Effect of Indian Herbal Formulation on Hepatomegaly: An Evidence Based Case Report
Enlargement of the liver, or hepatomegaly, occurs due to fatty liver disease, liver abscess, hepatitis, liver fibrosis, and carcinoma. Clinical diagnosis and PET CT scan revealed hepatomegaly with abscess in a 60-year-old male patient with a history of left laparoscopic radial nephrectomy due to cancer. The patient’s blood contained somewhat elevated levels of hepatic enzymes, including gamma glutamyl transferase (γ-GT), alkaline phosphatase (AKP) and alanine transaminase (ALT), which were indicative of damage to the liver cells. Diabetes, high blood pressure, obesity, and viral hepatitis were not reported. For a period of 12 weeks, the patient consumed oral Body Revival® liquid (BR) at a dose of 5 ml on alternate days. Physical, clinical, and laboratory examinations were conducted every four weeks. The patient’s liver enzymes were found to be within normal range following a 12-week course of BR treatment, and a CT scan examination showed that the patient’s liver had neither a confluent nor an abscess. At that time, there were no signs of liver abscess, hepatomegaly, or NAFLD.The patient had a full recovery after receiving Body Revival®.
Introduction
Hepatomegaly is enlargement of the liver beyond its normal size. The most common causes of hepatomegaly include fatty liver, liver abscess, hepatitis and liver carcinoma [1]. Accumulation of excessive fat in the liver is the common denominator underlying the two most common and emerging causes of chronic liver disease, alcoholic liver disease (ALD) and non-alcoholic fatty liver disease (NAFLD), that are emerging public health issues globally [2]. NAFLD is characterised by hepatic steatosis detected by either imaging or histology without secondary causes. It spans a spectrum of the disease from non-alcoholic fatty liver to non-alcoholic steatohepatitis (NASH) and ultimately to cirrhosis and its complications. The pooled overall prevalence of NAFLD in the general population was 26.9% [3]. The prevalence of adult NAFLD in India has been reported between 6.7% and 55.1% [4]. An expanded, dysfunctional, insulin resistant adipose tissue with ectopic fat deposition and hepatic storage due to an imbalance is the hallmark of NAFLD with lipotoxicity as the primary driver of hepatocyte injury [5]. On the other hand, NASH fibrosis is associated with an excess all-cause mortality and also liver related mortality in general population [6]. Moreover, the highest incident of liver abscess observed in Asia, where rates can be as high as 21 per 100000 inhabitants per year. The common clinical symptoms of liver abscess are fever, pain in abdomen, jaundice and hepatomegaly [7]. CT scan and USG Imaging is the preferred modality to diagnose liver diseases including hepatomegaly, NAFLD, abscesses, hepatitis and liver carcinoma [8].
Herbal medicines have been widely used for the management of hepatic diseases, including hepatomegaly, NAFLD, jaundice, hepatitis and liver carcinoma. Clinical trials of single herbs, such as Crataegus pinnatifida and Salvia miltiorrhiza, are effective in treating fatty liver disease [9]. Silymarin, berberine, resveratrol, curcumin, quercetin and other polyphenols have been reported for supportive and combination therapy of liver diseases [10, 11]. In earlier studies, Indian herbal formulation Body Revival® (BR) reported for the improvement of quality of life in cancers including hepatic carcinoma [12, 13]. BR contains with 9 ingredients including water extract of Aegle marmelos fruit pulp (150 mg), Acorus calamus rhizome (175 mg), Withania somnifera root (325 mg), Blumea lacera fruit (115 mg), Rumex vesicarius whole plant (240 mg), Rubia cordifolia root (200 mg), Cucumis melo seed (200 mg), Symplocos racemosa stem bark (95 mg) and honey q.s [14]. Scientific reports confirmed that most of the ingredients of BR have hepatoprotective actions including the supportive treatment of hepatic malignancies [15]. Although, BR is available in market, but its usefulness in targeted interventions are essential to ascertain. Therefore, the therapeutic role of BR was assessed in the following evidence based case study.
