Difloxacin Disposition and Residues in Broiler Chickens
Difloxacin disposition in broiler chickens was studied, with the objective of establishing pharmacokinetic parameters in plasma and tissues and estimating a withdrawal period. Forty-two adult chickens were divided into 14 groups of 3 individuals each, which received a 10 mg/kg single oral dose of difloxacin after a period of fasting between 12 hours before and 3 hours after administration. Each batch was sacrificed at pre-established times, and blood, muscle lung, liver, skin and kidney samples were obtained in a period up to 120 hours post application. Assay consisted in the extraction of the analyte, its separation and quantification by high performance liquid chromatography (HPLC). Mean plasma and tissue concentrations of difloxacin by time were analyzed with the PK Solution software. Oral application determines rapid absorption, moderate plasmatic permanence and extensive tissue distribution. The analysis of residual concentrations in tissues using WT 1.4 software calculated the withdrawal period, based on maximum residue limits (MRL) of 300, 1900, 400, 600 and 300 µg/kg, established for muscle, liver, skin, kidney and lung, respectively, a withdrawal period of 3 days is estimated for muscle, liver and skin and 5 days for kidney and lung.
Introduction
Fluoroquinolones are synthetic agents with optimal activity against Enterobacteria spp. and Pseudomonas aeruginosa, moderate activity against Staphylococci spp., and good activity against Chlamydia spp. and Mycoplasmas spp. [1, 2, 3, 4]. They exert concentration-dependent bactericidal activity blocking the enzymes DNA gyrase and topoisomerase IV, involved in the folding of the DNA double helix, essential for the three-dimensional structure of genetic material [1, 3, 4].
These antimicrobials have pharmacokinetic properties that allow their application in drinking water [5, 6], provide variable oral absorption in birds [3, 6], significant tissue concentrations with respect to plasma as a result of their amphoteric character and reduced affinity for plasma proteins [1, 3, 4] and exhibit a reduced toxicological profile in birds [6] and other domestic species [2, 3].
Difloxacin is a synthetic quinolone derived from pefloxacin with a pKa of 6.1-7.5 [7]. It has extensive antimicrobial activity on Gram-negative and positive bacteria such as Staphylococcus aureus, Streptococcus spp, [8]. The incorporation of a second fluorine atom in its structure influences its antibacterial potency [4].
Background information on oral application of difloxacin in chickens, indicates prompt absorption [8, 9, 10], determined by absorption half-life of 1.4 hours and a Tmax obtained at 2.6 hours. Oral bioavailability of difloxacin is moderate [9, 10], plasma retention is short, according to reported t½β values of 1.8 [10], 3.7 [10] 7 [8] 8 [11] and 12 hours [9] and MRT of 5.6 hours [10].
The administration of difloxacin in broiler chickens was promoted due to its microbiological characteristics, reduced tissue permanence and limited withdrawal periods [10, 12]. Other trials report significant tissue concentrations 72 hours after application in lung, liver and kidney and lower in muscle [9, 13]. The highest tissue concentrations are verified in the kidney, followed in decreasing order by liver and muscle [9, 13]. These results imply storage periods of 5 days [9].
Fluoroquinolone administration in production animals was reflected in an increased incidence of resistant strains of Campylobacter spp., associated with excessive and inadequate administration and by the presence of tissue residues [14, 15]. This situation determined restrictions in its employment, the determination of maximum residue limits (MRL) in edible tissues and the implementation of withdrawal periods [9, 14, 16].
In this context, a population pharmacokinetic study was carried out, replacing traditional designs that use few animals [16, 17, 18], with the aim of establishing plasma concentrations and in edible tissues, after single oral administration of difloxacin to estimate kinetic parameters that allow assessing its use, therapeutic utility and, with tissue depletion data, to establish a withdrawal period to slaughter [16].
Material and Methods
Animals
As experimental subjects, 42 mixed broiler chickens (n= 42) were used, Ross line, clinically healthy; vaccinated against Marek, Newcastle, Gumboro and Infectious bronchitis; birds were randomly selected from a population of 4000 chickens belonging to a commercial poultry farm near the city of Río Cuarto.
