Evaluation of the Use of SGLT2 Inhibitor in the Symptomatic Improvement of Patients with Chagas Cardiomyopathy
Chagas cardiomyopathy (CC) remains a serious disease with a poor prognosis in Latin America, and its treatment is based on the use of drugs commonly prescribed for heart failure (HF). Sodium glucose cotransporter-2 inhibitors (SGTL2i) improved cardiovascular mortality and HF hospitalization in several trials. As a result of growing body evidence in HF from different etiologies, it is reasonable to consider its potential benefits in CC. This study describes the impact on quality of life (QoL), using the New York Heart Association (NYHA) classification, the KCCQ and the 6MWT, in symptomatic patients with CC after the use of Dapagliflozin, an SGTL2i inhibitor, for a 12-week period. In this case of series of patients with Chagas Heart Disease, the use of dapagliflozin was associated with significant improvement in symptoms assessed by the NYHA classification and KCCQ scores, however there was not an improvement in performance on the 6MWT.
Introduction
Chagas Heart Disease (ChHD) is an important cause of Heart Failure (HF) in Latin America with high rates of morbidity and mortality. Due to its unique etiopathogenesis, it has worse prognosis compared to other forms of cardiomyopathy, including hypertensive cardiomyopathy, idiopathic dilated cardiomyopathy, and ischemic cardiomyopathy [1]. Most clinical trials that have established the standard medical treatment for HF included few individuals with chagas cardiomyopathy (CC), so in clinical practice physicians prescribe these drugs on the assumption that they would have the same benefits in these patients [1].
Sodium-glucose cotransporter type 2 inhibitors (SGLT2I) have become an important class of drugs in the management of HF, with many randomized clinical trials (RCTs) showing better clinical outcomes after their use with reduced length of hospital stay, cardiovascular mortality and symptomatic improvement (DAPA-HF, EMPEROR-Reduced, EMPEROR-Preserved) [2, 3, 4]. The aim of this study is to describe the impact on quality of life (QoL), using the New York Heart Association (NYHA) classification, the KCCQ and the 6MWT, in symptomatic patients with ChHD after the use of Dapagliflozin, an SGTLT2I, for a 12-week period.
Methods
This is a prospective and interventional case of series from a single center, at Ana Nery Hospital, Salvador-BA- Brazil, between June 2021 and February 2022. The research was based on medical interview of selected patients registered at the institution. We used the NYHA classification, the Kansas City Cardiomyopathy Questionnaire (KCCQ) and the 6-minute walk test (6MWT) as assessment methods, which are well-known tools in health status assessment and symptom assessment in patients with HF [5, 6].
Study Population
Eligibility requirements included patients with a diagnosis of ChHD, confirmed by serology (ELISA and IFI), with left ventricular ejection fraction (LVEF) ≤ 40%, who are still symptomatic despite optimized clinical treatment for HF before the addition of Dapagliflozin. Exclusion criteria were type 1 diabetes mellitus, estimated glomerular filtration rate (eGFR) below 30 ml per minute per 1.73 m2 or unacceptable side effects associated with an SGLT2 inhibitor.
According to resolution 466/2012 of the National Health Council, the present study was approved by the local research ethics committee, and all procedures were performed in accordance with the Declaration of Helsinki.
Data Collection
All patients were selected from the database of electronic medical records of individuals who were already being followed up in specialized outpatient clinics for Heart Failure and/or Arrhythmology at our Hospital.
Patients were evaluated by our investigators in a clinical consultation. Demographic and clinical characteristics, as well as NYHA classification, KCCQ and 6MWT were collected before and after the use of dapagliflozin.
Study Outcomes
The primary outcome was to assess symptomatic improvement through the NYHA classification, KCCQ and 6MWT after three months of the use of dapaglifozin.
