Prevalence of Antibiotic Resistant Bacteria in Urine Culture from Two Medical Laboratories in Benghazi
Background: Urinary tract infection is the most common bacterial infection and is the second after respiratory tract infection in antibiotic prescription. The treatment of UTI is becoming difficult because of the increasing drug resistance against the common bacteria associated with UTI. Objective: This study aimed to determine the bacteria, and their antimicrobial drug resistance, associated with UTI in the Libyan population in the city of Benghazi. Materials and Methods: We performed a retrospective analysis of data of urine culture (2019 -2020) taken from two Medical Laboratories in Benghazi. A total of 1031 urine samples; 318 male, 713 females were analyzed. Result: In this study, Escherichia coli was the most prevalent bacterial uropathogen with (59.84%), followed by Klebsiella pneumoniae (11.58%) and pseudomonas aeruginosa (10%). Then, Proteus and streptococcus pneumoniae had the same prevalence value (3.86%), Enterococcus faecalis (2.7%), and Staphylococcus aureus (2.3%). Neisseria gonorrhea had the lowest (.038). Furthermore, E coli is highly resistance to imipenem, nalidixic acid and nitrofurantoin, and Klebsiella pneumoniae is highly resistance to, imipenem, nitrofurantoin, levofloxacin and ciprofloxacin, pseudomonas is resistance to imipenem, levofloxacin, and ciprofloxacin, proteus mirabilis is resistance to nitrofurantoin, Augmentin and gentamicin. Antibiotics purchasing without prescriptions remains a major problem in Libya. Based on these findings, we recommend appropriate initiatives to monitor and control the use of antibiotics.
Introduction
The most common bacterial infection in human is urinary tract infection (UTI) and it is second to upper respiratory tract infection in antibiotic prescription [1, 2]. The UTI can be urethritis, cystitis, or pyelonephritis. If lower UTI is not well controlled, it may result in pyelonephritis, prostatitis, epididymo-orchitis or dangerous urosepsis. UTI can be classified as uncomplicated when it occurs in non-pregnant healthy ladies, whereas all others are known as complicated including cystitis in male patients [3].
More than half of all healthy women will experience one attack of UTI in their lifetime. UTI is one of the most common nosocomial infections, most likely because of catheterization of the bladder. UTI is more common in males than females in newborn age; however it becomes more in female latter in childhood and adulthood. However, after the age of 65 the incidence remains equal for both sexes. Gram negative bacteria are the most common cause; namely Escherichia coli and klebsiella pneumonia [2]. Recurrent UTI is defined as three or more infection during a 12-month period and it contribute largely to the incidence and morbidity of UTI, as more than 30% of women will experience a subsequent infection within one year of resolution of their initial symptoms, despite appropriate antibiotic therapy [4, 5].
According to The Global Prevalence Study on Infections in Urology, 9.4% urological patients admitted to hospitals between 2005 and 2013 developed UTI during their hospital stay [6]. The economic burden for primary UTI diagnosis costs around $2.8 billion every year in USA, and 7 million doctor visits and around one million emergency visits annually [7]. Individual risk that can make patients mor prone to develop UTI depends on different factors such as age, sexual activity, family history, medical comorbidities as diabetes mellitus and an individual history of previous UTI [8]. The emergence of antibiotic resistant bacteria led health authority in UK to reduce antibiotic use in primary care. Around 30% of Escherichia coli are now resistant to Trimethoprim [9].
The antibiotic stewardship has an important role in controlling the spread of multi-drug resistant organisms for example a study from South Korea has indicated that a reduction in the incidence of extended-spectrum β-lactamase producing klebsiella pneumoniae by enforcing electronic prescribing system for third-generation cephalosporins [10]. Antibiotic resistance (ABR) is a growing public health concern worldwide, and it is now regarded as a critical One Health issue. One Health’s interconnected domains contribute to the emergence, evolution, and spread of antibiotic-resistant microorganisms on a local and global scale, which is a significant risk factor for global health [11].