Case Report
A 60-year-old man with past history of left laparoscopic radial nephrectomy due to renal cell carcinoma, diagnosed and operated before three years (Nov 9, 2020), initially presented to the medical emergency with a two-week history of nausea, vomiting, right upper quadrant abdominal pain and distension, but no documented history of hepatomegaly on physical examination, although remarkable for abdominal tenderness on palpation. After nephrectomy, Sunitinib (protein kinase inhibitor), a targeted anticancer drug was continued to impede the existing metastatic cells (if any) as treatment regimen. Preliminary clinical examination revealed an enlargement of the left supraclavicular node (Troisier sign). The patient was thoroughly examined and diagnosed. His body mass index was 24.2 kg/m2and vitals were stable and as follows: blood pressure 132/89 mm of Hg, pulse rate 88 and respiratory rate 23/min. He never consumed alcoholic and did not smoke or chewing tobacco. He was vegetarian in diet. His only medication was a proton pump inhibitor (Pantoprazole, 40 mg/day). A through blood examination reported: Hb 12.7 g/dl (14-17 g/dl), RBC 4.25 million/mm3 (4.35-5.65 million/mm3) WBC 6270/mm3 (4500-11000 per mm3), fasting glucose 112.1 mg/dl (70-80 mg/dl), PP glucose 125 mg/dl (110-120 mg/dl), albumin 35 g/l (34-54 g/l) , alanine transaminase 94 IU/l (4-36 IU/l), alkaline phosphatase 285 IU/l (44-147 IU/l), total bilirubin 1.6 mg/dl (0.1-1.2 mg/dl), gamma glutamyl transferase 122 IU/l (5-40 IU/l), lactate dehydrogenase 193.7 U/l (140-280 U/l), urea 7.9 mg/dl (6-14 mg/dl) and creatinine 1.13 mg/ dl (0.7-1.3 mg/dl). Viral hepatitis (HBsAg) serology was negative.

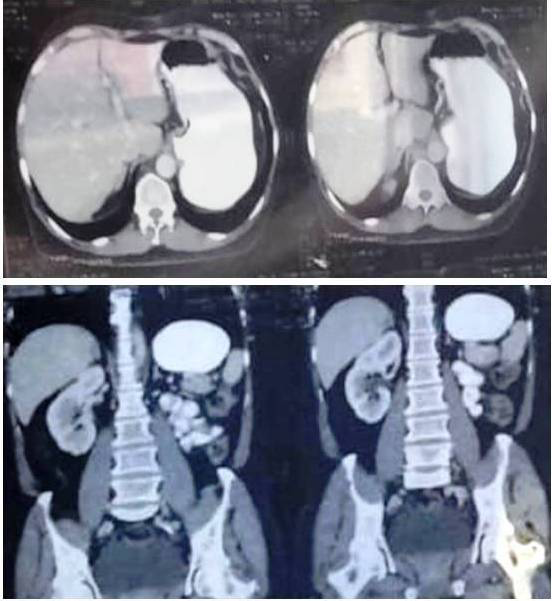
Furthermore, the patient went on to have an ultrafast multi-slice computed tomographic (CT) scan of the abdomen and pelvis after administration of oral and IV contrast and confirmed hepatomegaly and liver abscess (Figure 1). The posterior superior segment of the right lobe of liver reveals extensive confluent necrotic peripheral host oedema. The
entire confluent, measuring approximately 5.2x4x6.2 cm, extends up to the posterior capsular surface of the liver (segment 7), with immediate adjacent perihepatic inflammation and fluid. Flow within the portal vein and hepatic vein was normal. The intra-hepatic bile duct and common bile ducts were not dilated. Gall bladder was collapsed, and no CT evidence of gall bladder calculi was noted. Spleen, pancreas, and adrenals were normal in size, thickness, morphology, outline and attenuation. The right kidney was normal in size (11.9 cm), shape, outlines and revealed prompt symmetrical contrast enhancement and excretion of contrast. Urinary bladder was normal. The results of the laboratory test and clinical evaluations indicated hepatomegaly with major abscess and suggested that NAFLD or NASH would likely result if the condition was not well addressed.