Statistical Analysis
Categorical variables were described as frequencies and percentages. The Kolmogorov–Smirnov test was used to verify the normal distribution of continuous variables. Variables with normal distribution were described by means and standard deviations and compared using Student’s t-test. Variables with non-normal distribution were described by the medians and interquartile ranges 25% and 75% and compared using the Wilcoxon test. A value of P < .05 was statistically significant. The Statistical Package for the Social Sciences (SPSS) version 20.0 was used for the analysis of all data. The data were analyzed using IBM SPSS Statistical Package v.21 (IBM Corporation, Armonk, NY).
Results
This study selected 14 patients with Chagas cardiomyopathy who started dapagliflozin. Two patients dropped out the study because of worsening in their kidney function and one because of recent implantation of cardiac resynchronization therapy. A total of 11 patients completed the three months follow-up. The baseline characteristics are shown in Table 1. The majority (54.55%) were men, and the median age was 65 years, with six (54.54%) diagnosed with hypertension, four (36.36%) with diabetes and four (36.36%) with atrial fibrillation.
| Population Baseline. | N= 11 |
|---|---|
| Age, (min-max) | 65.36 (49-79) |
| Female, n (%) | 5 (45.4%) |
| LVEF (min-max) | 32 (21-39) |
| LVDD (min-max) | 56.25 (48-80) |
| LVSD (min-max) | 52.27 (41-72) |
| Hypertesion, n (%) | 6 (54.5%) |
| Diabetes, n (%) | 4 (36.4%) |
| AFib, n (%) | 4 (36.4%) |
| Stroke, n (%) | 1 (9%) |
| Pacemaker, n (%) | 8 (72.7%) |
| ICD, n (%) | 3 (27.3%) |
| CRT, n (%) | 1 (9%) |
| Sacubitril/Valsartan, n (%) / fulldose, n (%) | 3 (27.3%) / 1 (9%) |
| ACEI or ARB, n (%) / full-dose, n(%) | 7 (63.6%) / 3(27.3%) |
