
Psychologically, patients with chronic constipation have been reported to have a higher prevalence of depression, anxiety, somatization symptoms (or hypochondriasis), and neuropathy (neurological disorders), such as Parkinson’s disease and multiple sclerosis [5, 6]. In addition, patients with chronic constipation have been reported to have a higher complication rate for ischemic heart diseases, such as myocardial infarction and angina, leading to increased mortality [7]. The findings described above suggest that patients with constipation routinely experience more mental and physical stress than patients without constipation. In fact, patients with functional bowel disease, including constipation, have been reported to experience psychological distress [5]. Psychological stress was also reported to be strongly associated with the development of constipation in children [8] and adolescents [9]. In Korean male college students, life stress was reported to be strongly associated with functional constipation [10]. Thus, a positive correlation has been shown between psychological stress and constipation, and stress load is considered to be one of the causes and exacerbations of constipation. Therefore, understanding the stress status in patients with constipation may be useful in the treatment and prevention of constipation.
These psychological stresses have been evaluated by subjective psychological tests using various questionnaires. Psychological tests include the Manifest Anxiety Scale (MAS), Self-Rating Depressive Scale (SDS), the Minnesota Multiphasic Personality Inventory (MMPI), and Profile of Mood States-Second Edition (POMS2) or its shortened version [11, 12]. The MAS, SDS, and MMPI tests determine a subject’s personality traits, namely and respectively the tendency for anxiety, depression, and multifaceted personality. In contrast, the POMS2 or its shortened version is a test that does not evaluate personality traits but rather changes in mood over time, such as the last few hours or days. The advantage of this test, which is used in various fields, such as medical care, mental health, and sports or exercise, is that it measures multiple mood states at the same time with a single questionnaire [13]. However, since subjective factors strongly influence the mood or psychological evaluations, it is desirable to perform these questionnaire-based tests in combination with an objective evaluation.
One objective assessment of stress status is to measure biomarkers that have been suggested to reflect stress status. To evaluate the stress state more accurately, it is necessary to measure biomarkers in biological samples, such as blood and tissues, in a state with no stress load other than stress stimulation. Thus, since invasive blood collection involves mental stress, it is desirable to use biological samples, such as urine, saliva, tears, and sweat, that can be collected noninvasively. Recently, attention has been focused on saliva, which is easy to collect. Stress-related biomarkers cortisol, chromogranin A, oxytocin, and secretory immunoglobulin A (s-IgA) have been identified in saliva. These salivary biomarkers have been measured in many stress-related clinical studies [14].
The purpose of the present study was to evaluate the stress status in patients with chronic constipation. To achieve this goal, 84 adult female patients with chronic constipation (constipation group) and 20 healthy adult female volunteers (control group) were enrolled. All subjects were then subjectively evaluated for their mood using a shortened version of POMS2 and objectively evaluated by measuring salivary stress markers (cortisol, chromogranin A, oxytocin, and s-IgA).
Materials and Methods
Participants and Ethics Statement
Of the patients who first visited the constipation outpatient department of Juntendo Hospital (Tokyo, Japan) from 2015 to 2018, 84 adult female patients with chronic constipation aged 20–70 years old (average 43.0 ± 1.4 years) were enrolled as the constipation group in the present study.
The three criteria for registration were: (1) no bowel movements for three days or more (Patients with only a sensation of incomplete defecation were not enrolled in this study), (2) no use of laxatives and (3) no illness other than constipation. Twenty healthy adult female volunteers aged 20–70 years old (mean 37.3 ± 2.3 years) were enrolled as controls.
The three criteria for registration of control subjects were: (1) daily defecation, (2) regularity of time to defecate and no feeling of incomplete bowel movements and (3) no illness, including constipation.
Informed consent was obtained from all individual participants included in the present study. All procedures applied in the present study complied with the Helsinki Declaration and the Ethical Guidelines for Medical and Health Research Involving Human Subjects and were approved by the Ethics Committee of Medical Corp Koyokai.
Evaluation of Mood Status
The mood profiles of all subjects in the constipation and control groups were analyzed using a shortened version of POMS2, a psychological rating scale to assess transient, distinct mood states [11, 12].