The current study was conducted in two private labs in Benghazi to estimate the prevalence of antibiotic resistant bacteria among Libyan population in Benghazi.
Materials and Methods
A retrospective study was done after getting approval from the ethical committees. The data of the sample of urine culture in two medical laboratories in Benghazi (AL Saleem and Iben sena medical laboratories) were collected. All the urine cultures were taken for a clinical indication (suspicion of infection). A total of 1031 data was analyzed in the period from 1st of January 2019 to 4th of August 2019. The data were of different age and sex. Urine collection by, clean catch midstream urine samples (MSU) were collected in sterile disposable containers (20 mL) with tight-fitting lid to prevent leakage. The collected urine specimens were subjected to general urine examinations using direct microscopy for white blood cells (WBCs) counting, then cultured on 5% Blood agar, MacConkey agar, and Eosin-Methylene blue (EMB) agar using calibrated loops for semi-quantitative method [12], and incubated aerobically for 24 hours at 37°C. Cultures without any colony at the end of 24 hours incubation were further incubated for 48 hours. Samples with colony count ≥ 105 cfu/mL were considered positive isolates. Categorical variables were using the frequency and percentage. The chi- square test was used to identify difference between susceptibility proportions among Island and regions. The chi-square test for trend in proportion was used to evaluate trends in the considered statistically significant and analysis was conducted using R software version 3.5.1.
Results
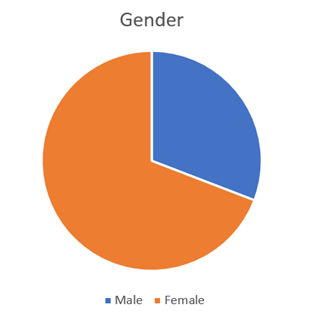
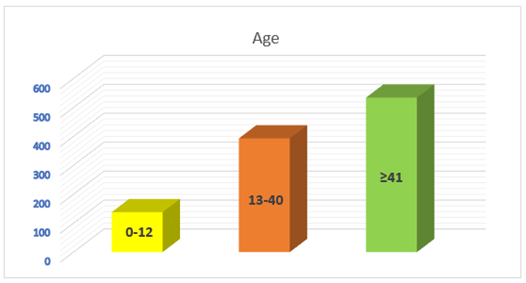
Data from one thousand and thirty-one (1031; 318 male, 713 females (Figure 1), morning clean catch midstream urine samples collected from two different laboratories in Benghazi city in Libya patients were analyzed. The samples were divided into groups according to the age; 0-12 (138), 13-40 (393), more than 41 (534) (Figure 2).
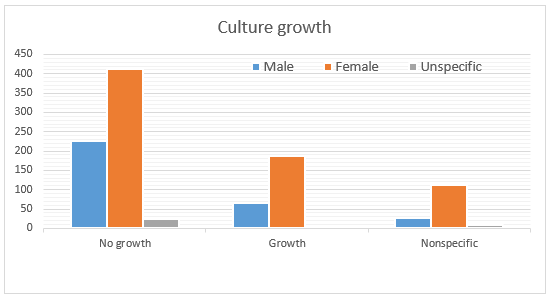
Significant bacteriuria was observed in 259/1031; 25.12%. The other samples contain either no growth (664/1031; (64.4%) or non-specific growth result (148/1031; 14.35%) (Figure 3). Urinary tract infection was highest in females with 188/259 (72.58%) as compared to 65/259; 25%) in male.
