Impact of COVID-19 Infection in Kidney Transplant Patients: A Review
Managing COVID-19 in kidney transplant patients is complex due to limited data on its severity, treatment, and management. Conflicting information from studies necessitates case-by-case treatment decisions. Atypical symptoms can lead to misdiagnosis, so a thorough evaluation is crucial. Immunosuppressants and comorbidities can worsen the disease, leading to the controversial approach of discontinuing or reducing immunosuppressive drugs. Kidney transplantation is challenging due to the surgical procedure’s sensitivity and high risk of transmission. While vaccines offer protection, their efficacy may be altered by immunosuppressive drugs in these patients. This review summarizes the management of COVID-19 in kidney transplant patients, addressing these complexities. Kidney transplant patients face unique COVID-19 challenges due to weakened immunity. They are at higher risk for severe illness and complications from both the virus and immunosuppressant medications. Early identification and intervention are crucial, including antiviral treatment like remdesivir in severe cases. Managing immunosuppressants is critical to balancing the risk of transplant rejection with COVID-19 severity. Drug interactions with COVID-19 treatments require careful consideration, potentially necessitating dose adjustments or alternative medications. The pandemic has disrupted transplant services, highlighting the need for prioritized vaccination and safe access to care. Telemedicine can help minimize virus exposure during post-transplant follow-up. While immunosuppression may impact vaccine responses, vaccination remains crucial to reducing the severe COVID-19 risk. Booster doses and continued precautions are important. Mental health support is essential to address pandemic-related anxiety, depression, and social isolation. More data is needed on the safety and effectiveness of COVID-19 treatments and vaccines in this population. A multidisciplinary approach, including close monitoring, careful medication management, vaccination, and psychosocial support is needed to optimize management and improve outcomes.
Introduction
Coronavirus disease has become a curse for the people of the whole world. The life-threatening culprit of this contagious disease is the novel SARS (severe acute respiratory syndrome) Cov-2 virus (coronavirus-2). This pandemic was first reported in Wuhan city of China and rapidly spread throughout the world. The main pathway of COVID-19 transmission is the respiratory route through the inhalation of droplets and airborne particulate carrying infectious viruses. This notorious virus can down-regulate the host immune response by dysregulating the activation of macrophages, disabling the cellular response of natural killer cells. COVID-19 induces a systemic hyperinflammatory response characterized by an increased level of inflammatory cytokines which can cause multiple organ damage in severe cases [1]. So, sudden loss of kidney function can be developed due to acute kidney injury caused by COVID-19 [2]. So, kidney transplant patients with COVID-19 are considered a high- risk group. In end-stage kidney disease (ESKD) patients lose their kidney functions gradually with the development of other complications like heart disease, high blood pressure, anemia, fluid retention, malnutrition, etc. So, kidney transplantation can be beneficial for patients to live longer with improved quality of life. However, transplant patients must take immunosuppressive drugs or anti-rejection drugs of different classes after post-operative period to suppress the immune system to reduce the risk of rejection of transplant kidneys [3]. Since their immune system is suppressed by immunosuppressive drugs, they are highly susceptible to being affected by SARS Cov-2 as these immunosuppressants interfere with the activation and proliferation of T-cell which is a very important part of the immune system to combat with any kind of viral attack in the body [4]. Besides comorbid conditions increase the mortality rate of these patients due to impaired immune systems [5]. Sometimes they manifest atypical symptoms and sometimes diagnosis can give false-negative results [3]. To handle the worsening situation of this vulnerable class of patients, continuous monitoring, management, and treatment protocol are very essential to protect their life. Since the severity of sign symptoms can vary, treatment approaches should be individualized based on the condition. Besides, kidney transplantation facilities should be more improved and organized to properly carry out any kidney transplantation in this pandemic situation [6]. Emphasis should be given to the development of appropriate vaccination criteria for this special class of patients.
Consideration of Chronic Kidney Disease (CKD) Stages
The stages of chronic kidney disease (CKD) is crucial when managing drug interactions involving immunosuppressants and antivirals, particularly because CKD can impact drug metabolism and elimination. Here’s a note specifically addressing this:
It’s imperative to recognize the stage of CKD in patients requiring both antiviral and immunosuppressant therapy. CKD stages, ranging from mild to severe impairment of kidney function, influence drug dosing and pharmacokinetics. Adjustments may be necessary to prevent drug toxicity or suboptimal therapeutic effects. Regular monitoring of kidney function, including estimated glomerular filtration rate (eGFR) and serum creatinine levels, guides appropriate medication management in this population. Collaboration with nephrology specialists may be beneficial for optimizing therapeutic regimens and minimizing the risk of adverse events.
Understanding the stages of chronic kidney disease (CKD) is crucial for managing drug interactions involving immunosuppressants and antivirals, as CKD can impact drug metabolism and elimination. The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) classification categorizes CKD into five stages based on glomerular filtration rate (GFR) and other markers of kidney function. Each stage represents different degrees of kidney impairment, ranging from mild to severe: Stage 1: Kidney damage with normal or increased GFR (>90 mL/min/1.73 m²) Stage 2: Mild reduction in GFR (60-89 mL/min/1.73 m²) Stage 3: Moderate reduction in GFR (30-59 mL/min/1.73 m²) Stage 4: Severe reduction in GFR (15-29 mL/min/1.73 m²) Stage 5: Kidney failure or end-stage renal disease (ESRD) with GFR <15 mL/min/1.73 m² or on dialysis Each stage requires careful consideration when prescribing medications to ensure optimal therapeutic outcomes and minimize the risk of adverse effects.
Age- and Gender-Wise Disease Distribution
Age and gender play significant roles in the distribution of chronic kidney disease (CKD) among populations. Epidemiological studies have shown variations in CKD prevalence and progression based on age and gender.
Age Distribution: CKD prevalence tends to increase with age, with older adults being more susceptible to kidney function decline due to factors such as vascular aging, comorbidities, and medication use. However, CKD can also affect younger individuals, particularly those with underlying health conditions or genetic predispositions.
Gender Distribution: While CKD affects both men and women, certain gender-specific factors may influence disease prevalence and progression. For example, some studies suggest that men may have a higher prevalence of CKD compared to women, possibly due to differences in lifestyle factors, genetic predisposition, and hormonal influences. However, CKD progression and outcomes may vary between genders, warranting individualized management approaches.
Understanding the age- and gender-related patterns of CKD can inform healthcare providers about population- specific risk factors, screening strategies, and treatment interventions tailored to the needs of diverse patient groups. Collaborative efforts involving primary care physicians, nephrologists, and other healthcare professionals are essential for addressing these complexities and optimizing CKD management across different demographics.
Incorporating Psychological Therapy for Patients with Chronic Kidney Disease (CKD)
Patients with chronic kidney disease (CKD) often face significant psychological challenges alongside their medical condition. Integrating psychological therapy into their care can improve overall well-being and treatment outcomes. Here’s how psychological therapy can benefit CKD patients.
Addressing Emotional Distress: CKD diagnosis and its management, including dialysis or transplantation, can evoke feelings of anxiety, depression, and stress. Psychological therapy provides a safe space for patients to express their emotions, learn coping strategies, and develop resilience in dealing with the challenges of living with CKD.
Managing Lifestyle Changes: CKD often necessitates significant lifestyle modifications, such as dietary restrictions, fluid intake management, and medication adherence. Psychological therapy can help patients navigate these changes by providing education, support, and motivation to adhere to treatment recommendations.
Improving Quality of Life: CKD can impact various aspects of a patient’s life, including social relationships, work, and leisure activities. Psychological therapy aims to enhance quality of life by addressing psychosocial factors that may contribute to distress or impaired functioning. This may involve interpersonal therapy, cognitive-behavioral techniques, or mindfulness-based interventions.
Facilitating Adjustment to Illness: CKD is a chronic condition that requires long-term management, which can be emotionally challenging for patients and their families. Psychological therapy assists individuals in adapting to their illness, fostering acceptance, and promoting a sense of control over their health outcomes.
Supporting Caregivers: Caregivers of CKD patients also experience psychological strain due to the demands of caregiving, uncertainty about the future, and concerns for their loved one’s well-being. Psychological therapy offers support and coping strategies for caregivers, recognizing their vital role in the patient’s care.
Promoting Patient Empowerment: Psychological therapy empowers CKD patients to actively participate in their treatment decisions, communicate effectively with healthcare providers, and advocate for their needs. It fosters self-efficacy and resilience, empowering patients to navigate the complexities of managing their condition.
Integrating psychological therapy into the multidisciplinary care of CKD patients enhances holistic care, addressing not only the physical but also the emotional and social aspects of their well-being. Collaborative efforts among nephrologists, mental health professionals, and support networks are essential in providing comprehensive support for CKD patients throughout their healthcare journey [7, 8].
WHO COVID-19 Variants Classification
The World Health Organization (WHO) has established a classification system for COVID-19 variants based on their public health significance. This system categorizes variants into different classes, including Variants of Interest (VOIs) and Variants of Concern (VOCs), to monitor their spread and impact. Here’s an overview.
Variants of Interest (VOIs): Variants that are closely monitored due to specific genetic changes that may affect virus characteristics, such as transmission, severity, or immune evasion. VOIs have the potential to pose a risk to global public health.
Variants of Concern (VOCs): Variants that have demonstrated increased transmissibility, virulence, or decreased effectiveness of public health and social measures, diagnostics, vaccines, or therapeutics. VOCs are prioritized for enhanced monitoring and research to inform public health responses.
The classification of variants by WHO helps guide public health actions, including surveillance, risk assessment, and the development of countermeasures such as vaccines and treatments. It facilitates international collaboration and coordination in the fight against COVID-19 by providing a standardized framework for monitoring and responding to emerging variants. Regular updates on variant classification are issued by the WHO to ensure timely and evidence-based decision-making in pandemic response efforts [9, 10, 11].
Prevalence of COVID-19 in Kidney Transplant Patients
Several studies and reports suggest higher morbidity and mortality among candidates waitlisted for a kidney transplant and recipients of a kidney transplant transplantation. Recently attention has been given to this class of people [12]. COVID-19 infection shows a greater progression among immunocompromised kidney transplant patients with a higher rate of ICU admission and fatality (21.4%) [13]. In the Bronx, New York the prevalence of COVID-19 was found 23.4% among kidney transplant patients tested by either RT-PCR or SARS-Cov-2 IgG with a 20.5% mortality rate. The mortality rate was very high in hospitalized patients (37.8%). Another study in six transplant centers of London found 121 transplant recipients with COVID-19 positive among whom 36 patients died after hospitalization. In this case, the mortality rate was about 30% and higher mortality was found in older kidney transplant patients [14]. In Italy, a retrospective study was conducted on 82 adult kidney transplant patients with COVID-19 during the first and second outbreaks. The incidence of infection in transplant centers was 5.2%. Here, 37 hospitalized older patients showed the severity of respiratory symptoms and a lengthy disease period. Even the mortality rate (29.7%) was about four times higher than that of the general population [15]. In a cohort study in the USA, COVID-19 was blamed for 11% of waitlisted patients’ deaths in 2020, and these patients were more likely to be male, obese, and from a racial/ethnic minority group. COVID-19 was responsible with about one out of every six deaths (16%) among active transplant recipients in the United States in 2020. COVID-19 recipients were younger, more likely to be obese, have lower educational attainment, and be members of racial/ ethnic minority groups than COVID-19 recipients who died of other causes in 2020 or 2019. According to a cohort study in the institute for Urology and Renal Transplantation in Cluj-Napoca, overall mortality during the first wave was 24%, whereas during the second wave it was 16%. During both COVID-19 waves, hospitalized patients died at the same rate (27%). Intensive-care patients died in 8 out of 9 cases (89%) in the first wave, but only 68 % of ICU patients died in the second wave (23 deaths). In the United States, case analysis of a group of kidney transplant patients with COVID-19 has noticed a higher rate of early mortality rate (28% at 3 weeks) than mortality with COVID-19 in the general population (only 1%-5%). Even the mortality rate with in COVID-19 patients with age greater than 70 years old is lower (8-15%) than COVID-19 in kidney transplant patients [16].