The POMS2 shortened version is a mood inventory containing 35 items that assess the following seven different subscales (moods): Anger-Hostility (AH), Confusion– Bewilderment (CB), Depression–Dejection (DD), Fatigue– Inertia (FI), Tension–Anxiety (TA), Vigor–Activity (VA), and Friendliness (F). Subjects were asked to indicate mood states during the previous 1-week period on a 5-point score that ranges from “not-at-all” (0) to “extremely” (4). The sum of the scores was calculated for each subscale. The total mood disorder (TMD) score was calculated from the individual total score of six subscales, excluding subscale F as follows: TMD = (AH + CB + DD + FI + TA) - VA. Evaluation of individual subscales and TMDs was performed using standardized scores (T-scores) that were converted from the individual total subscale scores and TMD scores using a conversion table.
Statistical Analysis
All analytical data were nonparametric data with no normal distribution. Therefore, those data are shown as box plots. The box represents the median ± interquartile range (IQR), and the whiskers of the box represent the 1.5 × IQR range. Statistical significance between the constipation and healthy control groups in all analyses was assessed using the nonparametric Mann–Whitney U test using EZR 1.52 software. The significance level was accepted at P < 0.05.
Results
Evaluation of Mood Status
Figure 1 shows the seven subscales and TMDs evaluated by the shortened POMS2 version in the constipation and control groups. The T-scores for AH, CB, DD, FI, and TA included in the negative mood subscale were significantly higher in the constipation group than in the control group. However, the T-scores for VA and F included in the positive mood subscale were not significantly different between the two groups. The T-score of TMD, which comprehensively reflects a negative mood, was significantly higher in the constipation group than in the control group.
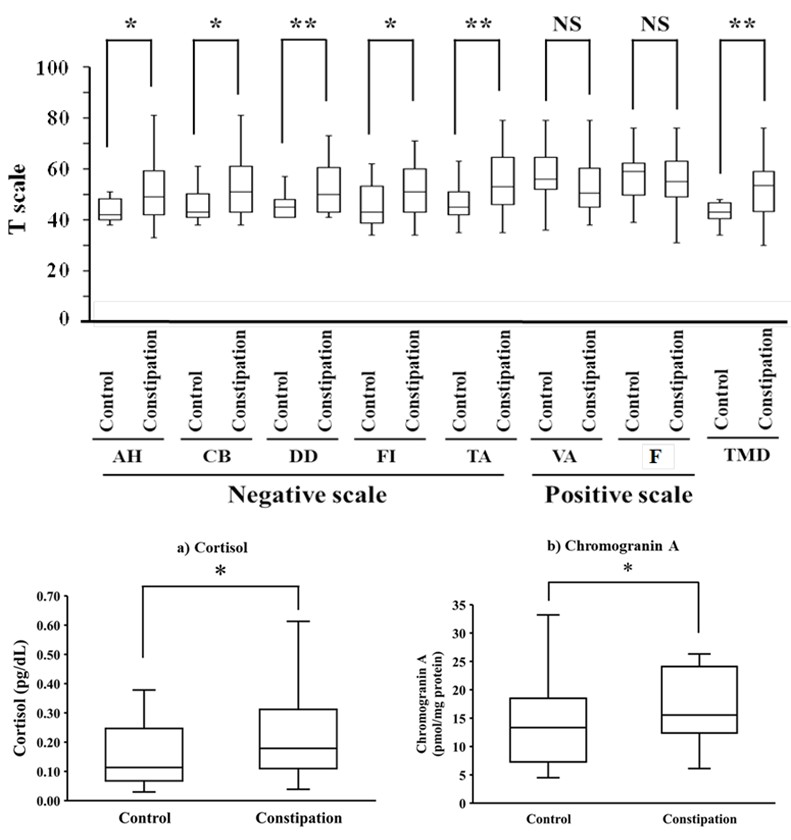
Figure 1: The evaluation of seven subscales and TMDs by the shortened version of POMS2 in the constipation patient group and the healthy subject group as control. All data are shown as box plots. The box represents the median ± interquartile range (IQR), and the whiskers of the box represent the 1.5 × IQR range. Statistical significance between both groups was assessed by Mann–Whitney U test: *P < 0.05, **P < 0.01, and NS = No significance.