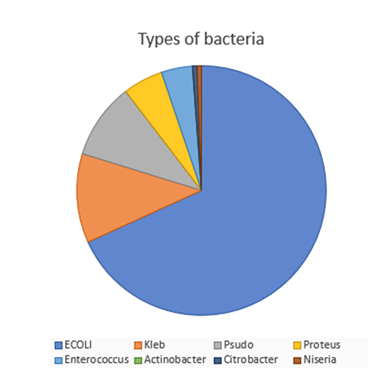
Escherichia coli was the most prevalent bacterial uropathogen with total prevalence of (59.84%; 118 in female and 31 in males), followed by Klebsiella (11.58%; 20 in females and 10 in males) and pseudomonas aeruginosa (10%; 17 in females and 9 in males). While Proteus mirabilis had the value of (3.86%; 9 in females and 1 in males). Enterococcus faecalis (2.7%; 7 in females and none in males). Only, Actinomyces isrealii was more in males (none in females and 3 in males). Corynebacterium urealyticum, Citrobacter species had a lower value (1.15%; 1 in females and 1 in males) and Neisseria gonorrhea had the lowest prevalence (0.38%; 1 in females and 0 in males) (Figure 4).
As presented in Figure 5 A, the gentamicin, amoxicillin, cefotaxim, cefotriaxone, septrin, chloramphenicol, tobramycin and pipramycin resistances of Escherichia coli were higher in several parts of Africa as compared to these antibiotics resistances of the same isolate in our study in Libya, where the Z tests were significantly different (7.9, 8.9, 7.2, 11, 9.4, 7, 18, 24.8 respectively). In contrast, the imipenem, nalidixic acid and nitrofurantoin resistances of E coli were significantly higher in Libya as compared to median percent of the same antimicrobial resistance of the same pathogen in different territories in Africa, where the Z tests were -2.1, - 2,1 and -7.5 respectively. The resistances of Escherichia coli to the other tested antibiotics as augmentin, ciprofloxacin and levofloxacin in the current study where insignificant as compared to several areas in Africa ( Z tests ranged between -2 and 2) Figure 5A.
Although the Patterns of imipenem, nitrofurantoin, levofloxacin, and ciprofloxacin resistant Klebsiella were higher in this study in Libya as compared to the patterns of the same anti-microbial resistances of Klebsiella in many countries of Africa, statistically, there were no significant differences of Z tests (-1.4, -0.7, -1 respectively) Figure 5 B. On the other hand, the other tested antibiotic resistances of Klebsiella isolates were significantly higher in parts of Africa (Z tests ranges between 2.1 as in augmantin and 20.7 as in tobramycin) Figure 5B.
In several regions of Africa, the pseudomonas aeruginosa showed to process more resistance to gentamicin, amoxicillin, cefotaxim, nalidixic acid, nitrofurantoin and septrin as compared to these antibiotic resistances of the same isolate in the current study Figure 6C. In addition, the resistant patterns of pseudomonas to imipenem, levofloxacin, and ciprofloxacin were slightly higher in the present study as compared to the mean percent of resistance in different countries in Africa, However, these were not significantly different (Z tests were -0.3, -0.9, -0.8 respectively) Figure
5C. Although the prevalence of tobramycin and Pipramycin resistant pseudomonas strains were tested (38.5 and 46.2% respectively), no comparable studies were found in many countries in Africa.
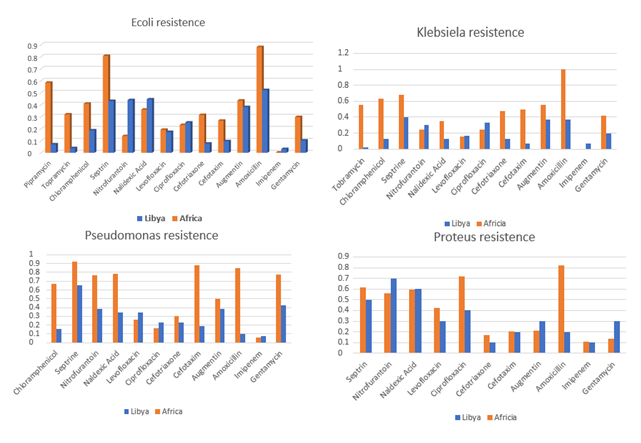
Figure 5: Percentage of several antimicrobial resistance in the most common gram negative uropathogens in Libya compared with the Median ranges of percent antimicrobial resistance for the same bacteria in Africa during 2016. A: antimicrobial resistance in Escherichia coli B: antimicrobial resistance in Klebsiella pneumoniae. C: antimicrobial resistance in Pseudomonas aeruginosa. D: antimicrobial resistance in Proteus mirabilis.