Diagnosis of COVID-19 in Kidney Transplant Patients
Like the general population, COVID-19 is detected by real-time RT-PCR (reverse transcriptase polymerase chain reaction) tests in kidney transplant patients. However, due to some accuracy problems, the findings of this test results cannot be reliable to large extent [17]. So, some other pathological tests are needed to be performed for firm confirmation of COVID-19 in kidney transplant patients. So, while dealing with transplant patients with nonspecific symptoms without any microbiological isolation and epidemiological risk factors, the entire medical team should be alert and consider the diagnosis of COVID-19 [18].
Real-time RT-PCR Test: According to WHO, to detect the presence of COVID-19 in any symptomatic patients, a real-time RT-PCR test with the oropharyngeal and nasopharyngeal swabs of suspects is used [19]. However, asymptomatic recipients or tests before 5-7 days of onset of symptoms have a higher tendency to give false negative results through the RT-PCR test.3 Moreover, due to the use of long-term immunosuppressants, these patients have a poor prognosis of the disease [17]. So, underdiagnoses can occur due to limited sensitivity. Within this time of false detection, symptoms become more complicated which can lead to a greater chance of mortality in patients. So, it has been recommended to do a second RT-PCR test in symptomatic kidney transplant patients, if their first test result comes out negative [19]. Apart from these, to overcome this limitation some other pathological tests should be conducted to check the severity of infection and inflammation. Symptoms, intensity of community transmission of COVID-19 and contact tracing can give a signal about the invasion of COVID-19 in kidney transplant patients. These factors can be the basis of diagnosis.
T lymphocyte counts: Patients have reduced lymphocyte count as they take immunosuppressive drugs and in the case of COVID-19, this level decreases drastically which is a positive sign of COVID-19 infection [17]. Hospitalized patients experience lymphopenia and thrombocytopenia (Montefiore, 2020). However, immunosuppressants can cause drug-induced lymphopenia for which the report of low T-cell levels cannot be the only reliable diagnosis [20]. But most of the studies showed a radical change in T-cell count among kidney transplant patients with COVID-19.
C-reactive Protein: C-reactive protein (CRP) is an indicator of systemic inflammation and is associated with infection and positively correlated with lung lesions. In COVID-19 the level of CRP goes beyond the normal range and patients with high C-reactive protein have displayed adverse outcomes [21]. Due to overwhelming inflammation, the level of CRP increase in most kidney transplant patients with COVID-19 [17]. As the elevation of CRP can be variable based on the severity of the infection, detection of CRP level can predict patients’ condition.
Serum creatinine and blood urea nitrogen: These two are biological markers of kidney function. As kidney transplant patients have compromised kidney function and COVID-19 can cause kidney failure, these markers should be monitored periodically to evaluate the kidney status of infected patients [17]. COVID-19 infection can increase the level of these two biochemical substances in most kidney transplant patients.
D-dimer: The level of D-dimer protein is an indicator of blood clots which is noticed in COVID-19 patients. The D-dimer level is a biomarker for predicting the mortality rate and severity of patients with COVID-19. It has good accuracy and sensitivity. Patients with a high level of complexity show elevated levels of D-dimer [22].
Ferritin: It has been hypothesized the Ferritin level can influence the complications related to COVID-19 as it can play a key role in dysregulating immunity by providing an immunosuppressive effect and inducing cytokine storm [23]. Several studies have given evidence of high ferritin levels in severe cases especially patients with comorbidities like diabetes mellitus. In the case of kidney transplant patients, hospitalized individuals have shown high ferritin levels during COVID-19 infection [16].
White blood cell, neutrophil and Procalcitonin: These three factors have been found in the normal range in one study where the kidney transplant patient experienced mild respiratory discomfort and showed comparatively stable condition [17]. However, in another study, hospitalized kidney transplant patients with critical COVID-19 symptoms have shown a higher percentage of these three markers [24]. So, there is a link between the severity and level of these inflammatory markers. In atypical symptoms of COVID-19, the WBC count was reported normal in range [18].
Troponin Level: A High troponin level has been noticed during COVID-19 in kidney transplant patients, especially those who are hospitalized and have comorbidities like heart disease [25].
Chest Computed Tomography (Chest CT): Chest CT reports can identify pneumonia 26. This also helps to predict lung involvement. A CT report of two kidney transplant patients with COVID-19 showed 40%-50% of lung involvement during hospitalization which was a typical representation of pneumonia. This report helps to be confirm viral pneumonia and the initiation of a specific treatment approach. Even CT report has acted as a basis for performing RT-PCR test to detect COVID-19 in these patients since RT-PCR was carried out based on the CT report [27].
Antibody detection: A cohort of 36 kidney transplant patients with COVID-19 showed the development of detectable IgG antibodies after approximately 15 days of infection. So, detection of antibodies in a patient’s serum can identify any past COVID-19 infection retrospectively. But in this case, the timing of tests is very important. In a study,42% of kidney transplant patients were detected SARS CoV-2 positive with any noticeable symptoms. However, SARS- CoV-2 IgG detection is a less sensitive technique for elderly patients and patients with a high serum creatinine level [28].
History searching: Besides all of these above-mentioned tests, history taking of suspected patients about their physical contact with any COVID-19-affected patient or traveling history in any area with a high prevalence of COVID-19(contact tracing) can give preliminary hints about infection by COVID-19 [29].
Others: As false-negative results can be found in nucleic acid tests due to improper sampling, viral accumulation in the upper respiratory tract, and mutation in the virus gene, some other kinds of detection techniques can be included as a diagnostic approach for optimized diagnosis of COVID-19 in kidney transplant patients. These can be lower respiratory tract sampling, whole genome sequencing etc [30].
Signs and Symptoms of COVID-19 in Kidney Transplant Patients
The clinical presentation of COVID-19 in kidney transplant patients is quite similar to the immunocompetent patient. However, these symptoms can vary from patient to patient. Even patients can be asymptomatic and can show atypical symptoms. Besides, the severity of symptoms can vary to a higher extent in kidney transplant patients. Typical presentation of symptoms Fever: According to study findings, at the initial stage of infection by COVID-19, kidney transplant patients show fever less commonly (58%). Even some data have told that patients can be asymptomatic at an earlier phase of infection. On the other hand, manifestations of fever have been considered as very common initial typical symptoms in certain case reports and case series. In a case series of each of 5 kidney transplant patients showed fever, a common symptom of COVID-19 [30]. In milder cases, body temperature remains < 38 °C and in moderate to severe cases > 38°C has been observed [20]. So, in general, fever can be considered a very common symptom in kidney transplant patients just like general populations.
Dry cough and sputum: Dry cough is very common in maximum people [17]. A case report of 59 years old kidney transplant patient was admitted to the hospital with fever and cough [31]. A case series showed sputum production in 60% of cases (3 out of 5 patients) [30].
Renal impairment and concomitant infection: Impairment of kidney functionality is noticed in all kidney transplant patients infected with COVID-19 in varying ranges as this novel virus can affect the renal system of hosts and alter its regular activity. In kidney transplant patients the possibility of renal dysfunction is high. Nosocomial bacterial and fungal superinfection infection has been found in several cases [13].
Lymphopenia: 2 case series of transplant patients in New York have shown lymphopenia as a profound symptom than non-transplant patients of COVID-19. In another case series in China, 5 kidney transplant patients with COVID-19 also display lymphopenia as a very common symptom. Lymphopenia is noticed in about 63% of general populations infected with COVID-19. On the other hand, according to some investigators, in most kidney transplant patients drug-induced lymphopenia occurs [20]. So, lymphopenia as a symptom of COVID-19 in kidney transplant patients is conflicting. But in COVID-19 their lymphocyte level drastically falls which can be the impact of both COVID-19 infection and the use of immunosuppressive agents.
Leukopenia and High LDL level: Leukopenia (low count of leukocyte or WBC in the blood) and high Low-density lipoprotein (LDL) levels have also been noticed in COVID-19 of kidney transplant patients [13].
Pneumonia: COVID-19 related pneumonia is seen in most cases of hospitalized kidney transplant patients. In a case study, about 96% of hospitalized kidney transplantation recipients with COVID-19 show viral pneumonia [16]. Bilateral COVID pneumonia was more frequent during the first wave.
Symptoms even after vaccination: Unfortunately, even after vaccination, kidney transplant patients can be diagnosed with COVID-19 and they show cough, fever, dyspnea, fatigue, diarrhea, and body pain. Despite completing the course of vaccination, the severity of illness may not be minimized retrospective cohort study with 10 kidney transplant patients displayed severity among these patients. 7 Patients were hospitalized with severe symptoms of COVID-19. Their oxygen saturation was <94 and treated with mechanical ventilation and supplemental oxygen- therapy. So, transplant patients should remember that they are not fully safe from COVID-19 after becoming vaccinated.
Atypical presentation of symptoms: Vomiting and myalgia as initial symptoms: A case report of 50 years old kidney transplant patient (in 2016) has manifested vomiting, myalgia, and fever with gastrointestinal symptoms which are infrequent in general populations and progressive cough was developed without dyspnea and conjunctivitis. So this case has indicated the atypical clinical symptoms of COVID-19 in kidney transplant patients [31].
Initial symptoms without a fever: In Italy, 36-year-old female with kidney transplantation and COVID-19 positive showed only milder cough, fatigue, and coryza and had no fever. Even her lymphocyte count and interleukin level were within a normal range [29].
Pneumonia without foreseeable respiratory symptom: Sometimes patients do not display any considerable respiratory symptoms, although their radiological test reports show evidence of pneumonia.23 Initial gastrointestinal representation without any respiratory symptom: In Spain, a case report of 50- year- old male patient, recipient of 3rd deceased donor kidney transplant, showed rare symptoms after affecting COVID-19 which delayed the diagnosis of the actual disease. He had no previous traveling history to the area of high prevalence with COVID-19. Initially, he showed fever (38.2°C), vomiting, and mild dehydration without any respiratory symptoms, and C-reactive protein, WBC count was normal. Mild kidney impairment was found by testing serum creatinine and GFR level. The physician suspected it was non-severe gastroenteritis and gave only acetaminophen as medication for fever. But after 5 days he developed a progressive dry cough with persistent fever and showed no gastrointestinal symptoms. Conjunctivitis, mucous dehydration crackle in the lung, and dyspnea appeared without other severe abnormalities. Based on the chest report of the lung, community-acquired pneumonia was suspected but swab tests for influenza A and B and respiratory syncytial virus came out negative. Despite the absence of any travel history to the area of contagious infection, the COVID-19 test was performed according to local screening protocol. Finally, the real-time RT-PCR test was come out positive.
This initial gastrointestinal symptom of COVID-19 is very rare (3-5%) and atypical. Electrolyte disorder (hyponatremia) and conjunctivitis are also considered as infrequently seen symptoms. These types of atypical symptoms under high immunosuppressive dose and without any epidemiological risk factor make the differential diagnosis of COVID-19 more difficult [18].