At the beginning of the experience the birds were 30 days old and an average weight of 1.96 ± 0.23 Kg. The birds, subject to identical handling and feeding conditions, were housed in appropriate environmental conditions for the age of the animals: forced ventilation, light plan of 18 total hours, conditioned room temperature between 19 and 21°C and 65% average humidity, water ad libitum and balanced feed free of growth promoters and coccidiostats.
After a week of acclimatization, birds were weighed individually and randomly formed into 14 batches of 3 individuals each. Each batch was identified and after fasting for 24 hours and 3 hours after application, each animal received a single dose of 10 mg/Kg of the commercial solution of difloxacin applied directly as a bolus in the oral cavity.
After administration of the antimicrobial, each batch was sacrificed by exsanguination at the following times: 0.33, 0.66, 1, 2, 3, 4, 6, 8, 12, 24, 48, 72, 96 and 120 hours, after stunning according to the procedure established by the World Organization for Animal Health (OIE) in the Terrestrial Animal Health Code [19] adopted in establishments authorized for the slaughter of birds and accepted by in articles 8.3 of Directive 86/609 of the European Economic Community [20].
From each animal, 5 ml of blood were obtained in heparinized tubes that were immediately centrifuged for 10 minutes at 2500 rpm and 3 grams of skin, muscle, kidney, liver and lung. Plasma and tissue samples obtained from each animal were identified and stored in separate vials until analysis at -20°C.
Solutions
Stock solutions of difloxacin (Guobang Pharma Laboratory, China, 98% purity) and enrofloxacin (Chile Laboratory, 99.9% purity) in methanol (Baker Laboratory) were prepared in 100 mL volumetric flasks to obtain a concentration of 100 mg/mL. Solutions were subject to ultrasound for 10 minutes to ensure complete dissolution and were kept protected from light at room temperature.
From the stock solutions, daily dilutions in deionized water were prepared and used for calibration and recoverability standards. Mobile phase was prepared with deionized water, acetonitrile (Baker Laboratory) and triethylamine (Sintorgan Laboratory), in proportion (79:19:1 v/v/v) respectively, adjusted to pH 3.0 with orthophosphoric acid (Sintorgan Laboratory) and filtered with a 0.22 µ nylon filter using a vacuum pump. Homogenization solution was constituted by deionized water, methanol, 70% perchloric acid and phosphoric acid (500:500:10:1 v/v/v/v), respectively [21].
Sample Treatment
In plasma, the preparative assay consisted of extracting the analyte using 200 μL of plasma, 200 μL of deionized water, 750 μL of homogenizing solution, 50 μL of tricloacetic acid (25%), and a 5 μg/mL enrofloxacin solution. as internal standard. The whole was vortexed for 30 seconds and centrifuged at 13,500 rpm at 4°C for 25 minutes [21].
Supernatant was filtered with a 0.22 μ nylon filter and 100 μL of it, were used as sample injection volume for its separation and quantification by HPLC. In the tissues, 200 mg of sample (skin, muscle, kidney, liver or lung) were added to identical solutions as the plasma, then mechanically homogenized for 5 minutes, remaining at rest for 20 minutes at room temperature and then kept in refrigeration for 12 hours at 4°C and finally, subjected to vortex for 5 minutes and centrifuged at 13500 rpm for 25 minutes, supernatant was filtered through 0.22 µm nylon filters and 100 µL of the supernatant was injected for its separation and quantification by HPLC [21].
Separation and Quantification
Separation and quantification were carried out at room temperature by HPLC (Hewlett Packard), by means of reverse phase isocratic elution at 0.8 mL/minute flow, using an octadecylsilane C-18 column, 5 μ, 25 cm, Phenomenex pre- column, injection syringe Hamilton of 100 μL and reading in a fluorescence detector established at 295 nm of excitation and 490 nm of emission [22]. The elution generates peaks in the chromatogram corresponding to the analyte under study, difloxacin, and the internal standard enrofloxacin.