As revealed in the figure 5D, the nitrofurantoin, Augmentin and gentamicin resistant Proteus pathogens were more prevalent in our country in this study as compared to median percent of the same antibiotic resistance for the Proteus in different parts of Africa. However, these were not significantly different (Z test = -1.5, -0.9, -1.8 respectively). The percentages of Proteus resistant strains against amoxicillin and ciprofloxacin were significantly lower in the current study as compare to that in many countries in Africa (Z tests= 7.9, 3.3 respectively) Figure 5D.
Discussion
Antibiotic resistance is a real problem in our country due to misuse of antibiotic which were frequently prescribed even for simple upper respiratory tract infection without prescription, antibiotic resistance among uropathogens is common worldwide. In our country no enough data found on antibiotic resistance so in this study we tried to shed light on the prevalence of antibiotic resistant in urine samples [13, 14]. One thousand and thirty one (103; 318 male, 713 females cases). Anatomical factors and alterations also play an important role in the pathogenesis of UTI in women. The shortness of the urethra, with its close relationship to the anus, makes it easy for bacteria to ascend into the urinary tract [15].
In our study urinary tract infection was highest in females with 188/259 (72.58%) as compared to 65/259; 25%) in male. This is in agreement with study in Bushra
medical laboratory, Tripoli, Libya who found the prevalence of significant bacteriuria was 20.4% (291/1423), among them 81.4% (237/291) were females and 18.6% (54/291) were males [16]. Also in support of our results study done in a rural community of Odisha, India. The finding showed that females (45.2%) had higher prevalence of UTI in comparison with males (18.4%) [17].
Furthermore, in accordance with our results study done in Iran showed that the frequency of UTI was significantly higher in girls (70.3%) than in boys [18]. UTI was more common in age group <41 years (534) then 13-40 (393) and 0-12 (138) this is in accordance with previous study done in Iraq. The study found that 58.4% of participants belonged to 21-30-year age group followed by 26% who belonged to 31-40-year age group. 48.4% of the study participants were illiterate [19].
In our paper, Escherichia coli was the most prevalent bacterial uropathogen with (59.84%), followed by Klebsiella pneumoniae (11.58%) and pseudomonas aeruginosa (10%). Then, Proteus and streptococcus pneumoniae had the same prevalence value (3.86%), Enterococcus faecalis (2.7%), and Staphylococcus aureus (2.3%). Actinomyces isrealii, Corynebacterium urealyticum, Citrobacter species had a lower value (1.15%) and Neisseria gonorrhoea had the lowest (0.38%). This is in agreement with previous study in 2010 Escherichia coli was the most common cause of urinary tract infection (62.88%), the second most common was Klebsiella (23.080/%), followed by Proteus mirabilis (7.02%), Citrobacter (5.35%), Staphylococcus saprophyticus (1.34%) and Candida albicans (0.33%) [20]. Also, in support of our results study conducted in patients attending hospitals in Bushenyi district western Uganda by Odoki and others, a significantly high prevalence of E. coli 41.9% was reported [21].