Stress-Related Biomarkers in Saliva
The salivary cortisol, chromogranin A, s-IgA, and oxytocin concentrations in the constipation patient group and the healthy control group are shown in Figures 2a, 2b, 2c, and 2d, respectively. The cortisol, chromogranin A, and s-IgA concentrations in the constipation group were significantly higher than those in the control group. Oxytocin levels were not significantly different between the two groups, but the level in the constipation group tended to be lower than that in the control group (P = 0.070).
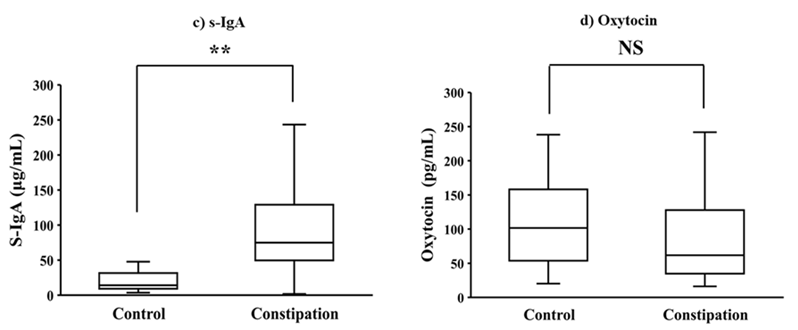
Figure 2: Comparison of salivary stress-related hormone levels between the constipation and control groups. Each of the stress-related hormones, such as cortisol, chromogranin A, s-IgA, and oxytocin was measured using a separate analytical ELISA kit. Each data set is shown as a box plot. The box represents the median ± interquartile range (IQR), and the whiskers of the box represent the 1.5 × IQR range. The Mann–Whitney U test assessed statistical significance between both groups: * P < 0.05, ** P < 0.01, and NS = no significance.
Discussion
The purpose of the present study was to evaluate the stress status in patients with constipation. To achieve this goal, 84 adult female patients with chronic constipation and 20 healthy adult female volunteers were enrolled. Both a subjective emotional profile test using the shortened POMS2 version and objective analysis of some stress markers in saliva were performed in all subjects.
There have been several reports on the relationship between constipation and stress. Heymen et al. performed an MMPI to assess personality differences in patients with chronic pelvic floor disorders, including constipation, and found significantly higher scores for hypochondriasis, depression, and hysteria in the constipation group [5]. From this result, they suggested that patients with constipation may manifest their psychologic distress as physical symptoms. Using a bowel disease questionnaire, Jiang et al. reported that the abdominal bloating and distention observed in constipation and irritable bowel syndrome caused somatic distress in patients [15]. In an epidemiological study investigating comorbidities in patients with chronic constipation using a self-reported gastrointestinal symptom questionnaire, patients with chronic constipation were more likely to have ischemic heart disease and depression or anxiety [6]. In cohort studies using a self-administered structured questionnaire to clarify the association between psychological stress and constipation, psychological stress was strongly associated with the development of constipation in children [8] and adolescents [9]. In a case- control study, which investigated the relationship between the onset of functional constipation and life stress in male university students using a self-administered questionnaire, life stress was reported to be strongly associated with functional constipation [10]. These reports show that there is a positive correlation between stress and constipation, that is, various psychological stresses such as depression, anxiety, and distress are associated with the onset and exacerbation of constipation. In addition, the data suggest that patients with constipation are prone to psychological stress-sensitive hypochondriasis. However, PONS2, which was used in all patients with constipation enrolled in this study, is not a personality tendency test, but a mood assessment over a period of time, such as the past few hours or days. The POMS2 has been well-established for standardization, reliability, and validity [11, 12]. In the present study, all negative mood subscale scores (AH, CB, DD, FI, and TA) in the constipation group were higher than those in the control group. This result suggests that negative mood predominates in patients with constipation over positive mood, and is also supported by the fact that the TMD scores were higher in patients with constipation than in controls. This shows that the patients with constipation are experiencing negative mood psychological stress such as depression, malaise, and anxiety. However, the positive mood subscale scores (VA and F) were not significantly different between the two groups, indicating that the high negative mood was not due to impaired positive emotions. In other words, the data suggest that positive emotions were retained. Stress has been suggested to be either a triggering or aggravating factor for many diseases and pathological conditions, including a variety of psychological symptoms, such as anxiety, tension, depression, lethargy, anger, confusion, and fatigue [16]. Therefore, understanding the mood states of patients with constipation using the POMS2 provides important information for the treatment of constipation. A unique feature of this study was the combination of the subjective evaluation with an objective measure of stress-related biomarkers in saliva to make the questionnaire-based POMS2 test more precise.