Factors that can influence the severity of illness in kidney transplant patients infected with COVID-19
The information about the impact of COVID-19 in kidney transplant patients compared with the non-transplant population is very limited [5]. But some factors have an inductive effect to make the COVID-19 disease more severe in kidney transplant patients. These are:
Dysfunctional immunity
Deregulated and hyper inflammatory immune response is mainly responsible for disease severity. Extreme low levels of T-cell after COVID-19 in kidney transplant patients can cause patient death even under mechanical ventilation which has been found in a 59-year-old kidney transplant patient. Even after finding negative results in the RT-PCR test, this patient died, although all types of necessary treatment approaches were taken [26]. Most of the hospitalized patients due to COVID-19 have lymphopenia [25]. Previous immunologic weakness due to immunosuppression and infection by COVID-19 can increase the vulnerability of patients [26].
Comorbidities
It can also be said that renal transplant patients with other comorbidities (diabetes mellitus, chronic kidney disease, heart disease, hypertension, etc.) are highly susceptible to being infected by SARS-CoV-2 [4]. So, they show the severity of symptoms. On the other hand, comorbidities in transplant patients make difficulties in the assessment of the influence of transplantation on the severity of COVID-19 disease. Malignancy and coinfection can also be contributing factors to the severity of COVID-19 in kidney transplant patients [30]. Microscopical analysis of transplant kidneys showed the presence of viral inclusion in the kidney cell and histological analysis of endothelium of the heart and lung showed accumulation of inflammatory cells. So, comorbidities and endothelium dysfunction have contributed to the severity of this kidney transplant patient [32].
Immunosuppressant
Immunosuppressants for kidney transplant patients comprise a combination of calcineurin inhibitors, azathioprine, mycophenolic acid/MMF (MPA/MMF), mammalian target of rapamycin‑inhibitors, prednisone, and belatacept. Therapeutic class, type, dose, side effects, and intensity of immunosuppressive agents can influence the disease severity of COVID-19 in kidney transplant patients. For example:
- Anti-lymphocyte antibodies and anti-metabolite can cause lymphopenia which is a very common contributor to the severity of COVID-19 in kidney transplant patients.
- A part of these, Cyclosporine A and Mycophenolate mofetil can induce opportunistic and viral infection as well [26].
- In the case of mammalian target of rapamycin (mTOR)- inhibitors there is a controversy. Some research declared that it impairs the adaptive immunity in kidney transplant patients which increases the disease severity. On the other hand, some consider that this immunosuppressant is biologically active against coronavirus. Lymphocyte- depleting antibodies also increase the risk of COVID-19 in kidney transplant patients [25].
- Combination of hydroxychloroquine and ritonavir plus lopinavir causes QTc interval prolongation [5].
- In a follow-up study,4 out of 7 patients who were hospitalized have shown lymphopenia, which can display a link between COVID-19 severity and low lymphocytes count [25].
But a case series in China showed that five kidney transplant patients with milder symptoms of COVID-19 recovered gradually without any mechanical ventilation support and ICU admission and they were on the maintenance dose of various immunosuppressants. This indicates that milder symptoms of COVID-19 in kidney transplant patients do not decline more due to the maintenance dose of immunosuppressive drugs [30]. But more valid evidence is needed for its approval. case of 58-year-old male kidney transplant patient who died in COVID-19 due to a drastic fall of T-cell which might have occurred due to the use of Mycophenolate mofetil. At the same time, this drug might worsen the pneumonic condition [26].
Drug-Drug Interaction Between Anti-Viral and Immunosuppressant
In COVID-19 of kidney transplant patients along with reduced immunosuppressive doses other anti-viral and antibiotic therapy are given. These drugs can interact with each other and alter their desired effectiveness and efficacy (Figure 1). So, it is another concerning issue in this case that can worsen the situation of patients and make the treatment procedure more complicated [29].
Lopinavir and ritonavir interact with a calcineurin inhibitor, Tacrolimus, and have a risk of induced mTOR- inhibitor-induced pneumonitis [8]. It has been found that lopinavir and ritonavir are inefficient treating hospitalized kidney transplant patients in terms of viral clearance and these two anti-viral also interact with calcineurin inhibitors interfering with its metabolism [5]. As the pharmacokinetics of Tacrolimus is dependent on CYP3A4, any kind of inhibition of this enzyme can alter the Tacrolimus level in the blood. This kind of competitive inhibition of the CYP3A4 enzyme by lopinavir and ritonavir increases the bioavailability of Tacrolimus and other calcineurin inhibitors.23 A combination of two protease inhibitors can increase the blood Tacrolimus to the toxic level compared with a single protease inhibitor [20].
Interaction between ritonavir and Tacrolimus can influence the glomerular filtration rate in kidney transplant patients [29]. Based on these phenomena, a reduced dosage of protease inhibitor should be used [20]. Recently it has been found that Darunavir/Ritonavir and Darunavir/Cobicistat can be used as an alternative for the anti-viral medication [33].
Sirolimus cannot be given with lopinavir as it shows high and injurious interaction. But Cyclosporin has shown significant interaction with lopinavir which requires dosage adjustment [20]. Interaction between hydroxychloroquine and ritonavir/lopinavir can also prolong the cardiac QTc interval, although this is not seen in all patients [29]. Azathioprine shows potential interaction with hydroxychloroquine and MMF shows interaction with lopinavir. Anti-thymocyte globulin, Belatacept and Basiliximab do not show any significant interaction with any kind of anti-viral drugs [20].
![Figure 1: Drug-drug interactions between antivirals and immunosuppressants [20].](/fulltextimages/12845/fig_1.png)
Management and treatment of drug-drug interactions between antiviral medications and immunosuppressants require careful consideration to minimize risks and maintain therapeutic effectiveness. Here’s a concise overview:
Identify Potential Interactions: Healthcare professionals should be vigilant in recognizing potential interactions between antivirals and immunosuppressants. This involves thorough medication reconciliation and awareness of the pharmacokinetic and pharmacodynamic properties of each drug.
Assess Patient’s Medical History and Condition: Consideration of the patient’s medical history, including comorbidities and organ function, is essential. Additionally, assess the severity of the underlying condition requiring treatment with both antiviral and immunosuppressant medications. Consultation with Healthcare Providers: Collaboration among healthcare providers, including infectious disease specialists, pharmacists, and transplant specialists, is crucial in managing these interactions. A multidisciplinary approach ensures comprehensive evaluation and tailored management strategies.
Adjust Dosing and Monitoring: Depending on the specific drugs involved and the clinical scenario, dosage adjustments may be necessary to minimize adverse effects or therapeutic failure. Close monitoring of drug levels, therapeutic response, and adverse reactions is essential to optimize outcomes.
Pharmacological Interventions: In some cases, pharmacological interventions such as changing the timing of medication administration, selecting alternative drugs with lower interaction potential, or using pharmacokinetic enhancers or inhibitors may be considered. Non-Pharmacological interventions: Non- pharmacological interventions play a vital role in managing drug interactions. This includes patient education regarding medication adherence, potential side effects, and the importance of regular follow-up appointments. Lifestyle modifications and dietary considerations may also be relevant.
Regular Follow-up and Communication: Patients should undergo regular follow-up visits to assess treatment response, monitor for adverse effects, and adjust therapy as needed. Open communication between patients and healthcare providers facilitates early detection and resolution of any emerging issues.
By employing a comprehensive approach that integrates pharmacological and non-pharmacological interventions, healthcare professionals can effectively manage drug-drug interactions between antiviral and immunosuppressant medications while optimizing patient outcomes and safety [34, 35, 36].
Acute kidney rejection
There are many cases of graft loss and de novo chronic antibody-mediated allograft rejection following COVID-19 among kidney transplant patients [37, 38, 39]. Due to sudden reduction or discontinuation of immunosuppressive drugs as a treatment approach to COVID-19 in kidney transplant patients can induce acute rejection which can complicate the severity and future treatment plan and recovery procedure [30].
Acute kidney injury
Kidney transplant patients are highly susceptible to being affected by acute kidney injury (AKI) and COVID-19 can increase this possibility. A large cohort study has found a higher rate of AKI and mortality in kidney transplant patients affected with COVID-19 than in the general population kidney rejection 1. The presence of the ACE-2 receptor, the main way of viral entry, at proximal tubular epithelium can be a probable cause of AKI.20 AKI in KTRs with verified COVID-19 was studied in 38 individuals, 30 of whom were AA (79 %). AKI was found in 71.1 % (n=27) of COVID-19 KTRs. That group had a 71 percent (27/38) incidence of AKI. The rate of AKI among African Americans (AA) was 76.7 %, compared to 50 % in the non-AA group. Although AA race was not an independent predictor of AKI in our population, we believe the elevated incidence of AKI in AA is due to the higher prevalence of diabetes. Among these 7 kidney transplant patients, 4 developed AKI which also reveals that kidney transplant patients with COVID-19 have the possibilities to develop AKI [25].
Time of transplantation
Kidney transplantation during this pandemic condition may enhance the progression of pneumonia as post-transplantation therapy weakens the immunity of transplant patients [26]. According to the UK organ donation and transplantation association, within the first 3 months of transplantation, there is a high risk of severity of COVID-19 in kidney transplant patients due to high doses of immunosuppressive drugs to prevent kidney rejection. Besides, the virus can be transmitted from one donor to the recipient [25].
Atypical symptoms
Peculiar symptomatic representation of COVID-19 disease in this type of patient can mislead the treatment approach. This type of exceptional case can misguide the dosage adjustment of immunosuppressive drugs during the management of COVID-19 in kidney transplant patients [29]. Banerjee et al. found that the kidney transplant patient who died after the COVID-19 infection showed no severe respiratory complications but rather manifested bowel infarction and intra-abdominal sepsis. So, sometimes extra-pulmonary complications can be responsible for high mortality due to COVID-19 in kidney transplant patients [25]. An Italian woman of 36 years old with 2nd-time kidney transplantation was diagnosed COVID-19 positive by RT- PCR test but her initial symptoms were very mild (slight dry cough, fatigue, coryza without any fever) despite using immunosuppressants and her symptoms took time to develop and did not deteriorate rapidly. So, the physician did not stop the Tacrolimus which led to a high trough level of Tacrolimus in those patients [29].
Probability of Spreading COVID-19 Infection by Kidney Transplant Patients
Kidney transplant patients are immunocompromised and this lowers the infectious dose to cause COVID-19. Furthermore, kidney transplant recipients have a higher ability to shed a greater amount of virus for a long period than the general population [31]. So, researchers have given a hypothesis that this type of patient has a higher tendency to spread the most infectious coronavirus than the healthy hosts. So, these types of patients have a probability to transmit COVID-19 into the health care team [31]. But more evidence and analysis are needed to establish this hypothesis. Atypical signs and symptoms, delayed symptoms development and longer incubation period can cause persistent viral shedding without decaying patient’s condition [29]. So, these can also be a probable cause of viral transmission by kidney transplant patients. During kidney transplantation, the virus can be transferred from infected donor to recipient, although adequate valid evidence has not been gathered yet. The virus has been isolated from blood in 15% of cases which poses a risk of virus transmission in all kinds of organ transplantation [40].
Possible Treatment Strategies for COVID-19 Positive Kidney Transplant Patients
Pharmacological approach for COVID-19 in kidney transplant patients
There is no optimal treatment approach for COVID-19 in kidney transplant patients. However, tocilizumab, remdesivir, low‑dose methylprednisolone, convalescent plasma therapy, colchicine, and favipiravir are being utilized for the treatment of COVID‑19 in kidney transplant patients [29]. Different countries have dealt with this complication in different ways. The treatment procedures and medication are individualized according to the clinical presentation and severity of the patient’s condition, time of post- transplant, risk of allograft rejection, types of immunosuppressive drugs etc [5]. Comorbidities can complicate the treatment procedures and in these cases success rate of full recovery is low and the death rate is comparatively high [26]. Besides drug interactions between anti-viral and immunosuppressants have made difficulties in exact dosage determination [20]. To gather information about effective pharmacological therapy for COVID-19 in kidney transplant patients, an explanation of different treatment protocols in several case reports will be more practical [5].