In another study in Colorado Escherichia coli (72%) and (Klebsiella species (12%) [22]. In our paper E coli is highly resistance to imipenem, nalidixic acid and nitrofurantoin resistances of E coli were significantly higher in Libya as compared to Africa this is in accordance with study done in Iran. The results of this study showed that the highest resistance rate was against nalidixic acid (74.4%) and trimethoprim/sulfamethoxazole (69.8%) [23]. In contrast another study showed that of these 119 E. coli isolates, 91 (76.51%) were multi drug resistant (MDR). The isolates showed high levels of resistance to ampicillin (88.4%), amoxicillin-clavulanic acid (74.4%), norfloxacin (74.2%), cefuroxime (72.2%), ceftriaxone (71.4%) and co-trimoxazole (64.2%) [24].
Although the Patterns of imipenem, nitrofurantoin, levofloxacin, and ciprofloxacin resistant Klebsiella were higher in this study in Libya of as compared with Africa this is in accordance with study in central Poland K. pneumoniae were resistant to amoxicillin plus clavulanic acid (75.0%), piperacillin plus tazobactam (76.2%), cefotaxime (76.2%), cefuroxime (81.0%), ciprofloxacin (81.0%), and trimethoprim plus sulphamethoxazole (81.0%) [25] carbapenem-resistant strains are emerging worldwide. In this study in turkey Klebsiella pneumoniae, with high-level carbapenem resistance (imipenem minimum inhibitory concentration of 32 g/mL) [26]. Klebsiella is also resistance to levofloxacin and nitrofurantoin this is in accordance with study done in Romania which showed that the second most prevalent uropathogen was Klebsiella (16.93%), with the highest resistance quota to amoxicillin–clavulanic ac. (R = 28.62%), levofloxacin and nitrofurantoin (both R = 15.61%), and ceftazidime (R = 15.24%) [27].
In another study in UK,(2019). In this study the six leading pathogens for deaths associated with resistance (Escherichia coli, followed by Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa) were responsible for 929,000 (660,000–1,270,000) deaths attributable to AMR and 3.57 million (2.62–4.78) deaths associated with AMR in 2019. One pathogen–drug combination, meticillin-resistant S aureus, caused more than 100 000 deaths attributable to AMR in 2019, while six more each caused 50 000–100 000 deaths: multidrug-resistant excluding extensively drug-resistant tuberculosis, third- generation cephalosporin-resistant E coli, carbapenem- resistant A baumannii, fluoroquinolone-resistant E coli, carbapenem-resistant K pneumoniae, and third-generation cephalosporin-resistant K pneumoniae [28].
Pseudomonas is highly resistance to imipenem, levofloxacin, and ciprofloxacin this is in accordance with study done in Ethiopia.
The overall resistance rate of P. aeruginosa was higher against cephalosporins, i.e. ceftazidime (35%) and cefepime (31%), followed by fluoroquinolones, i.e. levofloxacin (24%) and ciprofloxacin (18%), then carbapenems, i.e. imipenem (18%) and meropenem (13%); the resistance rate was ceftolozane-tazobactam (9%) and piperacillin-tazobactam (16%) [29]. Another study in accordance with our results in Winnipeg, Manitoba. Showed that Ciprofloxacin-resistant P aeruginosa increased from 1.0% of all isolates in 1988 to 10.0% in 1995. A significant (P=0.05) correlation was demonstrated between the amount of ciprofloxacin use and prevalence of ciprofloxacin-resistant P aeruginosa (r=0.73, P=0.05). Imipenem-resistant P aeruginosa increased from 1.0% of isolates in 1987 to a maximum of 10.4% in 1991, and subsequently decreased to 5.4% in 1995. Imipenem use and the prevalence of imipenem-resistant P aeruginosa were significantly correlated (r=0.85, P=0.014) [30]. In our study Proteus is resistance to nitrofurantoin, augmentin and gentamicin this is in accordance with the study in the hospitals of Kharkov of the antibiotic response to 42 Proteus strains isolated from different sources. Many strains were resistant to gentamicin, ampicillin and carbenicillin irrespective of the isolation source [31]. Also in support of our study another study done on strains Proteus mirabilis were isolated from urine samples from ambulatory and hospitalized patients diagnosed with urinary tract infection (UTI) between April 2008 and April 2010. Two hundred and thirteen of P. mirabilis strains were tested. Eighty-two (38.5 %) strains were resistant to ampicillin, 49 (23.0 %) to cefalotin, 83 (39.0 %) to sulfamethoxazole/ trimetoprim, 75 (35.2 %) to ciprofloxacin, 95 (44.6 %) to oxolinic acid, 54 (25.4 %) to gentamicin, and 72 (33.8 %) to chloramphenicol. There was significantly lower resistance to cefotaxime - 8 strains (3.8 %), ceftazidime - 8 (3.8 %), amoxicillin/clavulanic acid 17 (8.0 %) and aztreonam - 8 (3.8 %) [32].