The use of saliva to measure stress-related substances compared to blood has obvious advantages in terms of sample collection, including speed, ease, subject mobility, and noninvasiveness. In the present study, salivary cortisol, chromogranin A, oxytocin, and s-IgA were selected as stress markers to objectively and easily assess stress status in constipated patients. The stress response system includes the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic-adrenomedullary (SAM) system, whose activities can be biochemically evaluated by measuring cortisol and catecholamines, respectively [17]. Psychological and physical stress has been reported to increase HPA axis activity and subsequently increase salivary cortisol levels [18]. Subjects under chronic episode stress have been reported to have higher scores for “FI” and “TA” in the shortened POMS test, and also had higher salivary cortisol levels [19].
Chromogranin A is an acidic glycoprotein stored and coreleased with catecholamines by exocytosis from the adrenal medulla and sympathetic nerve endings [20]. Catecholamine levels are commonly used as a sensitive biochemical index of stress. Still, it is difficult to measure their concentrations in the saliva due to generally low levels and rapid degradation. Therefore, salivary chromogranin A is used as an alternative marker for catecholamines. Salivary chromogranin A levels are commonly measured as reliable biological markers of changes in the SAM system activity caused by prolonged psychosocial stress [21]. Chromogranin A levels in saliva have been reported to increase with computer-controlled psychological stress [22]. It has also been suggested that it reflects psychological stress more quickly and sensitively than cortisol [21, 22].
The neuropeptide oxytocin not only plays a role in uterine contractions during parturition and milk production during lactation but is also released within multiple regions of the brain, affecting behavior and neuroendocrine responses to stress [23]. Several studies suggest that oxytocin is involved in the central regulation of the response to stress through the regulation of the corticotropin-releasing hormone; i.e., oxytocin is associated with an inhibitory effect on adrenocorticotropic hormone secretion followed by impaired corticosterone secretion [24]. Evidence from rodent models suggests that both acute and chronic oxytocin administration reduces physiological and behavioral stress responsiveness [25]. In humans, stress responses have been reported to be attenuated by exogenous oxytocin administration [26]. These findings suggest that oxytocin plays a role in relieving stress.
S-IgA is a protein present in the mucus of mucous membranes, such as the oral cavity, nasal cavity, and digestive organs. It is mainly responsible for the local immune system of the mucosa [27]. Thus, s-IgA in the saliva is a marker of the immune system, but since the immune system is closely related to stress, it has also been used as a stress marker in recent years. For example, it has been reported that s-IgA in saliva generally decreases under chronic academic stress [28] and temporarily increases or decreases depending on the type of stress situation under acute psychosocial stress [14].
In this study, salivary cortisol and chromogranin A levels in the constipation group were significantly higher than in the control group. In contrast, the oxytocin levels in the constipation group tended to be lower than in the control group. These results suggest that patients with constipation are more stressed than healthy people. However, contrary to our expectations, the salivary levels of s-IgA were significantly higher in patients with constipation than in healthy individuals. Although the cause cannot be elucidated in this study, it is worth noticing that the reflection of the psycho- immune response may differ depending on the type and condition of stress [14]. Because the present study targeted patients with constipation, it is possible that in our study s-IgA worked more as an immune system marker rather than as a psychological stress marker for constipation [29]. This hypothesis is supported by the fact that constipation is known to cause abnormalities in the intestinal environment, such as intestinal inflammation and disturbance of the intestinal flora [30]. Therefore, the constipation patients enrolled in this study may have elevated s-IgA levels, reflecting their biological defense response to these abnormalities. It is necessary to examine the characteristics of s-IgA as a stress marker in more detail in the future.