Reduction or discontinuation of immunosuppressive drugs
As immunosuppressants can impair the immune response, recently in most cases it has been suggested that reduction or discontinuation of immunosuppressive agents and steroid treatment can help for faster recovery of kidney transplant patients with COVID-19 positive [25]. It is mainly important for moderate to severe cases including hospitalized patients especially. The main purpose of stopping immunosuppression is to promote specific anti- viral immune responses [27]. But the interesting thing is that some case reports have given evidence of successful recovery of COVID-19 in kidney transplant patients without any termination of immunosuppressants [31].
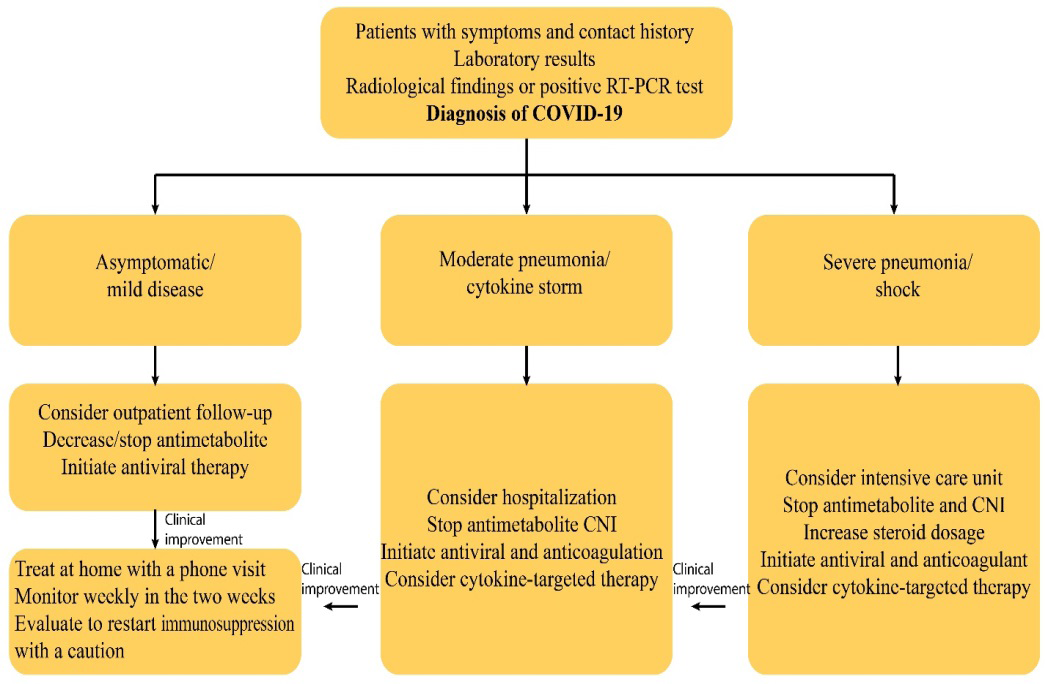
RT-PCR- Reverse transcription-polymerase chain reaction, CNI- Calcineurin inhibitor Figure 2: Treatment scheme for kidney transplant recipients with COVID-19.
Treatment of co-infections
As the immunity of this class of patients is comparatively weaker than a normal healthy person, they are very susceptible to different bacterial and fungal infections [8]. Considering this, the treatment strategy also includes various broad-spectrum antibiotics and anti-fungal drugs to fight against these kinds of infections. Treatment of pneumonia In the case of COVID-19, pneumonia is one of the main dangers that can accelerate the death rate. The main target of the treatment procedure is to fight against this pneumonia that occurs due to opportunistic bacteria during COVID-19 infection and combat dysregulated inflammatory response.
A case study of 50-year-old man with end-stage renal disease of a 3rd deceased donor kidney transplantation was detected covid positive by rRT-PCR test. Hydroxychloroquine inhibits viral replication15891.On the other hand, Remdesivir inhibits the action of a viral enzyme which is called RNA- dependent RNA polymerase enzyme, and incorporated themselves into the newly formed viral RNA reducing the viral load and improving lung function. Although no positive microbial culture has been detected, a broad-spectrum antibiotic (ceftaroline and meropenem) was given as an extra precautionary measure to protect against any bacterial infection. For more severe pneumonia, statin, anti-IL6, or corticosteroid therapy is reserved [8].
Use of corticosteroid with Anti-viral drug
In another case report of Tongji Hospital at Wuhan in China, 49-year-old kidney transplant patient was affected by COVID-19 in February 2020. His transplant specialist suggested stopping Mycophenolate mofetil and halving the dose of Tacrolimus. At the same time an anti-viral drug, Umifenivir (200mg, three times per day) was given orally. But his situation deteriorated with COVID-19 pneumonia. So, Tacrolimus and Prednisolone were discontinued and IV Methylprednisolone, Ribavirin, oral Moxifloxacin, and IV immunoglobulin were administered.
After this new medication approach, the body temperature of the patient decreased but after some days his oxygen saturation level decreased and he was admitted to the respiratory intensive care unit due to breathing difficulty. At this time, methylprednisolone was given intravenously and shifted to oral dose after improving his condition. Then his condition gradually improved and his symptoms disappeared.
Here the emphasis has been given to corticosteroid therapy. Corticosteroid mainly works at the second phase of the disease of COVID-19 in kidney transplant patients which is hyperinflammatory syndrome and cytokine release syndrome. However, glucocorticoids’ use should be based on a case-by-case basis as it can induce prolonged viral shedding in some cases. In some cases, Dexamethasone in combination with Tocilizumab can be given [5]. Besides, Ribavirin which is a member of nucleoside anti-metabolite drug has anti- viral activity against RNA viruses by increasing mutation frequency in their genome and hamper the duplication procedure of viral genetic material.
Fighting cytokine storm to control the severity
The virology department of Strasbourg University Hospital in France has recommended another antibody Belatacept to treat COVID-19 in kidney transplant recipients. A 58-year-old male patient with testicular cancer, renal vein thrombosis, and coronary artery disease had his kidney transplantation in January 2017. After surgery he was taking Belatacept (345mg every 28 days), Mycophenolate mofetil (750mg twice daily), and Prednisolone (5mg per day). 3 weeks after of the last dose of Belatacept, the patient experience fever, and he was identified as a COVID-19-positive patient and hospitalized. But he displayed mild symptoms and his condition did not deteriorate. He recovered very soon only after treatment with bacterial super-infection and low-dose Cyclosporine.
In this patient, it was thought that his situation would worsen due to immunosuppression and comorbidities. Fortunately, he got well soon and this case was hypothesized by the specialist that, Belatacept has played the main role in fighting the massive cytokine storm and chemokine production which is very common in COVID-19. Belatacept, a CTLA-Ig molecule can stop the co-stimulatory B7-CD28 signal which is important for T-cell activation and T-cell and B-cell crosstalk [41]. According to this case study, the immunosuppressant had a positive effect on improving the symptoms of COVID-19 in kidney transplant patients and symptoms were mild [42].
Another case study in Italy has demonstrated that, in addition to cyclosporine (half dose) and Hydroxychloroquine, another humanized monoclonal antibody tocilizumab has been given to a kidney transplant patient with COVID-19. And it has shown a successful recovery with less severity of symptoms [43]. In this case, Tocilizumab has acted as a competitive IL-6 inhibitor which is responsible for the proliferation of T-cell and B-cell differentiation. It had a beneficial effect on COVID-19 pneumonia [43]. In a Group of kidney transplant patients, 6 out of 28 patients have been treated with another monoclonal antibody called Leronlimab.11 It is a Chemokine receptor type-5(CCR5) antagonist that prevents the cytokine storm and in COVID-19 patients, it helps to recruit inflammatory cells-like CD8-T lymphocyte and macrophages, normalize CD4/CD8 ratio and decrease the production of interleukin-6 and thus restore the immune function of critically ill patients. But before using this, importance should be given to the estimation of CRP (C-reactive protein) level. Leronlimab will be applicable only for those patients whose CRP level is elevated [44].
As we know, cytokine storm is a common phenomenon in COVID-19 patients and is responsible for severity and morbidity, discontinuation of anti-rejection therapy in kidney transplant patients can worsen the viral infection. In these patients, a high level of IL-6 has been noticed which can be increased by lowering the immunosuppressant dose [45]. For this reason, Another IL-6 targeting treatment approach has been suggested. An agent has been proposed in this case: that is colchicine. The function of Colchicine is to prevent the NLRP3 inflammasome assembly which is activated by a viral component of SARS Cov-2 known as Viroporin E. In this way, colchicine helps to reduce the level of certain pro-inflammatory cytokines including IL-1b and IL-6 [27]. So, combining two approaches of interrupting immunosuppression and the use of anti-inflammatory agents can give a synergistic effect with anti-viral therapy [27]. In some therapeutic adjustments, calcineurin inhibitor is not discontinued as it can block the function of inflammatory cytokines IL-6 and IL-1. However this agent has the potential to prolong the QTc interval.
Use of Cyclosporin in Place of Anti-Metabolite
A 45-year-old male kidney transplant recipient who had been transplanting 16 years ago was affected by COVID-19. He was on the maintenance dose of MMF an anti-metabolite immunosuppressant. After his COVID-19 infection, he was suggested to switch to a low dose of cyclosporin A which is a calcineurin inhibitor, hydroxychloroquine, and azithromycin. MMF was withdrawn. After 4 days of mechanical ventilation, his condition improved and discharged from the hospital after 17 days. So, cyclosporin-based treatment of kidney transplant patients during COVID-19 can be another therapeutic alternative [46].
Continuation of Conventional Dose of Immunosuppressive Drugs
An exceptional recovery case from COVID-19 of kidney transplant patients has been found in China at an early stage of the pandemic. In China, a case of COVID-19 in a kidney transplant patient was treated successfully without stopping or reducing the dose of the immunosuppressive drug. The 49-year-old male was maintained with three immunosuppressive agents (cyclosporine, mycophenolate mofetil, and prednisolone) after his kidney transplantation. He was also suffering from hypertension and type-2 diabetes. In January 2020, he was admitted to the hospital after getting affected by COVID-19. Ritonavir, lopinavir, Ribavirin, methylprednisolone, and inhalation of interferon alpha- 2b were used to treat the COVID-19 symptoms. Besides, his immunosuppressive drugs were continued according to conventional dose throughout his treatment period. His lung function was quite stable with a slight dry cough. The test result came out negative after 14 days of his illness and he fully recovered. So, although having comorbidities and severe symptoms, a patient could successfully fight this virus. The poorer prognosis of COVID-19 has been described by the Specialist for two possible reasons [47].
One reason can be the protective effect of immunosuppressive drugs which has given protection from hyper-inflammation and excessive cytokine release which can cause organ dysfunction and death. Another cause can be the antiviral activity of Cyclosporine A which can interfere with the replication of various derivatives of coronavirus. So, this is an exceptional case where a normal dose of immunosuppressive drugs acts as a protective agent against the severity of coronavirus [47].
Another cohort study in France also maintained the regular dose of immunosuppressive drugs in kidney transplant patients with COVID-19 infection. However they apply this only for those outpatients and hospitalized patients whose respiratory condition and oxygen saturation were quite stable [19]. But for severe cases, they also discourage the use of anti-metabolite and provide invasive mechanical ventilation.