Concentration Calculation
From the areas under the curve observed in the chromatograms, which reflect the analyte under study and the internal standard, a quotient of the division of both (y) was determined, and using the slope (b) from the calibration curve and intercept (a) obtained from the linearity study, a simple and transformed linear function was performed to determine the concentration of the analyte under study (x) in plasma and each tissue [22]: x=(y-a)/b
Validation Tests
The validation of the chromatographic technique was carried out by linearity (L), recoverability (%R), detection limit (LD), quantification limit (LC), reproducibility (RR) and repeatability (RR) tests. These tests, and the determination of the concentration of the analyte in the problem samples, were carried out on the area index, resulting from the division of the areas of the difloxacin chromatographic signals and the internal standard, enrofloxacin. The L was determined by adjusting the area index values and their respective calibration standards to a linear regression line between both variables, accepting correlation coefficients (r2) ≥ 0.99. The relative %R was established according to the variation experienced by the concentration of the analyte under study, when the sample is subjected to extraction through the elution of three calibration standards and three recoverability standards. At each concentration, it was estimated with the formula: %R= (calibration area index/recoverability area index) x 100. The LD was calculated according to the EMEA [26]: LD= 3.3 (k) x DS/β. Where is average DS the standard deviation of the response and β is the value of the slope in the calibration curve. The LC was calculated with the same formula and values, except that K is 10. The RR was estimated by six-fold elution of the calibration standards, and it was acceptable if the coefficient of variation (CV) between elutions, in terms of time of retention, and peak area in the chromatograms was ≤1.5%. The rr is established by eluting the calibration standards on six different days, and was acceptable if the CV was ≤ 3% [25, 26, 27].
Pharmacokinetic Analysis
From the samples obtained in plasma and each tissue under study (skin, muscle, liver, lung and kidney) the average concentrations of difloxacin were obtained as a function of time up to 24 hours post application. The entry of data in the non-compartmental program Pk Solution 2.0 [27], in addition to the average weight of the birds and the dose used, allowed us to estimate robust kinetic parameters of difloxacin for plasma and each tissue, essential to assess the disposition of difloxacin in the body: peak concentration (Cmax), time to peak concentration (Tmax), absorption half-life (t½abs), distribution half-life (t½α), elimination half-life (t½β), area under the curve (AUC) and mean residence time (MRT) [27].
Withdrawal Period Calculation
EMEA WT 1.4 software [24] with 99% confidence was used to estimate the withdrawal period, by entering the MRLs for difloxacin established by the Committee for Veterinary Medicinal Products in EMEA/MRL/819/02- FINAL (Difloxacin) that determines in chicken muscle, liver, skin, kidney 300, 1900, 400 and 600 µg/Kg, respectively, while for lung 300 µg/Kg safest MRL was selected. For the calculation, concentrations obtained from 8 to 120 hours post application, from each animal were used (16.24).
Results
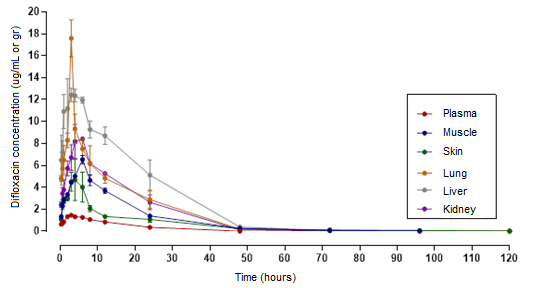
Regarding the validation of the analytical technique implemented, Table 1 indicates results of the linearity tests, recoverability percentages and variation coefficients percentages (CV), established in repeatability and reproducibility tests and the limits of detection and quantification in plasma and each tissue [26]. Figure 1 shows the plasma and tissue disposition curves obtained by the mean concentrations (±SD) after a single oral application of 10 mg/Kg of difloxacin.
The results of the different robust pharmacokinetic
parameters provided by the non compartimental PK Solution 2.0 software [27], derived from the analysis of the average concentrations of each tissue at different times after the application of difloxacin are shown in Table 2 and the analysis of the residual concentrations versus time with the EMEA WT 1.4 program [24] allowed estimating a withdrawal period of 3 days for muscle, liver and skin and 5 days for kidney and lung.