The combined results of subjective emotional profile test using the POMS2 version and objective analysis of some stress markers in saliva suggest that patients with constipation are more stressed than healthy individuals. Not only does stress cause constipation, but the constipation caused by stress causes new stress, which in turn exacerbates constipation. Thus, constipation and stress are presumed to have a “negative spiral” relationship that exacerbates constipation. In this study, the stress status of patients with chronic constipation was clarified by both subjective and objective evaluations. Considering that psychological stress induces or exacerbates constipation [5, 8, 9, 10] it is important to understand the current state of stress in these patients.
Conclusion
We evaluated the stress status of constipation patients by comparing 84 adult female patients with chronic constipation with 20 healthy adult female volunteers. Both the subjective emotional profile test using the shortened POMS2 version and objective analysis of some stress markers in saliva were used as stress assessments in constipation. The results showed that constipated patients were more stressed and had negative emotions, such as anxiety, depression, tension, and fatigue than healthy individuals. By combining both these assessments, our approach to understanding the stress status of patients with constipation will provide important and useful information for the treatment and prevention of constipation and constipation worsening cases.
References
-
Sun SX, Dibonaventura M, Purayidathil FW, Wagner JS, Dabbous O, et al. (2011) Impact of Chronic Constipation on Health-Related Quality of Life, Work Productivity, and Healthcare Resource Use: An Analysis of the National Health and Wellness Survey. Dig Dis Sci 56(9): 2688- 2695.
-
Kawamura Y, Yamamoto S, Funaki Y, Ohashi W, Yamamoto K, et al. (2020) Internet Survey on the Actual Situation of Constipation in the Japanese Population Under 70 Years Old: Focus on Functional Constipation and Constipation- Predominant Irritable Bowel Syndrome. J Gastroenterol 55(1): 27-38.
-
Talley NJ, O’Keefe EA, Zinsmeister AR, Melton III LJ (1992) Prevalence of Gastrointestinal Symptoms in the Elderly: A Population-Based Study. Gastroenterology 102(3): 895-901.
-
Mimura T, Honma Y, Horie H (2019) Diagnosis and Treatment of Chronic Constipation. J Jpn Soc Coloproctol 72(10): 583-599.
-
Heymen S, Wexner SD, Gulledge AD (1993) MMPI Assessment of Patients with Functional Bowel Disorders. Dis Colon Rectum 36(6): 593-596.
-
Choung RS, Rey E, Locke GR, Schleck CD, Baum C, et al. (2016) Chronic Constipation and Co-Morbidities: A Prospective Population-Based Nested Case-Control Study. United European Gastroenterol J 4(1): 142-151.
-
Honkura K, Tomata Y, Sugiyama K, Kaiho Y, Watanabe T, et al. (2016) Defecation Frequency and Cardiovascular Disease Mortality in Japan: The Ohsaki Cohort Study. Atherosclerosis 246: 251-256.
-
Yamada M, Sekine M, Tatsuse T (2019) Psychological Stress, Family Environment and Constipation in Japanese Children: The Toyama Birth Cohort Study. J Epidemiol 29(6): 220-226.
-
Yamada M, Sekine M, Tatsuse T, Fujimura Y (2021) Lifestyle, Psychological Stress and Incidence of Adolescent Constipation: Results from the Toyama Birth Cohort Study. BMC Public Health 21(1): 47.
-
You JS, Park JY, Chang KJ (2010) A Case-Control Study on the Dietary Taurine Intake, Nutrient Status and Life Stress of Functional Constipation Patients in Korean Male College Students. J Biomed Sci 17(1): 41.
-
Heuchert JP, McNair DM (2012) Profile of Mood States 2nd (Edn.), Adult. Multi-Health Inc. North Tonawada, NY, USA.
-
Komura H, Hirose H, Yokoyama K (2015) Relationship of the Japanese Translation of the Profile of Mood States Second Edition (POMS 2®) to the First Edition (POMS®). Juntendo Med J 61(5): 517-519.