Treatment of Kidney Transplant Patients with COVID-19 based on their Lung Infiltration
A study at Hospital Lapaz in Madrid has described a treatment protocol for kidney transplant patients with COVID-19 based on the condition of their lung function. This treatment procedure can be described by the following Table 1:
| Kidney transplant patients | Hypoxemia | <60 years | >60 years |
|---|---|---|---|
| Without lung infiltrates | -Maintaining the actual immunosuppressive treatment | Discontinuing MMF and using tacrolimus with the usual dose of Prednisolone (not more than 20mg) | |
| -Tacrolimus dose should be reduced by 20% if used with hydroxychloroquine to prevent significant interaction. Monitoring tacrolimus level every 48 hours and maintaining the level at 4-6ng/ml | |||
| With pulmonary infiltrates | Absent and no fever | Suspending MMF and maintaining with tacrolimus (level 4-6ng/ml) and prednisolone 20mg daily | Stopping MMF with reduction of tacrolimus dose to maintain the level of 3-5 ng/ml and using prednisolone not more than 20mg. |
| Presents with fever and need oxygen. | 1. For 1st four days treat with only 20mg of Prednisolone daily and discarding both tacrolimus and MMF or iMTOR. | 1. For 1st four days treat with only 20mg of Prednisolone daily and discarding both tacrolimus and MMF or iMTOR. | |
| 2. On the 5th day of admission, after confirmation of clinical improvement (no fever and no need for oxygen) tacrolimus, can be resumed to maintain the level of 4-6ng/ml along with prednisolone of 20mg. | 2. On the 5th day of admission, after confirmation of clinical improvement (no fever and no need for oxygen) tacrolimus, can be resumed to maintain the level of 3-5 ng/ml in combination with prednisolone of 20mg. | ||
| 3. If the clinical condition is not improved, only prednisolone of 20 mg/day should be maintained. Tacrolimus will be started again as in point 2 when the patient improves. Here, MMF= Mycophenolate mofetil; iMTOR is the mechanistic target of rapamycin inhibitor. | 3. If the clinical condition is not improved, only prednisolone of 20 mg/day should be maintained. Tacrolimus will be started again as in point 2 when the patient improves. | ||
| 4. In the case of starting hydroxychloroquine, the tacrolimus dose should be reduced by 20%. |
Table 1: Treatment of kidney transplant patients with COVID-19 based on their lung infiltration [20].
Above mentioned drugs have both merits and demerits and not every class of drug and its dosing is appropriate for all kidney transplant patients. Moreover, during the treatment of COVID-19 infection extra awareness and attention should be given to dosage adjustment of these immunosuppressive agents as inappropriate dosing and potential drug interaction can be fatal. So, further research and analysis should be carried out on these drugs to optimize the therapeutic approach for kidney transplant patients with COVID-19 [5].
Convalescent plasma therapy: 3 kidney transplant recipients in the USA got successfully recovered from COVID-19 after receiving convalescent plasma (CP) therapy. So, this can be a potentially useful treatment option, although further research, analysis and trials should be conducted to evaluate the outcome of this treatment option as this was a very small case series that cannot clearly define the exact efficacy of CP. CP products with an optimum level of neutralizing antibody can be more effective if given earlier during the disease period. Other proteins present in CP products are transferred from donor to recipient which strengthens the immune system of the recipient.
Comparison of patient management during two waves of COVID-19: In many ways, patient management varied between the two waves, reflecting evolving health policies and recommendations, growing knowledge about COVID-19, and growing experience. During the second wave, a significant number of patients were treated as outpatients (15 %vs. 39 %). During the second wave, antiretrovirals and hydroxychloroquine were all but disregarded. During the second wave, there was also a trend toward using anticoagulants less frequently. During the second COVID wave, immunosuppression was handled differently. During the second wave, antimetabolites were reduced in a similar proportion (91 vs. 86), but calcineurin inhibitors were reduced or withdrawn more sparingly. Around 40% of transplanted patients who developed COVID-19 required oxygen therapy in various forms, although admission to intensive care units was similar in both the first (27%) and second waves (40%) of patients (23 %).
![Figure 3: Algorithm for the management of the COVID-19-positive kidney transplant recipient [48].](/fulltextimages/12845/fig_3.png)
(*Mild symptomatic patient has oxygenation saturation >95% without dyspnea. Moderately symptomatic patients show the presence of COVID-19 on imaging with oxygen saturation level >94% and respiratory rate is <30. Patients with low oxygen saturation <94%; respiratory rate >30 and require supplemental oxygen and mechanical ventilation are defined as a severely symptomatic patient; For patients who are at low risk of rejection, the physician can consider the discontinuation of Calcineurin inhibitor/mTORi; *Use of remdesivir can vary from country to country).
Supportive Treatment Recommendations for Patient Management and Monitoring
Information about the management of COVID-19 in post- transplant patients is very limited [26]. Organ transplant facilities should provide special care and monitoring to kidney transplant patients, as they are under maintenance on long-term immunosuppression therapy and are most likely to be infected by COVID-19 [31]. So, along with proper medication, kidney transplant patients with COVID-19 infection need some complementary treatment. They should be under continuous monitoring by a physician.
Isolation of patients: The first and foremost thing to do is to isolate the patients as they shed a high level of the virus from normal populations. Their isolation period can be longer than general populations and continuous testing at regular intervals may be needed for the assessment of viral clearance. This measure will be helpful for patients to be protected from further infectious attacks as well as prevent the spread of the virus among general populations.
Mechanical ventilation and supplemental oxygen: In case of severe respiratory symptoms, they should be supplied with supplemental oxygen through a nasal catheter considering the blood oxygen saturation level. Hospitalized patients with excessive lung involvement due to hyperinflammatory response, require mechanical ventilation [33]. For patients with an extremely low level of T-cell count and severe hypoxemia, non-inclusive ventilation, mechanical ventilation, and after that extracorporeal membrane oxygenation can be provided [26, 2]. Kidney International has published an article where the management of two series of kidney transplant patients has been discussed. Two out of seven patients were managed only on an outpatient basis and 5 were hospitalized. Among these 4 patients, three were admitted to the intensive care unit (ICU) and one died [5]. So, it gives an assurance that milder cases of COVID-19 in kidney transplant patients can be handled without any hospitalization. Another case report has also shown that patients without any major respiratory symptoms can be managed at home (22%). But for the hospitalized patient symptoms got worsened and required ongoing ventilation. So, the condition of hospitalized patients is more critical. About 78% of case patients get hospitalized.
Stabilizing endothelium dysfunction: As it has been found that, viral attack and its replication can cause endothelial dysfunction (Endotheliitis), stabilizing the endothelium can help to handle the severe cases including comorbidities in kidney transplant vulnerable patients (endothelial dysfunction). Anti-inflammatory, anti-cytokine, ACE inhibitors and statin classes of drugs can help in these cases. Intubation: Patients with a high level of IL-6, very low oxygen saturation (<94%), and high respiratory rate (>30) despite supplemental oxygen need intubation [48].
Renal replacement therapy: Renal replacement therapy which is a special kind of dialysis required for unstable ICU patients who have intolerance with regular dialysis is recommended in some case studies of COVID-19 in kidney transplant patients [16]. A study in New York, Bronx found that 23% of the hospitalized kidney transplant patients with COVID-19 required renal replacement therapy [48].
Normalizing D-dimer level: Patients with a high level of D-dimer protein (>3μg/dl) are treated with Apixaban [16]. This is an anticoagulant that prevents blood clots.
Patient education and telecommunication: Some basic patient education can ease the management of COVID-19 in kidney transplant patients. The patient should be made informed about potential risk factors comorbidities and immunosuppressive drugs. Telecommunications can help in this regard [19]. Dealing with drug-induced consequences: As ritonavir/ lopinavir and hydroxychloroquine have a tendency to prolong the cardiac QTc interval, the monitoring of prolongation should be carried out every 2 to 3-days basis. If the prolongation is noticed the dose reduction should be initiated [49].
Treatment of comorbidities If any kidney transplant patients use concomitant medication for other comorbidities like hypertension (Angiotensin-converting enzyme inhibitor or Angiotensin receptor blockers), a continuation of these co-medications has been recommended by the UK Renal Association and European Society of Cardiology [25].
Role of transplant disease infectious Disease (TID) physician to deal COVID-19 in kidney transplant patients
In this emerging COVID-19 pandemic, the role of TID is very crucial. He gathers information on experimental therapy and suggests them to immunocompromised kidney transplant patients. They assist other transplant physicians and coordinators. They help to develop screening strategies of COVID-19 in both donor and recipient. TID physicians try to optimize the overall transplantation procedure during the COVID-19 pandemic, provide updated educational tools and categorize transplant activities according to epidemiological risk factors of the pandemic [25].
Vaccination in Kidney Transplant Patients
Effectiveness of COVID-19 Vaccination in kidney transplant patients
To combat the injurious effect of SARS-Cov-2 and to minimize the intensity of critical illness, vaccination is very effective as it helps to develop adaptive immunity against this harmful virus [50]. But there are much evidence which have revealed weak antibody response after administration of the mRNA COVID-19 vaccine. However, some earlier studies have given information that the transplant patients who cannot produce adequate humoral immunity through the mRNA vaccine, may grow immunity through the development of cell-mediated immunity. So, it can be said that, although a kidney transplant patient does not show a detectable response after vaccination, this vaccination can decrease the severity of disease in patients [41, 51]. mRNA-based vaccines (Pfizer-BioNTech and Moderna) have been given priority for this special class of patient who shows severe illness [41]. and this vaccine helps to induce antibody response and the CD8 T-cell which kills the virus-infected cell [52]. This mRNA vaccine developed with 2 mutations in viral RNA can encode the full-length viral Spike-protein inside a vaccinated individual and produce neutralizing antibodies [50] (Table 2).
| for header rows | for data cells | for header rows | for data cells | |
|---|---|---|---|---|
| Serial No. | Author | No. of Subjects in Cohort | Response After Vaccination N (%) | |
| 1 | <50% after 1or2 dose of vaccine | |||
| 2 | 8 | 100% when vaccination is given after transplantation | ||
| 3 | 308 | 112(36.4%) after 28 days of 2nd dose of vaccine | ||
| 4 | 205 | 98(47.8%) after 2nd dose of vaccine | ||
| 5 | 61 | Spike-specific IgG seroconversion raised from 27(44.3%) after the second dose to 38(62.3%) after the third dose | ||
| 6 | 66 | circulating spike-specific CD4+ T cells and anti-RBD | ||
| 6 | 66 | IgG level raised to 28(42%) after 3rd dose specially in younger responders with lower baseline | ||
| 6 | 66 | creatinine level and patients who were less frequently exposed to mycophenolate mofetil | ||
| 7 | 242 | 26(10.8%) after 28 days of 1st dose and one had COVID-19 within 1 week after 1st dose of vaccine |
Table 2: Effectiveness of COVID-19 Vaccination.
But there is a scarcity of information about the efficiency of these newly invented vaccines in kidney transplant patients. Although International recommendations on COVID-19 vaccine distribution have given importance to immunocompromised patients, including kidney transplant recipients, they are excluded from the phase 3 clinical trial of vaccine development and initial vaccination guidelines have been developed without the inclusion of this class of people. As they cannot participate in any randomized controlled trial, prospective cohort studies are highly encouraged [41].
Influence of different classes of immunosuppressive drugs on the efficacy of the vaccine in kidney transplant patients
The probable reason for different antibody responses for vaccines in kidney transplant patients can be the use of immunosuppressants, such as T-cell depleting therapy or antimetabolites vaccination. Patients with a low dose of immunosuppressive drugs give a comparatively good response. So, it is considered that immunocompromised kidney transplant patients have comparatively less capability to produce neutralizing antibodies in their bodies after vaccination [50]. It can delay the induction of immune response after administration of the mRNA vaccine. Patients with kidney transplantation for a very long time, stable kidney function, and low immunosuppressant dose have displayed better responses to the vaccine. Just like the previously mentioned cohort study, patients under treatment of calcineurin inhibitor, MMF, and steroids have shown a relatively lower level of anti-SARS Cov-2 antibody in the titer test. And unfortunately, one patient was diagnosed with SARS-Cov-2 after 5 days of 2nd vaccination and his condition was severe. Patients who showed seroconversion had a long time from kidney transplantation, were using less immunosuppression and had a stable kidney function [51].