Furthermore in support of our study another paper showed that proteus is resistance to tetracycline was 95% followed by nitrofurantoin (92.5%), trimethoprim/ sulfamethoxazole (75%), ciprofloxacin (45%), cefotaxime (42.5%), ofloxacin (40%), ampicillin (35%), meropenem (30%), norfloxacin (25%), cefixime and amoxicillin- clavulanate (22.5%), aztreonam and amikacin (15%), ceftazidime (7.5%), and ampicillin-sulbactam (2.5%) [33].
There are three major mechanisms by which bacteria become resistant to carbapenems: enzyme production, efflux pumps and porin mutations .Resistance to carbapenems may be attributed to three major mechanisms: porin-mediated resistance to reduce uptake of carbapenems, efflux pumps, which pump the carbapenem outside the cells and enzyme- mediated resistance which is mediated via the acquisition of carbapenemase genes. The reduced uptake or increased efflux of antibiotics are usually associated with an overexpression of β-lactamases possessing weak affinities for carbapenems [34, 35]. The nature of the resistance determinants can affect the dynamics of their spread [36]. Fluoroquinoloe resistance is due to one or more point mutation in quinolole binding region of the target enzyme or to a change in the permeability of the organism [37]. Nitrofurantion resistance is mainly mediated by mutations in nfsA and/or nfsB, both of which encode oxygen-insensitive nitroreductases responsible for high-level nitrofurantoin resistance (NFT-R; median MIC of 96 μg/ml) [13]. These mutations hinder the reduction of NFT, preventing the formation of toxic intermediate compounds. Resistance to nitrofurantoin may be chromosomal or plasmid-mediated and involves inhibition of nitrofuran reductase [38].
References
-
Aabenhus R, Hansen MP, Siersma V, Bjerrum L (2017) Clinical Indications for Antibiotic Use in Danish General Practice: Results from a Nationwide Electronic Prescription Database. Scand J Prim Health Care 35(2): 162-169.
-
Goldman L, Schafer A (2020) Goldman-Cecil medicine. 26th (Edn.). Philadelphia, PA: Elsevier. pp: 1836-1837.
-
Wagenlehner FME, Bjerklund Johansen TE, Cai T, Koves B, Kranz J, et al. (2020) Epidemiology, Definition and Treatment of Complicated Urinary Tract Infections. Nat Rev Urol 17(10): 586-600.
-
Epp A, Larochelle A (2010) Recurrent Urinary Tract Infection. J Obstet Gynaecol Can 32(11): 1082-1090.
-
Foxman B (2014) Urinary Tract Infection Syndromes: Occurrence, Recurrence, Bacteriology, Risk Factors, and Disease Burden. Infect. Dis Clin North Am 28(1): 1-13.
-
Tandogdu Z, Cek M, Wagenlehner F, Naber K, Tenke P, et al. (2014) Resistance Patterns of Nosocomial Urinary Tract Infections in Urology Departments: 8-Year Results of the Global Prevalence of Infections in Urology Study. World J Urol 32(3): 791-801.
-
Simmering JE, Tang F, Cavanaugh JE, Polgreen LA, Polgreen PM (2017) The Increase in Hospitalizations for Urinary Tract Infections and the Associated Costs in the United States, 1998–2011. Open Forum Infect Dis 4(1): 281.