Treatment
As part of his disease management regimen, the patient was instructed to apply Body Revival® liquid (BR). It is used to treat liver fibrosis, cirrhosis, NAFLD, hepatitis, and jaundice. Following the medical professional’s recommendation, the patient ingested BR orally for 12 weeks at a dose of 5 ml on alternate days. During this therapy phase, the patient received extra attention through close monitoring. Every four weeks, physical, clinical, and laboratory tests were performed. The patient was also advices to restrict and control food habits including changes to follow lifestyle.
Results
After 12 week treatment with BR, laboratory investigations of the patient blood showed haemoglobin level 13.1 g/dl, RBC count 4.4 million/mm3, leukocyte count 6500 /mm3, glucose fasting 86 mg/dl and PP 103 mg/dl, albumin 36 g/l, ALT 32 IU/l, AKP 140 IU/l, total bilirubin 0.9 mg/dl, γ-GT 36 IU/l, LDH 162 U/l, urea 7.1 mg/dl (6-14 mg/dl) and creatinine 1.11 mg/dl (0.7-1.3 mg/dl). His liver function tests were within the normal limit.
Additionally, a CT scan assessment of the pelvis and abdomen revealed that the liver’s intrahepatic vascular systems, size, and outline were all normal. There was no confluent and no abscess (Figure 2). Pericocelescystic collection was not seen. The gall bladder, common bile duct, and hepatic bile ducts were among the other hepatic structures that were found to be normal. The size, shape, and attenuation of the spleen, pancreas, adrenal glands, prostates, right kidney, and ureters were all normal. There were no indications of NAFLD, hepatomegaly, or liver abscess at the time.
Discussion
There is no direct medication available for chronic liver disease; instead, non-pharmacological treatments including a balanced diet and/or regular exercise can be helpful. However, several herbal medicines and nutritional supplements are used in complementary and alternative medicine to treat chronic liver problems, such as cirrhosis, hepatitis, hepatomegaly, and liver abscesses. It has been claimed that the components of BR perform liver protection through a variety of mechanisms, including modulating metabolisms and absorption rates, facilitating the elimination of toxic metabolites, minimizing oxidative stress and inflammation, or retrieving the activities of hepatic cells [16, 17, 18, 19, 20, 21, 22].
A recent comprehensive review elucidates the thirteen clinical trials involving herbal medicines and chronic liver illnesses, such as hepatomegaly, ascites, cirrhosis, and liver abscesses [11]. While the duration between the onset of BR and the remission of symptoms and the elimination of clinical hepatomegaly may vary from week to months. Depending on the severity of the liver disease, improvement or normalization of blood indicators could take place one to three months later. Despite achieving non-diabetic glycemic control, our patient’s glycogenic hepatopathy did not worsen in response to treatment. NAFLD can lead to fibrosis and cirrhosis, although it is typically a rather benign condition when there is no indication of non-alcoholic steatohepatitis, as in his case. However, more investigation is advised to validate the curative effects of BR in NAFLD and related hepatomegaly.
Conclusion
In this critical instance, the herbal remedy known as Body Revival contributes to the treatment of clinical hepatomegaly with abscess. Future research is expected to determine the therapeutic role of Body Revival in NAFLD.
Acknowledgement
We thank CEO of Health Reactive, Mumbai for providing the test samples.
References
-
Ghosh CK, Islam F, Ahmed E, Ghosh DK, Haque A, et al. (2012) Etiological and clinical patterns of isolated hepatomegaly at Rajshahi, Bangladesh. Euroasian J Hepato-Gastroenterol 2(1): 1-4.
-
Mitra S, De A, Chowdhury A (2020) Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Transl Gastroenterol Hepatol 5: 16.
-
Niriella MA, Ediriweera DS, Withanage MY, Darshika S, deSilva ST, et al. (2023) Prevalence and associated factors for non-alcoholic fatty liver disease among adults in the South Asian Region: A meta-analysis. Lancet Regional Health-Southeast Asia 15: 100220.
-
Shalimar, Elhence A, Bansal B, Gupta H, Anand A, et al. (2022) Prevalence of non-alcoholic fatty liver disease in India: A systematic review and meta-analysis. J Clin Exp Hepatol 12(3): 818-829.