• Among different types of immunosuppressive drugs, anti-metabolite, Mycophenolate mofetil (MMF) has a higher tendency to interfere with the efficacy of the vaccine in kidney transplant patients. The response against the COVID-19 vaccine was found low who are taking MMF [53]. MMF inhibits the proliferation of CD4 T-helper cells which stimulate the differentiation of spike-specific B cell into an antibody-producing plasma cell [52]. MMF has a direct effect on B-cell activity and some studies have found that patients with a lower maintenance dose of MMF show a high response against SARS cov-2 after vaccination [50].
- A prospective cohort study has shown a more immune response towards the COVID-19 vaccine in patients who are using a low dose of different classes of immunosuppressive drugs [41].
- The use of Belatacept in some transplant patients has given poor outcomes for the vaccine.
- Corticosteroid does not affect the efficacy of the COVID-19 vaccine [50].
- Among Kidney transplant patients who use calcineurin inhibitors and show a high level of calcineurin inhibitor in their blood, display poor responsiveness towards vaccines with lower GFR levels. So, this might directly lower the predicted efficacy of the vaccine [50].
- Inhibitors can play a therapeutic role in SARS Cov-2 of kidney transplant patients by inhibiting cytokine storm. Besides they can cause downregulation of B and T lymphocytes which can interfere with the efficacy of vaccination. However, this information is conflicting as in a study with kidney transplant patients no alteration in vaccine efficacy was found due to regular use of mTOR-inhibitors [50]. So, more investigation is needed to establish this statement.
- Based on the commercial serological test, estimation of the amount of anti-spike protein IgG titer after 15 days of the last dose of vaccine in kidney transplant patients has shown a peak level of response which remains stable for at least 30 days. Follicular helper CD4 T (TFH) cell level can be an estimation of the efficacy of Covid vaccine but its measurement technique is very complex. Recently it has been found that, measuring the level of IFNγ by using IFNγ release assay, within 30 days of the last dose of vaccine, strongly correlates with the number of anti-spike specific TFH cells [52]. So, besides IgG titer estimation, this technique can also evaluate the efficacy of the vaccine in kidney transplant patients.
If we analyze the overall mechanism of impaired antibody production after the COVID-19 vaccine in kidney transplant patients, we found that corticosteroid, calcineurin inhibitors (tacrolimus, cyclosporin), mycophenolate mofetil, mechanistic target of rapamycin (mTOR) inhibitor suppresses the activity of T-cell which in turn down-regulate the production of anti-sars Cov-2 antibody by B-cell by a different mechanism. Thus, immunosuppressants influence the efficacy of the COVID-19 vaccine. These mechanisms are described in short by the following figure:
![Figure 4: Mechanism of impaired anti-SARAS Cov2 antibody response after vaccination in kidney transplant patients [43].](/fulltextimages/12845/fig_4.png)
Vaccination approach to enhance vaccine’s efficacy in kidney transplant patients
Vaccination against COVID-19 is an effective solution to protect the human body from the injurious effects and severity of coronavirus. So, this approach must be employed for kidney transplant patients as they are very prone to COVID-19 severity in a study, it has been found that the mRNA vaccine is capable of inducing a humoral response in only 37.5% of kidney transplant patient vaccine [50]. Recent
studies have recognized the importance of neutralizing antibodies (anti-spike IgG) in kidney transplant patients, as this can prevent viral entry by binding to the viral spike protein. Unlike the general population, only 4-48% of kidney transplant patients have become capable of producing this antibody after two doses of vaccination. If the recipient has no previous history of COVID-19 infection, they have a high possibility of growing anti-spike IgG in their body through vaccination after kidney transplantation. Even, vaccinated individuals also got infected severely which indicates the inefficiency of the vaccine and its standard dose in kidney transplant patients [52].
So, the vaccination regimen will be different for kidney transplant patients.46 But, before the administration of vaccines in kidney transplant patients, benefit-risk assessment in every organ transplant recipient is very important [50].
Administration of 2nd dose without delay: As kidney transplant patients are less responsive towards the COVID-19 vaccine, delay should not be allowed for the 2nd dose of vaccine in these immunocompromised patients, as this can increase the chance of being affected by COVID-19. Sometimes shortening the normal time interval between 1st and 2nd doses of vaccination has been suggested [51].
Selection of vaccination time: It has been suggested to give the vaccine before 2 weeks (at pre-transplant waiting period) and after 1-6 months of transplantation [50]. This timing of vaccination has been suggested to prevent the influence of immunosuppressive drugs on vaccine efficacy so that desired serological responses can be induced among these immunocompromised patients. A retrospective study at the Houston Methodist Hospital has found that vaccination before kidney transplantation can be beneficial as antibody response remains unaltered during post-transplantation periods vaccination. The time interval between doses has a known impact on vaccine immunogenicity and a 4- week interval between the second and third doses may be too short for vaccination.
Consideration of 3rd or 4th booster dose: To produce adequate adaptive immune response 3rd dose for the mRNA vaccine can be suggested as this is well tolerated by most kidney transplant patients in the world and can produce a sufficient amount of neutralizing antibodies. Determination of levels of anti-spike specific antibodies can help to decide for 3rd or 4th booster dose of mRNA vaccine [52]. Among Kidney transplant patients who give mild or less response after 1st dose of vaccine, vaccination with 3rd dose of mRNA vaccine should be taken under consideration for kidney transplant patients [51]. A third dose of the BNT162b2 vaccine increases both cross-variant neutralizing antibody and cellular (T-cell number and activity) responses in KT recipients with an acceptable tolerability profile.
Modification of dose of immunosuppressive drugs during vaccination: Similar to treatment approaches, modification of dose of immunosuppressive drugs during vaccination can help to enhance the efficacy of vaccination in kidney transplant patients. This can be either temporary discontinuation of MMF or belatacept replacement therapy [52]. Patients under low doses of immunosuppressive drugs can give a better response after the first dose of the mRNA vaccine by producing anti-SARS Cov-2 antibody in the body [51].
Sequential vaccination: Sequential administration of heterologous viral vaccines, such as mRNA vaccine followed by adjuvanted protein subunit or vice versa, can improve vaccine immunogenicity. Use of adjuvant for subunit vaccine: In cases of protein subunit vaccine, use of adjuvant (Windpessl et al., 2021), intradermal injection high antigen dose can increase seroconversion 491. This has not been proved for mRNA vaccines [52].
Simultaneous injection: The administration of a double dose which means two simultaneous injections instead of one can be another alternative solution to get the desired immune response by the vaccine, although this approach needs more research and controlled trial [41].
The following flowchart gives a guideline on the vaccination approach for COVID-19 in kidney transplant patients based on their previous history of COVID-19. Different vaccination algorithms have been suggested considering their history of previous viral infection and time of transplantation. During vaccination modification of the dose of immunosuppressive agents has also been suggested as they can influence the efficacy of vaccines. After 1st and 2nd doses of vaccination, the level of anti-spike IgG in the vaccinated individual has been determined to ensure the desired response of the vaccine against COVID-19. In case of low response, a third or fourth booster dose should be considered. This total scenario can be described by the following figure of a flowchart.
![Figure 5: Vaccination approach for kidney transplant recipients [52].](/fulltextimages/12845/fig_5.png)
Finally, more research and studies of COVID-19 vaccination, involving this special class of people can emerge a new evolution in vaccine development and can optimize the vaccination protocol for kidney transplant immunocompromised patients.
Management of Kidney Transplantation Program During COVID-19 Pandemic
Although kidney transplantation is a life-saving method for dialysis patients, conducting this complicated surgical procedure has become very difficult due to the safety issue in this pandemic [3].
![Figure 6: Factors affecCting kidney transplantation rates during COVID-19 [48].](/fulltextimages/12845/fig_6.png)
Nowadays, in many hospitals, there is a scarcity of resources (personnel, ICU bed-operating rooms, etc.) to conduct a kidney transplantation procedure as maximum physicians, nurses, and other medical personnel are busy treating the increasing number of COVID-19 patients. Besides, it has become very challenging to ensure a microbiologically safe environment in the hospital [3]. All of these things have made transplantation more complicated and have compelled many transplant facilities to stop or keep limiting their transplantation operation.
Therefore, kidney transplantation should be considered according to a case-by-case basis assessment of the severity of patients’ situation and known benefits and risks. If there is no alternative way to kidney transplantation, then the entire transplant team has to go for this task taking all necessary precautions. Some important matters should be considered in these cases such as optimized screening, proper utilization of healthcare resources, and proper planning and education by disseminating updated information about transplantation strategy should be considered [40]. Cautious and thoughtful selection of both the recipient’s and donor’s post-transplant management, risk assessment on the basis of the patient’s age and medical comorbidities, waitlist time, degree of sensitization, cold ischemia time, status of vaccination, and severity of pandemic in their region should be conducted.
Priority-based kidney transplantation
The European Association of urology has declared that deceased donor kidney transplantation can be done without delay in this pandemic. But in cases of living donors, it should be delayed to reserve resources [54]. On the other hand, non-urgent and deceased donor transplantation has been discouraged in communities with a high prevalence of COVID-19 infection. United has also planned to stop living donor transplantation and is discussing postponing deceased donor kidney transplantation during the COVID-19 outbreak [25]. So, there is no fixed rule of the transplantation program. Every community is conducting it by understanding the priority, situation, and availability of resources in this epidemic condition and the severity of patients after postponing transplantation [40].
According to the Korean Transplantation Society, South Korea carried out extensive virus testing by real-time RT-PCR test in both donor and recipient. They include contact tracing in their diagnosis schedule. Since delaying or disqualifying transplantation can be more harmful and injurious for end- stage kidney disease patients and they are unable to maintain social distancing due to continuous visits to dialysis centers, the national kidney transplantation program in South Korea remained active to some extent considering the benefit- risk ratio and current medical condition of kidney function compromised patients [55]. Observing the data of several kidney transplantations in South Korea, it can be seen that they increased their overall kidney transplantation activities from April 2019 to April 2020 in the case of deceased donor kidney transplantation, although living donor transplantation has been decreased.
Unlike the Korean transplantation society, the United Kingdom discourages kidney transplantation where induction therapy is required by using anti-thymocyte globulin or alemtuzumab. Because lymphocyte depleting antibodies can increase the risk severity of COVID-19 besides these [56], they have emphasized testing for deceased donors and discouraged transplantation in old and comorbid patients especially with diabetes this COVID-19 period [25].
Appropriate timing of transplantation
According to a cohort study in the UK, 2 out of 7 kidney transplant patients had their kidney transplantation within 3 months of the pandemic declaration (2019) and these patients showed severity in symptoms. So, transplantation timing is also important as within the first 3 months of transplantation COVID-19 symptoms can be deteriorated more as this time they are at a high dose of immunosuppressive drugs [5]. This is another reason for postponing kidney transplantation during this critical situation.
Transplantation in older patients with comorbidities
Transplantation in older patients and patients with several comorbidities especially with Diabetes mellitus has been discouraged in different transplantation centers in united-kingdom [25].
Screening of donor and recipient of kidney transplantation
There is a theoretical idea that COVID-19-positive donors can transfer this RNA virus into the recipients, although very little information has been gathered regarding this matter [20]. However the exposure of donors to COVID-19 patients or areas, asymptomatic donors, viremia, presence of the virus within specific blood or organ compartments can influence the donor-derived transmission of COVID-19. This can be a reason for halting transplantation programs where this virus has spread extensively [20] (Table 3).