| L (r2) | %cv rr | % cv RR | LD * | LC * | % R | |
|---|---|---|---|---|---|---|
| Plasma | 0,999 | 0,3 ± 0,1 | 1,7 ± 0,9 | 0,006 | 0,019 | 98,2 ± 0,7 |
| Muscle | 0,999 | 1,4 ± 0,7 | 2,8 ± 0,4 | 0,006 | 0,017 | 92,7 ± 0,8 |
| Liver | 0,999 | 0,6 ± 0,2 | 1,5 ± 0,7 | 0,005 | 0,018 | 93,8 ± 0,4 |
| Skin | 0,999 | 1,5 ± 0,2 | 2,3 ± 0,9 | 0,006 | 0,018 | 96,3 ± 0,2 |
| Kidney | 0,999 | 0,7 ± 0,3 | 1,8 ± 1,1 | 0,001 | 0,005 | 95,3 ± 0,3 |
| Lung | 0,999 | 1,7 ± 1,3 | 1,9 ± 1,1 | 0,001 | 0,004 | 95,1 ± 1,1 |
Table 1: Validation of difloxacin in plasma and tissues of broiler chickens. * (µg/gr o µg/mL, as appropriate)
| Plasma | Muscle | Skin | Liver | Kidney | Lung | |
|---|---|---|---|---|---|---|
| Cmax(μg/mL o μg/g) | 1.5 | 6.5 | 4.7 | 13 | 8.4 | 17.6 |
| Tmax(h) | 3 | 6 | 4 | 3 | 4 | 3 |
| t1/2abs(ing)(h) | 1,04 | 1,57 | 1,66 | 0,67 | 0,72 | 0,85 |
| t1/2α(h) | 1,21 | - | - | - | - | - |
| t1/2b(h) | 10,16 | 9,04 | 15,64 | 15,98 | 11,54 | 14,9 |
| AUCarea(μg-h/mL) | 25,7 | 101,4 | 82,1 | 32,8 | 166,3 | 199,2 |
| MRT(h) | 15,3 | 14,5 | 23,5 | 23,6 | 18,1 | 20,4 |
| Cmaxtissue/plasma | - | 4,33 | 3,1 | 8,6 | 5,6 | 11,7 |
| AUCtissue/plasma | - | 3,9 | 3,1 | 12,5 | 6,4 | 7,7 |
Table 2: Plasma and tissue pharmacokinetic parameters of difloxacin in broiler chickens, orally (10 mg/kg). References: Cmax= max
Table 2: Plasma and tissue pharmacokinetic parameters of difloxacin in broiler chickens, orally (10 mg/kg). References: Cmax= maximum concentration reached; Tmax= time when Cmax is achieved; t½ abs (ing): absorption or intake half-life, t½β: elimination half-life; t½α= distribution half-life; AUCarea= area under the curve; MRT= mean residence time; AUCtissue/plasma= Differentiation quotient between area under the curve of tissue and plasma.
Discussion
No adverse effects were observed in treated animals, consistent with the safety history of difloxacin and the group of fluoroquinolones when administered under recommended conditions [2, 3, 6].
The population design used surpasses the traditional one, that requires a reduced number of animals and avoids variations attributable to size, sex, pathologies or nutritional factors and provides data closer to real situations and is appropriate to establish the disposition of difloxacin in broiler chickens after single oral administration of 10 mg/kg, based on the average temporary concentrations in plasma and tissues [16, 17, 18].
Triethylamine inclution in mobile phase avoids the competition that fluoroquinolones present with residual groups (silanol), increases the sharpness of the peaks and avoids chromatographic tails [21]. In addition, the acidic pH improves the fluorescence intensity of fluoroquinolones [27].
The method is sensitive for kinetic studies of antimicrobial disposition in plasma and tissues and establishing residual levels, with low cost and very versatile since it adapts to different matrix, where fluorometric detection provides sensitivity and specificity [27, 28, 29].
Difloxacin disposition curves were adequately interpreted using the PK Solution 2.0 pharmacokinetic software, which allowed the calculation of robust kinetic parameters with high correlation coefficients (r2) in the linearity tests [27].
Oral administration denotes a rapid absorption process expressed by an income half-life of 1.04 hours, an intermediate value between the 1.46 hours [10, 11] and 0.73 and 0.53 hours by other studies [9, 29]. Quick dissolution in the intestinal environment results in immediate plasma levels after oral application [4]. Although fasting prior to the administration of difloxacin also influences, not only to avoid interference with food divalent cations [1]. The Cmax value in plasma (1.4 µg/ml) reached at 3 hours differs little from those reported [10, 29], between 2.2-2.6 hours and is lower than the Cmax is 2.3 µg/mL, reached at 1.3 hours, under similar dose conditions, previous fasting time and weight of the animals [9].