-
Scholes D, Hooton TM, Roberts PL, Stapleton AE, Gupta K, et al. (2000) Risk Factors for Recurrent Urinary Tract Infection in Young Women. J Infect Dis 182(4): 1177- 1182.
-
Gharbi M, Drysdale JH, Lishman H, Goudie R, Molokhia M, et al . (2019) Antibiotic Management of Urinary Tract Infection in the Elderly in Primary Care and Its Association with Bloodstream Infections and All-Cause Mortality: A Population-Based Cohort Study. BMJ 364: l525.
-
Kim JY, Sohn JW, Park DW, Yoon YK, Kim YM, et al. (2008) Control of Extended-Spectrum {Beta}-Lactamase- Producing Klebsiella Pneumoniae Using a Computer- Assisted Management Program to Restrict Third- Generation Cephalosporin Use. J Antimicrob Chemother 62(2): 416-421.
-
Aslam B, Khurshid M, Arshad MI, Muzammil S, Rasool M, et al. (2021) Antibiotic Resistance: One Health One World Outlook. Front Cell Infect Microbiol 11: 771510.
-
Fallon D, Andrews N, Frodsham D, Gee B, Howe S, et al. (2002) A Comparison of the Performance of Cystine Lactose Electrolyte Deficient (CLED) Agar with Oxoid Chromogenic Urinary Tract Infection (CUTI) Medium for the Isolation and Presumptive Identification of Organisms from Urine. J Clin Pathol 55(7): 524-529.
-
Clinical pharmacy and therapeutics by Roger Walker, Clive Edwards. 3rd (Edn.), pp: 503-511.
-
Applied therapeutics the clinical use of drugs by Mary Anne konda-kimble. 8th (Edn.), pp: 456-465.
-
Yamamoto S, Tsukamoto T, Terai A, Kurazono H, Takeda Y, et al. (1997) Genetic Evidence Supporting the Fecal- Perineal-Urethral Hypothesis in Cystitis Caused by Escherichia Coli. J Urol 157(3): 1127-1129.
-
Salem MA, Ahmed FA (2018) Bacterial Profile of Urinary Tract Infection and Antimicrobial Susceptibility Pattern Among Patients Attending at Bushra Medical Laboratory, Tripoli, Libya. Journal of Gastroenterology and Hepatology Research 7(4): 2671-2675.
-
Sood S, Gupta R (2012) Antibiotic Resistance Pattern of Community Acquired Uropathogens at a Tertiary Care Hospital in Jaipur, Rajasthan. Indian J Community Med 37(1): 39-44.
-
Pouladfar G, Basiratnia M, Anvarinejad M, Abbasi P, Amirmoezi F, et al. (2017) The Antibiotic Susceptibility Patterns of Uropathogens among Children with Urinary Tract Infection in Shiraz. Medicine (Baltimore) 96(37): e7834.
-
Salwa Al-Mukhtar (2018) Urinary Tract Infection Among Women Aged (18-40) Years Old in Kirkuk City, Iraq. The Open Nursing journal 12: 248-254.
-
Behzadi P, Behzadi E, Yazdanbod H, Aghapour R, Akbari Cheshmeh M (2010) A Survey on Urinary Tract Infections Associated with the Three Most Common Uropathogenic Bacteria. Maedica (Bucur) 5(2): 111-115.
-
Mladenović J, Veljović M, Udovicić I, Lazić S, Segrt Z, et al. (2015) Catheter Associated Urinary Tract Infection in a Surgical Intensive Care Unit. Vojnosanitetski Pregled 72(10): 883-888.
-
Michael LW, Loretta G (2004) Laboratory Diagnosis of Urinary Tract Infections in Adult Patients. Clinical Infectious Diseases 38(8): 1150-1158.