So, for safety, it is compulsory to do a test for both donor and recipient for COVID-19. Due to the limited accuracy and sensitivity of the RT-PCR test, both donor and recipient may be identified as COVID-19 negative while they have already been infected. RT-PCR test with bronchoalveolar lavages of a donor can minimize this accuracy problem. But it is not applicable for recipients [31].This is very important before conducting any surgical procedure of kidney transplantation. Nowadays, screening has added another feature in terms of detecting the presence of coronavirus.
| Country | Deceased Donor Transplantation | Living Donor Transplantation | Pre-transplant Recipient Screening | Specimen Type | |
|---|---|---|---|---|---|
| Canada | Universal NAT | Universal NAT | Clinical | NP or BAL | |
| Switzerland | Universal NAT | Universal NAT | Clinical | NP or BAL | |
| Italy | Universal NAT | Universal NAT | Clinical | BAL in deceased donor NP in living donor | |
| Spain | Universal NAT | Universal NAT | Clinical | NP±BAL | |
| Korea | Universal NAT | Universal NAT | Universal NAT | NP | |
| Japan | Risk-based NAT due to limited testing capacity | Self-isolation or hospital admission 14 days before surgery | Clinical; NAT where testing available | NP (and BAL for intubated patients) |
Table 3: Summary of donor and recipient screening practices.
BAL- Broncho Alveolar Lavage; NAT- Nucleic Acid Testing; NP-Naso-pharyngeal Table 3: Summary of donor and recipient screening practices.
Donor screening: According to the Italian Transplant Authority, primarily RT-PCR test using a nasopharyngeal swab or bronchoalveolar lavages is used to detect the infection of coronavirus [31] .In this case, a known and suspected donor, with active COVID-19 in terms of exposure in the highly infected region, symptoms, and a chest x-ray should be disqualified for kidney donation in 2019. US-FDA has suggested considering the travel history of the donor to the epidemic area, contact with COVID-19 patients, and suspected infection with COVID-19 before 28 days of kidney donation [31].
For the deceased donor, the RT-PCR test should be performed by the sample from the upper respiratory tract. According to the American Society of transplantation, if any living donor is identified as a COVID-19 positive patient then he should wait for at least 28 days from the time of diagnosis and recovery of symptoms.
Recipient or candidate screening: Recipients are also screened through history, chest radiography, computed tomography, RT-PCR, and other microbiological tests. If test results come COVID-19, then recipients cannot go for kidney transplantation and have to wait until the 2 RT-PCR tests come out negative and symptoms disappear.
Safety concerns about the transplant team
The entire team has to discuss the pros and cons of transplantation. The safety of the transplantation team is also very important as they can also be infected by the high viral shedding of kidney transplant patients.26 In case of safety concerns transplantation team should be careful about the following factors:
- Traveling off the team for donor procurement in high- risk areas of COVID-19.
- Carrying out any sensitive and high-risk procedures on the deceased donor.
- Dealing with recipients with a high probability of viral shedding.
- In this case, team members should use personal protective equipment. In addition any team member with symptoms of COVID-19 should be discarded from the team until full recovery [40].
Telecommunications service kidney transplant patients with COVID-19
During the COVID-19 pandemic, many countries’ transplantation facilities face a challenge to performing transplantation activity and provide any post-transplantation outpatient services. So, they had no other way to limit their regular transplantation activities. But French government’s medical and non-medical staff of kidney transplant area has uniquely handled this situation. They direct a kidney transplantation survey and telemedicine consultation program which not only minimizes the chance of transmission of COVID-19 inside the hospital but also maximizes the observation or follow-up and detection of COVID-19 in kidney transplant patients [19]. So, this is an appreciating effort conducted for kidney transplant patients.
Taking Informed Consent
Informed consent should be taken from the patient and his or her family member to make any decision regarding this issue [3].
Collaborative Working
The kidney transplantation center in collaboration with local infectious disease specialists and infection prevention professionals should gather knowledge to protect kidney transplant patients from COVID-19 [20].
Discussion
The whole world is facing a critical situation due to the ongoing pandemic. However, information about COVID-19 in kidney transplant patients is limited, incomplete, and unfixed. Various factors such as signs and symptoms, treatment approaches, vaccination guidelines, the effect of immunosuppressive drugs on COVID-19 severity, and comorbidities require extensive analysis, study, and research to gather enough knowledge in this sector. COVID-19 symptoms in kidney transplant patients can be delayed due to the effect of immunosuppressants, making diagnosis difficult. As a result, their condition can worsen, leading to a higher mortality rate compared to the general population. Therefore, an individualized approach is recommended, as there is a variety of symptoms and severity of COVID-19 in kidney transplant patients, and their regular immunosuppressants also vary from person to person. While dose reduction of immunosuppressive drugs has been suggested in most COVID-19 cases in kidney transplant patients due to their defective effect on the host immune response, there are also exceptional case reports where a conventional immunosuppressive dose has been maintained during COVID-19 treatment, resulting in full recovery of patients. Some evidence has shown the presence of anti- SARS CoV-2 antibodies in kidney transplant patients after about 15 days of COVID-19 disease, similar to that produced after vaccination. However, the use of immunosuppressive drugs interferes with the efficacy of the vaccine in kidney transplant patients. As a result, specialists have to plan for optimized vaccination procedures in kidney transplant patients, as information regarding appropriate vaccination procedures and their efficacy in kidney transplant patients is scarce, and they have no validity to be a part of the clinical trial. Prospective and retrospective cohort studies are the only way to define vaccination criteria. The diagnosis of asymptomatic recipients is also important, as excluding these asymptomatic patients can lead to an underestimation of any measurement [57]. For enhancing clarity and illustration in kidney transplantation management during the COVID-19 pandemic should follow the following.
Impact of COVID-19 on Kidney Transplantation
Understanding the Disruption: Assessing the immediate and long-term effects of the COVID-19 pandemic on kidney transplantation programs, including donor availability, transplant surgeries, and post-transplant care.
Case Study: Navigating Transplant Delays: Examining a case where a patient experienced delays in transplant surgery due to pandemic-related restrictions and exploring strategies employed to mitigate the impact on clinical outcomes.
Adapting Transplant Protocols and Practices
Implementing Safety Measures: Detailing the adjustments made to transplant protocols to ensure the safety of transplant recipients, donors, and healthcare staff during the pandemic, such as pre-transplant screening, testing, and infection control measures.
Case Study: Virtual Consultations and Telemedicine: Illustrating how telemedicine and virtual consultations have been utilized to facilitate pre- and post-transplant evaluations, patient education, and follow-up care, with a focus on improving accessibility and minimizing exposure risks.
Managing Immunosuppression in the Context of COVID-19
Balancing Risks and Benefits: Discussing the challenges of managing immunosuppressive therapies in transplant recipients amidst the COVID-19 pandemic, including the risk of viral infection versus the risk of allograft rejection.
Case Study: Individualized Immunosuppression Strategies: Presenting a case where immunosuppressive regimens were tailored based on patient-specific factors, comorbidities, and local epidemiological considerations to optimize graft outcomes while minimizing infectious risks.
Patient Education and Support
Empowering Patients: Highlighting the importance of patient education and support in navigating the uncertainties and complexities of kidney transplantation during the pandemic, including adherence to preventive measures, self- care practices, and mental health support.
Case Study: Virtual Support Groups and Resources: Demonstrating the utilization of virtual support groups, educational materials, and online resources to connect transplant recipients with peers, caregivers, and healthcare providers for mutual support and information sharing.
Future Directions and Lessons Learned
Preparing for Future Challenges: Identifying areas for improvement and lessons learned from the pandemic experience to enhance the resilience and preparedness of kidney transplantation programs for future infectious disease outbreaks or public health emergencies.
Case Study: Building Resilience through Collaborative Efforts: Showcasing collaborative efforts among transplant centers, healthcare systems, governmental agencies, and professional organizations to develop and implement evidence-based guidelines, protocols, and contingency plans for pandemic response and recovery.
By structuring the discussion with clear headings and incorporating specific examples and case studies, readers can better understand the challenges, strategies, and lessons learned in kidney transplantation management during the COVID-19 pandemic. These illustrative narratives provide valuable insights into real-world experiences and serve as practical guides for clinicians, researchers, and policymakers involved in transplant care and pandemic preparedness [58, 59].
Conclusion
The COVID-19 pandemic has severely impacted kidney transplant patients, who are highly vulnerable to the virus due to their weakened immune systems. Managing these patients during the pandemic presents significant challenges for healthcare professionals. Treatment approaches include adjusting immunosuppressive medications, antiviral therapy, and supportive care based on symptom severity. While the COVID-19 vaccine offers hope, its effectiveness is reduced in these patients. More research is urgently needed to develop effective treatment strategies and minimize the suffering of kidney transplant recipients during this pandemic. In conclusion, the review underscores the profound impact of COVID-19 infection on kidney transplant patients and the intricate challenges faced by transplant programs worldwide. To address the gaps identified in this discussion and improve the resilience of kidney transplantation management in the face of future pandemics, several recommendations and areas for future research emerge: Enhanced Surveillance and Preparedness: Implementing robust surveillance systems to monitor transplant outcomes, infectious risks, and healthcare disparities among vulnerable patient populations. Investing in pandemic preparedness plans tailored to the unique needs of transplant recipients and healthcare systems can mitigate the impact of future outbreaks. Optimization of Telemedicine and Digital Health Solutions: Expanding the integration of telemedicine and digital health technologies into kidney transplant care to improve access, continuity, and quality of care. Leveraging virtual platforms for pre-transplant evaluations, post-transplant monitoring, patient education, and psychosocial support can enhance patient outcomes and reduce healthcare disparities. Tailored Immunomodulatory Strategies: Advancing personalized immunosuppressive regimens and infection prophylaxis protocols based on patient-specific factors, including age, comorbidities, immunological status, and local epidemiological trends. Optimizing the balance between immunosuppression and infection risk mitigation is critical to preserving graft function and minimizing morbidity and mortality in transplant recipients. Multidisciplinary Collaboration and Knowledge Exchange: Fostering interdisciplinary collaboration among transplant specialists, infectious disease experts, public health officials, and patient advocacy groups to share best practices, guidelines, and research findings. Promoting knowledge exchange and capacity-building initiatives can enhance the collective response to future pandemics and improve patient outcomes on a global scale. Policy Advocacy and Resource Allocation: Advocating for policy changes and resource allocation to address systemic barriers and disparities in access to kidney transplantation care, including disparities in vaccination coverage, healthcare infrastructure, and socioeconomic support. Prioritizing equity-driven policies and interventions can mitigate the disproportionate impact of pandemics on marginalized communities and enhance health equity in transplant care delivery. By heeding these recommendations and fostering collaboration across disciplines, healthcare systems, and policymakers, the transplant community can mitigate the impact of COVID-19 and other infectious threats on kidney transplant patients. This review emphasizes the urgent need for proactive measures, innovative strategies, and collective action to safeguard the health and well-being of transplant recipients and optimize transplant outcomes in the era of COVID-19 and beyond.
References
-
Gustine JN, Jones D (2021) Immunopathology of Hyperinflammation in COVID-19. Am J Pathol 191(1): 4-17.
-
National Kidney Foundation (2021) Kidney disease & COVID-19.
-
Martino F, Plebani M, Ronco C (2020) Kidney transplant programmes during the COVID-19 pandemic. Lancet Respir Med 8(5): e39.
-
Ahmadpoor P, Rostaing L (2020) Why the immune system fails to mount an adaptive immune response to a COVID‐19 infection. Transpl Int 33(7): 824-825.
-
Coates PT, Wong G, Drueke T, Rovin B, Ronco P (2020) Early experience with COVID-19 in kidney transplantation. Kidney Int 97(6): 1074-1075.