-
Byrne CD, Targher G (2015) NAFLD: A multisystem disease. J Hepatol 62: S47-S64.
-
Asrani SK, Devarbhavi H, Eaton J, Kamath PS (2019) Burden of liver diseases in the world. J Hepatol 70: 151- 171.
-
Ghosh S, Bera PK, Saha A, Sur TK (2022) Comparative analysis of amoebic liver abscess versus pyogenic liver abscess on clinical and investigative consequences. J Indian Med Association (JIMA) 120(3): 36-40.
-
Jindal A, Pandey A, Sharma MK, Mukund A, Vijayaraghavan R, et al. (2021) Management practices and predictors of outcome of liver abscess in adults: a series of 1630 patients from a liver unit. J Clin Exp Hepatol 11: 312-320.
-
Liu ZL, Xie LZ, Zhu J, Li GQ, Grant SJ, et al. (2013) Herbal medicines for fatty liver diseases. Cochrane Database of Systematic Reviews 24(8): CD009059.
-
Yan T, Yan N, Wang P, Xia Y, Hao H, et al. (2020) Herbal drug discovery for the treatment of nonalcoholic fatty liver disease. Acta Pharmaceutica Sinica B 10(1): 3-18.
-
Kim S, Lee Y, Cho N, Choi H, Kim K (2021) A systematic review of herbal medicine in the treatment of cirrhotic ascites. J Korean Med 42(4): 222-237.
-
Joshi V, Pandit S, Saha A, Khan M, Somani R, et al. (2023) Assessment of quality of life in cancer patients supplemented with Ayurvedic medicine (Body Revival): Case Reports. Adv Phar & Clin Tria 8(2): 000215.
-
Joshi V, Khan M, Somani R, Pandit S, Sur TK (2023) Indian medicine can improve quality of life in breast cancer patients: Case Studies. Nat Ayurvedic Med 7(2): 000395.
-
Sur TK, Auddy B, Bhattacharyya D (2011) Effects of Body Revival (herbal formulation) on human platelet aggregation and myocardial ischemia in rats. Zhong Xi Yi Jie He Xue Bao 9(7): 746-751.
-
Khan M, Pandit S, Saha A, Joshi V, Sur TK (2022) Perspective of using Indian polyherbal medicine in the treatment of cancer. Curr Res Compl Alter Med 6: 165.
-
Bhattacharyya D, Pandit S, Jana U, Sen S, Sur TK (2005) Hepatoprotective activity of Adhatoda vasica aqueous leaf extract on D-galactosamine induced liver damage in rats. Fitoterapia 76(2): 223-225.
-
Sur TK, Hazra A (2015) Hepatoprotective and antioxidant properties of LST-02, a proprietary herbal formulation. Indian J Physiol Pharmacol 59(3): 322-329.
-
Sur TK, Hazra A, Hazra AK, Bhattacharyya D (2016) Antioxidant and hepatoprotective properties of Indian Sunderban mangrove Bruguiera gymnorrhiza L. leave. J Basic Clin Pharm 7(3): 75-79.
-
Rathee D, Kamboj A, Sachdev RK, Sidhu S (2018) Hepatoprotective effect of Aegle marmelos augmented with piperine co-administration in paracetamol model. Revista Brasileira de Farmacognosia 28(1): 65-72.
-
Xia Y, Yan M, Wang P, Hamada K, Yan N, et al. (2022) Withaferin A in the treatment of liver diseases: Progress and pharmacokinetic insights. Drug Met Disposition 50(5): 685-693.
-
Siddique A, Gaur PA, Bajpai A, John A (2022) Evaluation of hepatoprotective potential of Rubia cordifolia in experimentally (carbon tetrachloride) induced hepatotoxicity in albino rats. Int J Health Sci6(S4): 804- 814.
-
Vidya R, Kalaivani K, Amudha P (2022) Therapeutic potential of Cucumis melo (L.) fruit extract and its silver nanopartciles against DEN-induced hepatocellular cancer in rats. Appl Biochem Biotechnol 194(1): 368- 381.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study