-
Haghighatpanah M, Mojtahedi A (2019) Characterization of Antibiotic Resistance and Virulence Factors of Escherichia Coli Strains Isolated from Iranian Inpatients with Urinary Tract Infections. Infect Drug Resist 12: 2747-2754.
-
Niranjan V, Malini A (2014) Antimicrobial Resistance Pattern in Escherichia Coli Causing Urinary Tract Infection among Inpatients. Indian J Med Res 139(6): 945-948.
-
Barbara K, Agata G, Piotr S, Jolanta W, Urszula P (2021) Antibiotic Resistance of Uropathogens Isolated from Patients Hospitalized in District Hospital in Central Poland in 2020. Antibiotics (Basel) 10(4): 447.
-
Gülmez D, Woodford N, Palepou MF, Mushtaq S, Metan G (2008) Carbapenem-Resistant Escherichia Coli and Klebsiella Pneumoniae Isolates from Turkey with OXA- 48-Like Carbapenemases and Outer Membrane Protein Loss. Int J Antimicrob Agents 31(6): 523-526.
-
Petca RC, Mareș C, Petca A, Negoiță S, Popescu RI, et al. (2020) Spectrum and Antibiotic Resistance of Uropathogens in Romanian Females. Antibiotics (Basel) 9(8): 472.
-
Addis T, Araya S, Desta K (2021) Occurrence of Multiple, Extensive and Pan Drug-Resistant Pseudomonas aeruginosa and Carbapenemase Production from Presumptive Isolates Stored in a Biobank at Ethiopian Public Health Institute. Infect Drug Resist 14: 3609- 3618.
-
Mohsen Naghavi (2022) Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Antimicrobial Resistance Collaborators 399: 629-655.
-
Zhanel GG, Nicolle LE, Gin AS, Karlowsky J, Kabani A, et al. (1998) Ciprofloxacin or Imipenem Use Correlates with Resistance in Pseudomonas Aeruginosa. Can J Infect Dis 9(6): 382-386.
-
Ekowska A, Janicka G, Wróblewska J, Kruszyńska E (2004) Prevalence of Proteus Mirabilis Strains in Clinical Specimens and Evaluation of their Resistance to Selected Antibiotics. Pol Merkur Lekarski 17(101): 538-540.
-
Cernohorská L, Chvílová E (2011) Proteus Mirabilis Isolated from Urine, Resistance to Antibiotics and Biofilm Formation. Clin Microbial Infect 17(3): 81-85.
-
Mirzaei A, Nasr Esfahani B, Raz A, Ghanadian M, Moghim S (2021) From the Urinary Catheter to the Prevalence of Three Classes of Integrons, β-Lactamase Genes, and Differences in Antimicrobial Susceptibility of Proteus mirabilis and Clonal Relatedness with Rep-PCR. Biomed Res Int 995-2769.
-
Yang D, Guo Y, Zhang Z (2009) Combined Porin Loss And Extended Spectrum Β-Lactamase Production is Associated with an Increasing Imipenem Minimal Inhibitory Concentration in Clinical Klebsiella Pneumoniae Strains. Curr Microbiol 58(4): 366-370.
-
Logan LK , Weinstein RA (2017) The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J Infect Dis 215(1): S28-S36.
-
Little ML, Qin X, Zerr DM, Weissman SJ (2012) Molecular Diversity in Mechanisms of Carbapenem Resistance in Paediatric Enterobacteriaceae. Int J Antimicrob Agents 39(1): 52-57.
-
Laura JV (1998) Fluoroquinolone resistance: Overuse of Fluoroquinolones in Human and Veterinary Medicine can Breed Resistance. BMJ 317(7165): 1029-1030.
-
Sandegren L, Lindqvist A, Kahlmeter G, Andersson DI (2008) Andersson Nitrofurantoin Resistance Mechanism and Fitness Cost In Escherichia Coli. J Antimicrob Chemother 62(3): 495-503.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study