-
Vinson AJ, Kiberd BA, Tennankore KK (2021) Panic in the Pandemic: When Should Kidney Transplant Programs Close? Kidney Int Reports 6(5): 1232-1241.
-
Chen TK, Knicely DH, Grams ME (2019) Chronic kidney disease diagnosis and management: a review. Jama 322(13): 1294-1304.
-
Vidas MM, Rubio EM, Quiroga B, Montejano R, Morales E, et al. (2024) Strategies for prevention and treatment of SARS-COV-2 infection in patients with chronic kidney disease: Literature review. Nefrologia (Engl Ed) 44(2): 150-158.
-
Goswami S, Bakshi UG, Bhattacharya S (2022) COVID-19 and SARS-CoV-2: The Science and Clinical Application of Conventional and Complementary Treatments. 1st (Edn.), Boca Raton, CRC Press, pp: 12.
-
(2023) SARS-CoV-2 Variant Classifications and Definitions. CDC Covid-19.
-
DeGrace MM, Ghedin E, Frieman MB, Krammer F, Grifoni A, et al. (2022) Defining the risk of SARS-CoV-2 variants on immune protection. Nature 605(7911): 640-652.
-
Gibertoni D, Reno C, Rucci P, Fantini MP, Buscaroli A, et al. (2021) COVID-19 incidence and mortality in non- dialysis chronic kidney disease patients. PLoS One 16(7): e0254525.
-
Fishman JA, Grossi PA (2020) Novel Coronavirus‐19 (COVID‐19) in the immunocompromised transplant recipient: #Flatteningthecurve. Am J Transplant 20(7): 1765-1767.
-
Mamode N, Ahmed Z, Jones G, Banga N, Motallebzadeh R, et al. (2021) Mortality Rates in Transplant Recipients and Transplantation Candidates in a High-prevalence COVID-19 Environment. Transplantation 105(1): 212- 215.
-
Campise M, Alfieri CM, Perego M, Tamborini F, Cresseri D, et al. (2021) COVID-19 Infection in Kidney Transplant Patients: An Italian One Year Single Centre Experience. Journal of the American Society of Nephrology 32(10s): 639.
-
Akalin E, Azzi Y, Bartash R, Seethamraju H, Parides M, et al. (2020) Covid-19 and Kidney Transplantation. N Engl J Med 382(25): 2475-2477.
-
Wang J, Li X, Cao G, Wu X, Wang Z, et al. (2020) COVID-19 in a Kidney Transplant Patient. Eur Urol 77(6): 769-770.
-
Guillen E, Pineiro GJ, Revuelta I, Rodriguez D, Bodro M, et al. (2020) Case report of COVID‐19 in a kidney transplant recipient: Does immunosuppression alter the clinical presentation? Am J Transplant 20(7): 1875-1878.
-
Elias M, Pievani D, Randoux C, Louis K, Denis B, et al. (2020) COVID-19 Infection in Kidney Transplant Recipients: Disease Incidence and Clinical Outcomes. J Am Soc Nephrol 31(10): 2413-2423.
-
Lopez V, Vazquez T, Alonso-Titos J, Cabello M, Alonso A, et al. (2020) Recommendations on management of the SARS-CoV-2 coronavirus pandemic (Covid-19) in kidney transplant patients. Nefrologia 40(3): 265-271.
-
Pepys MB (2021) C-reactive protein predicts outcome in COVID-19: is it also a therapeutic target? Eur Heart J 42(23): 2280-2283.
-
Yu HH, Qin C, Chen M, Wang W, Tian DS (2020) D-dimer level is associated with the severity of COVID-19. Thromb Res 195: 219-225.
-
Vargas-Vargas M, Cortes-Rojo C (2020) Ferritin levels and COVID-19. Rev Panam Salud Pública 44: e72.
-
Chen G, Li X, Gong Z, Xia H, Wang Y, et al. (2021) Hypertension as a sequela in patients of SARS-CoV-2 infection. PLoS One 16(4): e0250815.
-
Banerjee D, Popoola J, Shah S, Ster IC, Quan V, et al. (2020) COVID-19 infection in kidney transplant recipients. Kidney Int 97(6): 1076-1082.
-
Huang J, Lin H, Wu Y, Fang Y, Kumar R, et al. (2020) COVID‐19 in posttransplant patients-report of 2 cases. Am J Transplant 20(7): 1879-1881.
-
Nair V, Jandovitz N, Hirsch JS, Nair G, Abate M, et al. (2020) COVID‐19 in kidney transplant recipients. Am J Transplant 20(7): 1941-1943.
-
Azzi Y, Parides M, Alani O, Loarte-Campos P, Bartash R, et al. (2020) COVID-19 infection in kidney transplant recipients at the epicenter of pandemics. Kidney Int 98(6): 1559-1567.
-
Bartiromo M, Borchi B, Botta A, Bagalà A, Lugli G, et al. (2020) Threatening drug‐drug interaction in a kidney transplant patient with coronavirus disease 2019 (COVID‐19). Transpl Infect Dis 22(4): e13286.
-
Zhang H, Chen Y, Yuan Q, Xia Q-X, Zeng X-P et al. (2020) Identification of Kidney Transplant Recipients with Coronavirus Disease 2019. Eur Urol 77(6):742-747.
-
Puliatti S, Eissa A, Eissa R, et al. (2020) COVID-19 and urology: a comprehensive review of the literature. BJU Int 125(6): E7-E14.
-
Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, et al. (2020) Endothelial cell infection and endotheliitis in COVID-19. Lancet 395(10234): 1417-1418.
-
Alberici F, Delbarba E, Manenti C, Econimo L, Valerio F, et al. (2020) Management of Patients on Dialysis and With Kidney Transplantation During the SARS-CoV-2 (COVID-19) Pandemic in Brescia, Italy. Kidney Int Reports 5(5): 580-585.
-
Boppana U, Leonard TS, Jolayemi A, Ansari MI, Salib A, et al. (2023) Drug-Drug Interactions Between COVID-19 Treatments and Psychotropic Medications: An Updated Study. Cureus 15(12): e50469.
-
Foy M, Sperati CJ, Lucas GM, Estrella MM (2014) Drug interactions and antiretroviral drug monitoring. Current HIV/AIDS Reports 11(3): 212-222.
-
Dickinson L, Khoo S, Back D (2010) Pharmacokinetics and drug–drug interactions of antiretrovirals: an update. Antiviral research 85(1): 176-189.
-
Bennett D, Franchi F, De Vita E, Mazzei MA, Volterrani L, et al. (2021) SARS-CoV-2 in pleural fluid in a kidney transplant patient. Postgrad Med 133(5): 540-543.
-
Trujillo H, Fernández‐Ruiz M, Gutiérrez E, Sevillano Á, Caravaca-Fontán F, et al. (2021) Invasive pulmonary aspergillosis associated with COVID‐19 in a kidney transplant recipient. Transpl Infect Dis 23(2): e13501.
-
Kumar D, Manuel O, Natori Y, Egawa H, Grossi P, et al. (2020) COVID‐19: A global transplant perspective on successfully navigating a pandemic. Am J Transplant 20(7): 1773-1779.
-
Rozen-Zvi B, Yahav D, Agur T, et al. (2021) Antibody response to SARS-CoV-2 mRNA vaccine among kidney transplant recipients: a prospective cohort study. Clin Microbiol Infect 27(8): 1173-1173.
-
Marx D, Moulin B, Fafi‐Kremer S, Benotmane I, Gautier G, et al. (2020) First case of COVID‐19 in a kidney transplant recipient treated with belatacept. Am J Transplant 20(7): 1944-1946.
-
Fontana F, Alfano G, Mori G, Amurri A, Tei L, et al. (2020) COVID‐19 pneumonia in a kidney transplant recipient successfully treated with tocilizumab and hydroxychloroquine. Am J Transplant 20(7): 1902-1906.
-
Agresti N, Lalezari JP, Amodeo PP, Mody K, Mosher SF, et al. (2021) Disruption of CCR5 signaling to treat COVID-19-associated cytokine storm: Case series of four critically ill patients treated with leronlimab. J Transl Autoimmun 4: 100083.
-
Pereira MR, Mohan S, Cohen DJ, Husain SA, Dube GK, et al. (2020) COVID‐19 in solid organ transplant recipients: Initial report from the US epicenter. Am J Transplant 20(7): 1800-1808.
-
Kemmner S, Guba MO, Schönermarck U, Stangl M, Fischereder M, et al. (2020) Cyclosporine as a preferred calcineurin inhibitor in renal allograft recipients with COVID-19 infection. Kidney Int 98(2): 507-508.
-
Xu Z, Shi L, Wang Y, Zhang J, Huang L, et al. (2020) Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med 8(4): 420-422.
-
Khairallah P, Aggarwal N, Awan AA, Vangala C, Airy M, et al. (2021) The impact of COVID‐19 on kidney transplantation and the kidney transplant recipient – One year into the pandemic. Transpl Int 34(4): 612-621.
-
Alberici F, Delbarba E, Manenti C, Econimo L, Valerio F, et al. (2020) A single center observational study of the clinical characteristics and short-term outcome of 20 kidney transplant patients admitted for SARS-CoV2 pneumonia. Kidney Int 97(6): 1083-1088.
-
Hou YC, Lu KC, Kuo KL (2021) The Efficacy of COVID-19 Vaccines in Chronic Kidney Disease and Kidney Transplantation Patients: A Narrative Review. Vaccines 9(8): 885.
-
Benotmane I, Gautier-Vargas G, Cognard N, Olagne J, Heibel F, et al. (2021) Weak anti–SARS-CoV-2 antibody response after the first injection of an mRNA COVID-19 vaccine in kidney transplant recipients. Kidney Int 99(6): 1487-1489.
-
Caillard S, Thaunat O (2021) COVID-19 vaccination in kidney transplant recipients. Nat Rev Nephrol 17(12): 785-787.
-
Windpessl M, Bruchfeld A, Anders HJ, Kramer H, Waldman M, et al. (2021) COVID-19 vaccines and kidney disease. Nat Rev Nephrol 17(5): 291-293.
-
Stensland KD, Morgan TM, Moinzadeh A, Lee CT, Briganti A, et al. (2020) Considerations in the Triage of Urologic Surgeries During the COVID-19 Pandemic. Eur Urol 77(6): 663-666.
-
Lee J, Huh KH (2020) Kidney transplantation trends in South Korea during the COVID-19 pandemic. Kidney Int 98(2): 512-513.
-
Hezer B, Massey EK, Reinders ME, Tielen M, Wetering J, et al. (2024) Telemedicine for Kidney Transplant Recipients: Current State, Advantages, and Barriers. Transplantation 108(2): 409-420.
-
Webb C, Davidson B, Jones ESW, Wearne N, Chetty DR, et al. (2021) COVID-19–Associated Graft Loss From Renal Infarction in a Kidney Transplant Recipient. Kidney Int Reports 6(4): 1166-1169.
-
Bevilacqua M, Chiu H, Melnyk Y, Williams J, Chohan R, et al. (2022) Protocol for a multistage mixed-methods evaluation of multidisciplinary chronic kidney disease care quality following integration of virtual and in-person care during the COVID-19 pandemic. Canadian Journal of Kidney Health and Disease 9: 20543581221103103.
-
Chattu VK, Mol R, Singh B, Reddy KS, Hatefi A, et al. (2024) Pandemic treaty as an instrument to strengthen global health security: Global health diplomacy at its crux. Health Promotion Perspectives 14(1): 9-18.
-
DeFelice G, Vijay A (2022) Coronavirus-19 infection in kidney transplant recipients: A comprehensive review. Indian J Urol 38(2): 110-114.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study