Other experiences with difloxacin show mixed results, reported Cmax reached in a longer time, without specifying if prior fasting was applied [11]. With a fasting period, reported a Cmax of 0.96 µg/mL, which was reached at 1.4 hours [8]. The differences respond to the biases introduced by individual animals, pharmaceutical factors in the formulation, sampling time and fasting conditions [9]. Elimination half-life and MRT reflects moderate permanence, lower than obtained by Anadón, et al. [9], but longer than those observed in other studies [8, 10, 11].
Difloxacin is detected in the tissues studied from 20 minutes up to 120 hours after application, except in muscle (96 hours). It originates disposition versus time curves in each tissue characterized by high levels in the first hours after administration, which decline significantly after 24 hours [9].
Anadón, et al. [9], in all cases tissue levels greatly exceed plasma levels [4]. AUC are relevant in lung decreasing in order in kidney, muscle, skin and liver, also in controversy with other studies. The extensive tissue distribution results from difloxacin pKa, being within the values of fluoroquinolones (6-8), giving them characteristics of weak organic acids, which in this range are predominantly in non-ionized form and at blood pH are sufficiently fat-soluble enough to diffuse into the tissues [7], in addition to the reduced binding to plasmatic proteins [1, 3, 4].
The results of tissue disposition are controversial with other authors, however they agree that in plasma and tissues they decrease rapidly; the residual concentrations incorporated into the EMEA WT 1.4 program [24] allowed estimating a withdrawal period of 3 days for muscle, liver and skin and 5 days for kidney and lung, results that refute the initial conception of early elimination and that validate a withdrawal period of 5 days, according to Anadón, et al. [9].
Conclusion
The methodology implemented in this study for the extraction of the analyte and subsequent elution by HPLC is simple, requires small amounts of solvent and is reliable according to the adjustments obtained in the calibration curves and the results of the method validation tests carried out in the different matrices studied.
The analytical method used is appropriate to quantify the antimicrobial in plasma and tissues after a single oral application of difloxacin. The disposition curves generated, analyzed by the non-compartmental pharmacokinetic program, yielded robust kinetic parameters in plasma and tissues that indicate prompt absorption of difloxacin after oral application, good tissue distribution and moderate permanence in the organism, results compatible with the physical-chemical characteristics. of difloxacin and similar to those provided by the group of fluoroquinolones in birds when applied orally, which support the use of this antimicrobial in the presence of sensitive microorganisms.
The tissue depletion analysis provides data for a prudent use of difloxacin in chickens, suggests a dosage schedule and a reasonably short withdrawal time, compatible with broiler production times, which guarantees safety for consumers.
References
-
Conková E, Cellárová E, VáczI P, Sabová L (2009) Quinolones from the point of view of pharmacology and veterinary indications (A review). Folia Vet 53(4): 175- 185.
-
Gupta R, Sharma K, Sharma R, Gupta D, Sachin T, et al. (2012) A review: pharmacokinetics application of fluoroquinolones. IJPPR 3(2): 650-660.
-
Papich M (2018) Fluoroquinolone Antimicrobial Drugs. Veterinary Pharmacology and Therapeutics, 20th (Edn.), In: J Riviere and M Papich (Eds.), Wiley & Sons pp: 953- 987.
-
Millanao A, Mora A, Villagra N, Bucarey S, et al. (2021) Biological effects of quinolones: a family of broad- spectrum antimicrobial agents. Molecules 26(23): 1-42.
-
Vermeulen B, De Backer P, Remon J (2002) Drug administration to poultry. Adv Drug Deliv Rev 54(6): 795-803.
-
Hofacre C (2013) Antimicrobial drug use in poultry. En: Antimicrobial therapy in veterinary medicine. 5th (Edn.), Ames: Blackwell Publishing pp: 545-553.
-
Diaz David D (2012) Comportamiento farmacocinético de la marbofloxacina en bovinos de diferentes edades y relación PK-PD frente a mastitis estafilocócicas. Tesis Doctoral. Universidad Complutense de Madrxid. España.
-
Inui T, Taira T, Matsushita T, Endo T (1998) Pharmacokinetic properties and oral bioavailabilities of difloxacin in pig and chicken. Xenobiotica 28 (9): 887- 893.
-
Anadón A, Suárez F, Martínez M, Castellano V, et al. (2011) Plasma disposition and tissue depletion of difloxacin and its metabolite sarafloxacin in the food producing animals, chickens for fattening. Food Chem Toxicol 49 (2): 441-449.