| Beta-blockers, n (%) / full- dose, n(%) | 10 (90.3%) / 3 (27.3%) |
| Spironolactone, n (%) | 9 (81.8%) |
| Furosemide, n (%) | 9 (81.8%) |
Table 1: The majority (54.55%) were men, and the median age was 65 years, with six (54.54%) diagnosed with hypertension, four (36
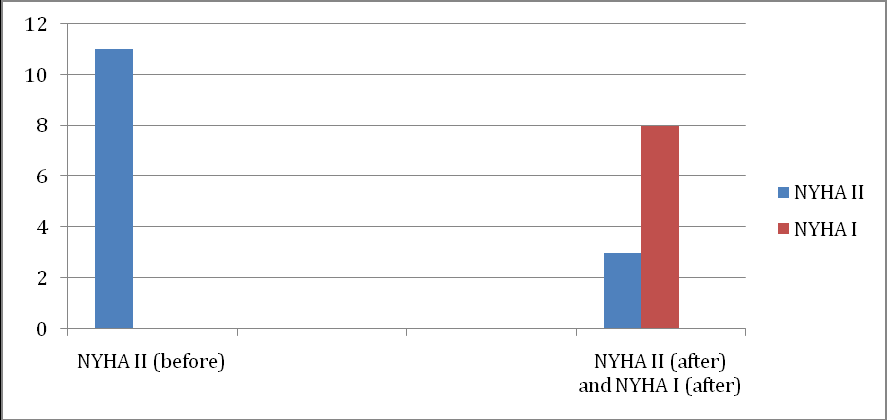
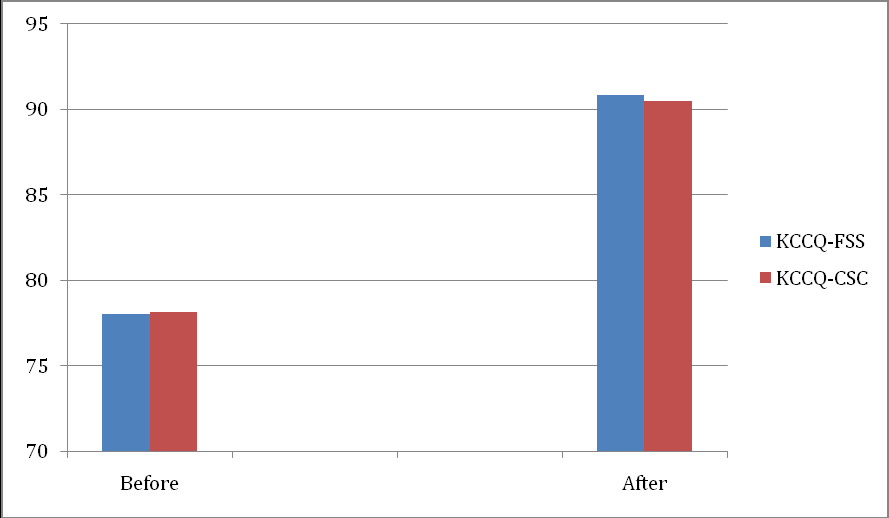
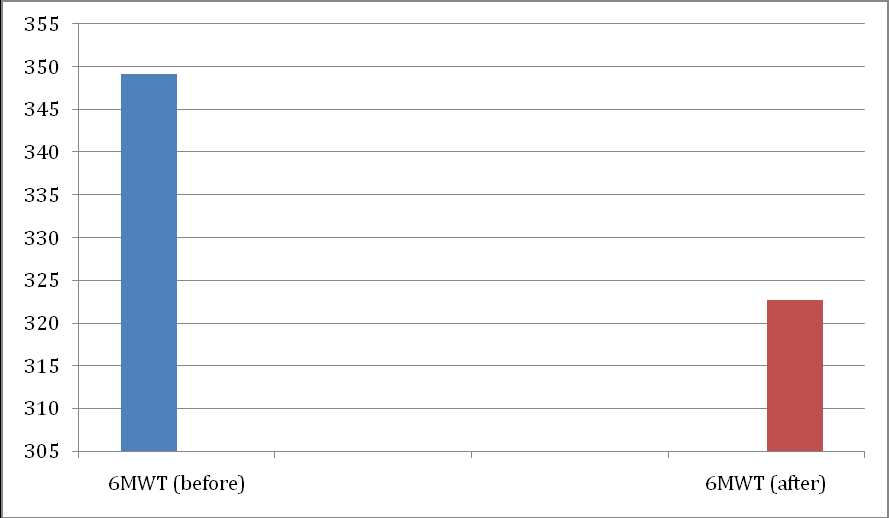
All patients were NYHA II in the first appointment and the medians KCCQ-FSS and KCCQ-CSC were 78.13 and 78, respectively. After twelve weeks, eight patients were considered NYHA I, with significant improvement in symptoms after the use of dapagliflozin (p=0.008) (Figure 1). In addition, there was an improvement in the median KCCQ-FSS score (78.13 to 90.83, p=0.008) and in the median KCCQ-CSC score (78 to 90.47, p=0.009) (Figure 2). However, no difference was observed in the median of meters covered in the 6MWT (349.18 to 322.63, p= 0.286) after the use of dapagiflozin (Figure 3).
Discussion
In this case of series of patients with ChHD, the use of dapagliflozin for a period of three months was associated with significant improvement in symptoms assessed by the NYHA classification and KCCQ scores.
Although the KCCQ and NYHA classification showed improvement in the quality of life of our patients, these results were not reproduced in an improvement in performance on the 6MWT after the use of dapagliflozin. The 6MWT is an easy, well tolerated, and reproducible test, and the “reduced function ability and exercise tolerance in patients with heart failure (HF) are associated with poor quality of life and a worse prognosis”, as Giannitsi, et al. [7] highlighted. Thus, we used this tool to have greater confidence and reproducibility in the evaluation of our patients, considering that symptoms such as dyspnea can be easily misinterpreted.