-
Higashikawa F, Kanno K, Ogata A, Sugiyama M (2020) Reduction of Fatigue and Anger-Hostility by the Oral Administration of 5-Aminolevulinic Acid Phosphate: A Randomized, Double-Blind, Placebo-Controlled, Parallel Study. Sci Rep 10(1): 16004.
-
Niimi M (2018) Stress Evaluation Using Salivary Biomarkers: A Review. J Kagawa Pref Univ Health Sci 9: 1-8.
-
Jiang X, Locke GR, Choung RS, Zinsmeister AR, Schleck CD, et al. (2008) Prevalence and Risk Factors for Abdominal Bloating and Visible Distention: A Population-Based Study. Gut 57(6): 756-763.
-
Yaribeygi H, Panahi Y, Sahraei H, Johnston TP, Sahebkar A (2017) The Impact of Stress on Body Function: A Review. EXCLI J 16: 1057-1072.
-
Buske-Kirschbaum A, Geiben A, Höllig H, Morschhäuser E, Hellhammer D (2002) Altered Responsiveness of the Hypothalamus-Pituitary-Adrenal Axis and the Sympathetic Adrenomedullary System to Stress in Patients with Atopic Dermatitis. J Clin Endocrinol Metab 87(9): 4245-4251.
-
Kirschbaum C, Hellhammer DH (1994) Salivary Cortisol in Psychoneuroendocrine Research: Recent Developments and Applications. Psychoneuroendocrinology 19(4): 313-333.
-
Izawa S, Sugaya N, Ogawa N, Nagano Y, Nakano M, et al. (2007) Episodic Stress Associated with Writing a Graduation Thesis and Free Cortisol Secretion After Awakening. Int J Psychophysiol 64(2): 141-145.
-
O Connor DT, Frigon RP, Sokoloff RL (1984) Human Chromogranin A: Purification and Characterization from Catecholamine Storage Vesicles of Human Pheochromocytoma. Hypertension 6(1): 2-12.
-
Den R, Toda M, Ohira M, Morimoto K (2011) Levels of Awakening Salivary CgA in Response to Stress in Healthy Subjects. Environ Health Prev Med 16(3): 155-157.
-
Nakane H, Asami O, Yamada Y, Ohira H (2002) Effect of Negative Air Ions on Computer Operation, Anxiety and Salivary Chromogranin A-Like Immunoreactivity. Int J Psychophysiol 46(1): 85-89.
-
Bell AF, Erickson EN, Carter CS (2014) Beyond Labor: The Role of Natural and Synthetic Oxytocin in the Transition to Motherhood. J Midwifery Womens Health 59(1): 35- 42.
-
Dief AE, Sivukhina EV, Jirikowski GF (2018) Oxytocin and Stress Response. Open J Endocr Metab Dis 8(3): 93-104.
-
Slattery DA, Neumann ID (2010) Chronic icv Oxytocin Attenuates the Pathological High Anxiety State of Selectively Bred Wistar Rats. Neuropharmacol 58(1): 56-61.
-
McQuaid RJ, McInnis OA, Paric A, Al Yawer F, Matheson K, et al. (2016) Relations between Plasma Oxytocin and Cortisol: The Stress Buffering Role of Social Support. Neurobiol Stress 3: 52-60.
-
Mestecky J (1993) Saliva as a manifestation of the common mucosal immune system. Ann N Y Acad Sci 694: 184-194.
-
Deinzer R, Kleineidam C, Stiller Winkler R, Idel H, Bachg D (2000) Prolonged Reduction of Salivary Immunoglobulin A (Siga) After a Major Academic Exam. Int J Psychophysiol 37(3): 219-232.
-
Engeland CG, Hugo FN, Hilgert JB, Nascimento GG, Junges R, et al. (2016) The effects of psychological distress on salivary secretory immunity. Brain Behav Immun 52: 11- 17.
-
Ohkusa T, Koido S, Nishikawa Y, Sato N (2019) Gut Microbiota and Chronic Constipation: A Review and Update. Front Med 6: 19.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study