-
Mohamed H, Atta A, Darwish A, Atef M (2020) Effect of probiotics on the pharmacokinetic aspects and tissue residues of difloxacin in broiler chickens. Pak Vet J 41(2): 269-273.
-
Ding H, Yang G, Huang X, Chen Z, et al. (2008) Pharmacokinetics of difloxacin in pigs and broilers following intravenous, intramuscular, and oral single‐ dose applications. J Vet Pharmacol Therap 31(3): 200- 204.
-
EMEA (European Medicines Agency) (1995) EMEA/ MRL/029/95-Rev5. Committee for Veterinary Medicinal Products. Difloxacin-Summary Report.
-
Abdel Aziz M, El Shazly K, El-Gazar W (2005) Disposition kinetics of difloxacin in normal and experimentally infected chickens with mycoplasma gallisepticum. KVMJ 3(1): 97-113.
-
Gouvêa R, Santos F dos, Aquino M de, Pereira V de (2015) Fluoroquinolones in industrial poultry production, bacterial resistance and food residues (a review). Braz J Poult Sci 17(1): 1-10.
-
Mund M, Khanb U, Tahir U, Mustafa B, et al. (2017) Antimicrobial drug residues in poultry products and implications on public health(a review). Int J Food Prop 20(7): 1433-1446.
-
Lees P, Toutain P (2012) The role of pharmacokinetics in veterinary drug residues. Drug Test Anal 4(1): 34-39.
-
Mason S (2014) Population pharmacokinetic modeling to predict withdrawal times. Strategies for reducing drug and chemical residues in food animals, In: Baynes R & Riviere J (Eds.), New Jersey, USA, John Wiley & Sons pp: 81-94.
-
Machuca Sánchez C (2021) Estudio farmacocinético poblacional de medicamentos de interés terapéutico evaluados en la práctica clínica (examen complexivo). UTMACH, Facultad de Ciencias Químicas y de la Salud, Machala, Ecuador.
-
Organización Mundial de Sanidad Animal (OMSA, OIE) (2019) Código Sanitario para los Animales Terrestres Cap. 7.5. Sacrificio de animales. Organización Mundial de Sanidad Animal.
-
European Economic Community (1986) Article 8.3 of Directive 86/609.
-
Böttcher S, Baum H, Hoppe-Tichy T, Benz C, et al. (2001) An HPLC assay and a microbiological assay to determine levofloxacin in soft tissue, bone, bile and serum. J Pharm Biomed Anal 25(2): 197-203.
-
Nouws J, Ziv G (1976) The effect of storage at 4°C on antibiotic residues in kidney and meat tissues of dairy cows. Tijdschr Diegeneesk 101(20): 119-127.
-
Campanyó R, Granadas J, Guiteras J, Prata M. (2009) Antibiotics in food: Legislation and validation of analytical methodologies. Anal Bional Chem 395(4): 877-891.
-
EMEA (2002) Committee for Veterinary Medicinal Products. EMEA/MRL/819/02-FINAL (Difloxacin).
-
Urzúa N, Sobre Casas B, Messina M, Errecalde ME, et al. (2021) Validación de un método analítico por HPLC- FD para cuantificar difloxacina en plasma y tejidos de pollos parrilleros. Abstract XXI Jornadas de Divulgación Técnico-Científicas. Facultad de Ciencias Veterinarias. Universidad Nacional de Rosario, Argentina pp: 81-82.
-
Hekman P (1998) Wt1.4 Withdrawal time calculation program. European Agency for the Evaluation of Medicinal Products (EMEA), London.
-
EMEA. (2006) European Medicines Agency. Veterinary Medicines and Inspections. Committee for Medicinal Products for Veterinary Use (CVMP). Reflection Paper on the Use of Fluoroquinolones in Food Producing Animals in the European Union.
-
Talero-Pérez Y, Medina O, Rozo-Núñez W (2014) Técnicas analíticas contemporáneas para la identificación de residuos de sulfonamidas, quinolonas y cloranfenicol. Universitas Scientiarum 19(1): 11-28.
-
Abo El-Ela F, Radi A, El-Banna H, El-Gendy A, et al. (2014) Pharmacokinetics of difloxacin in healthy and E. coli- infected broiler chickens, Br Poult Sci 55(6): 830-836.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study