In a subanalysis of the DAPA-HF Trial [2], the authors applied the KCCQ as a secondary endpoint to assess symptoms and observed better results in the dapagliflozin arm, as evidenced in our study. In addition, He Z, Yang L et al published a meta-analysis in the International Journal of Cardiology, including nine articles and a total of 9,428 patients [8], and showed that SGLT2I improves quality of life in HF, but does not improve exercise capacity, a finding that agrees with our results.
Chagas heart disease has a multifactorial and complex pathophysiology that is related to a poor prognosis, mainly because it presents with more severe cardiac dysfunction and worse clinical condition in a short period of time [9]. Most RCTs involving the treatment of heart failure have included a small sample of individuals with ChHD and, to date, there are no published studies on the use of ISGTL2 in Chagas heart disease. The DAPA-HF Trial had participants in the Latin America, but it did not specify if there were ChHD patients enrolled in the study.
The cardiovascular benefits of using SGLTI2 in HF have already been demonstrated, but its mechanisms are still unclear. Some theories have been proposed as its effect on diuresis/natriuresis, improvement of cardiac energy metabolism, reduction of myocardial inflammation, inhibition of the sympathetic nervous system, prevention of adverse cardiac remodeling, among others [10]. Regardless, so far, we already know that SGLT2I has a great impact on the prognosis of heart failure with a 26% reduction in hospitalization due to worsening of cardiovascular disease or death. Thus, further studies are needed to better understand and establish its role in a serious public health problem such as Chagas cardiomyopathy.
Conclusion
Although it is a small open single-arm study with a short follow-up period, we were able to demonstrate an improvement in HF symptoms in individuals with Chagas disease, illustrating an important step towards understanding the medical management of patients with ChHD. Despite the benefit shown in this study, we know that it is necessary to better evaluate the role of SGTL2 inhibitors in ChHD with large clinical trials, especially if we consider the high morbidity and mortality of this still neglected disease.
References
-
Maria CPN, Andrea B, Harry A, Caryn B, Bloger AF, et al. (2019) Chagas Cardiomyopathy: An Update of Current Clinical Knowledge and Management: A Scientific Statement From the American Heart Association. Circulation 138(12): e169-e209.
-
McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, et al. (2019) Dapagliflozin in Patients With Heart Failure and Reduced Ejection Fraction. N Engl J Med 381: 1995-2008.
-
Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, et al. (2020) Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Engl J Med 383: 1413- 1424.
-
Anker SD, Filippatos BG, Ferreira JP, Filippatos G, Bocchi E, et al. (2021) Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med 385: 1451- 1461.
-
Green CP, Porter CB, Bresnahan DR, Spertus JA (2000) Development and Evaluation of the Kansas City Cardiomyopathy Questionnaire: A New Health Status Measure for Heart Failure. J Am Coll Cardiol 35(5): 1245- 1255.
-
John AS, Philip GJ, Alexander TS, Suzanne VA (2020) Interpreting the Kansas City Cardiomyopathy Questionnaire in Clinical Trials and Clinical Care: JACC State-of-the-Art Review. J Am Coll Cardiol 76(20): 2379- 2390.
-
Giannitsi S, Bougiakli M, Bechlioulis A, Kotsia A, Michalis LK, et al. (2019) 6-Minute Walking Test: A Useful Tool in the Management of Heart Failure Patients. Ther Adv Cardiovasc Dis 13: 1753944719870084.
-
He Z, Yang L, Nie Y, Wang Y, Wang Y, et al. (2021) Effects of SGLT-2 Inhibitors on Health-Related Quality of Life and Exercise Capacity in Heart Failure Patients with Reduced Ejection Fraction: A Systematic Review and Meta-Analysis. Int J Cardiol 345: 83-88.
-
Velasco A, Morillo CA (2018) Chagas heart disease: A contemporary review. J Nucl Cardiol 27(2): 445-451.
-
Lopaschuk GD, Verma S (2020) Mechanisms of Cardiovascular Benefits of Sodium Glucose Co- Transporter 2 (SGLT2) Inhibitors: A State-of-the-Art Review. JACC Basic Transl Sci 5(6): 632-644.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study